
Jung-Min Ahn, MD
Asan Medical Center, Republic of Korea
Jung-Min Ahn, MD (Asan Medical Center, Korea) showed the relationship between Left Anterior Descending (LAD) and Left Circumflex (LCX) depending on new criteria describing how to optimize two stents for Left-Main (LM) bifurcation stenting technique.
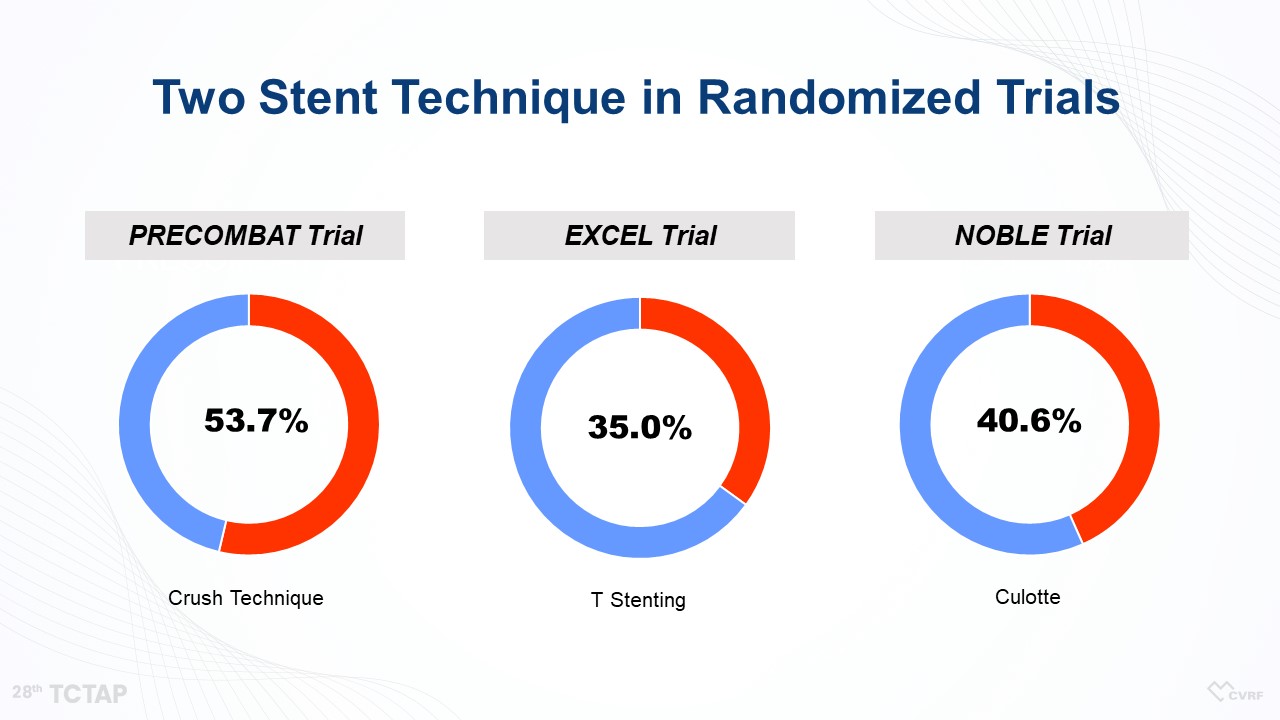
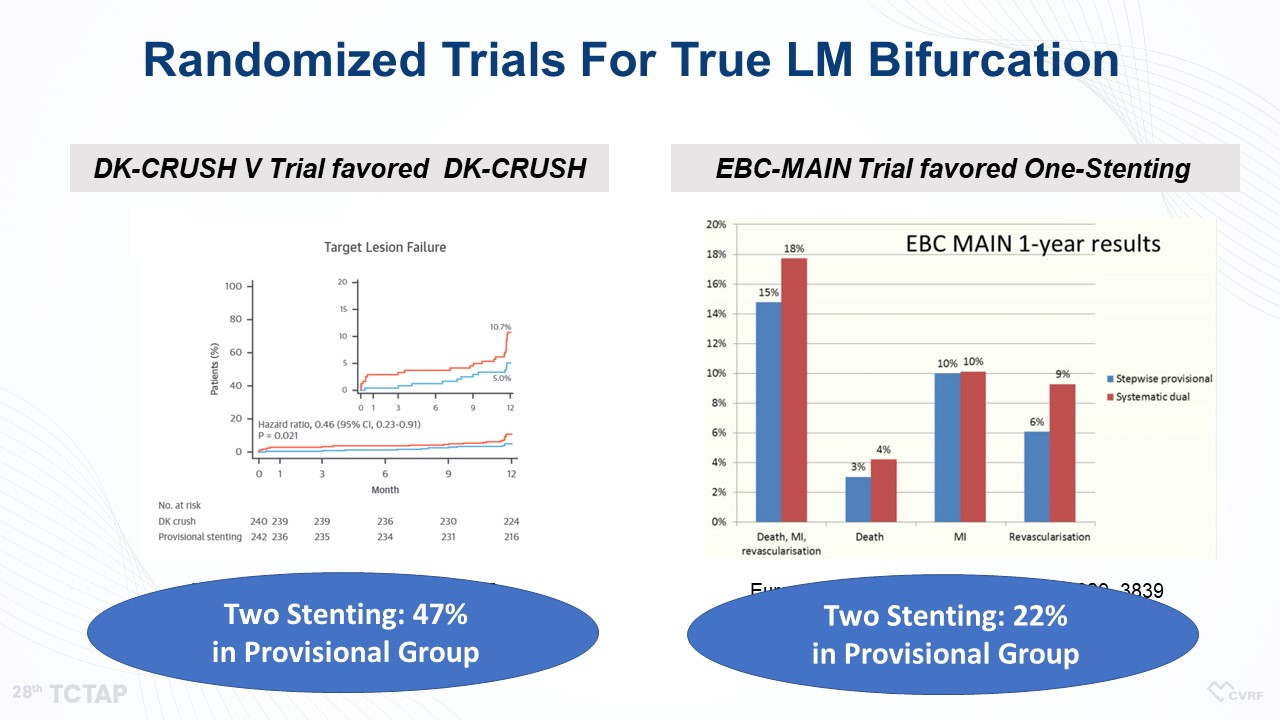
For the bifurcation lesion of left main coronary artery disease (LMCAD), a simple crossover of the LM to LAD artery has been considered as a default strategy. “However, there are many cases we cannot avoid two-stenting at bifurcation lesions,” Ahn said . Actually, in many trials about LMCAD including the PRECOMBAT, EXCEL, and NOBLE trials, more than one-third to up to half of patients received the two-stent technique (Figure 1). Even in the EBC-MAIN trial, which favored one-stenting, about 22% of patients in the provisional stenting group received two-stenting (Figure 2). Therefore, we should know how to optimize two stents for LM bifurcation stenting technique to improve the clinical outcomes of patients with LMCAD.
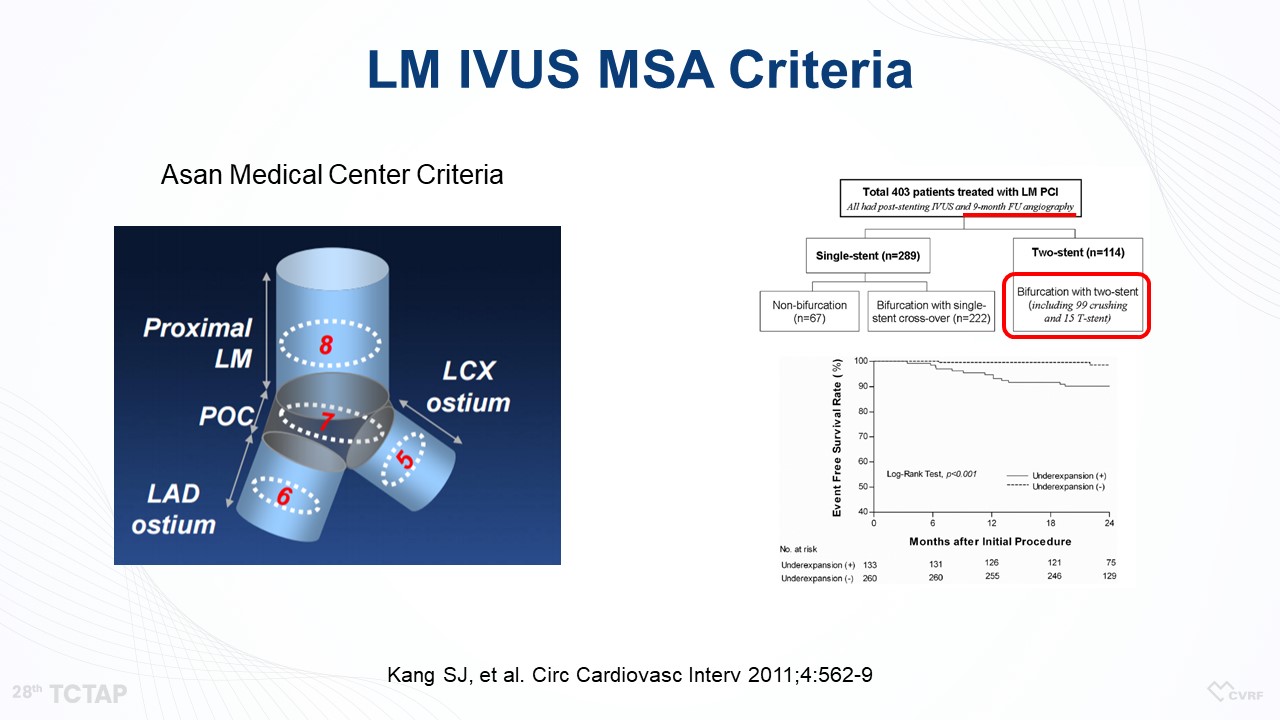
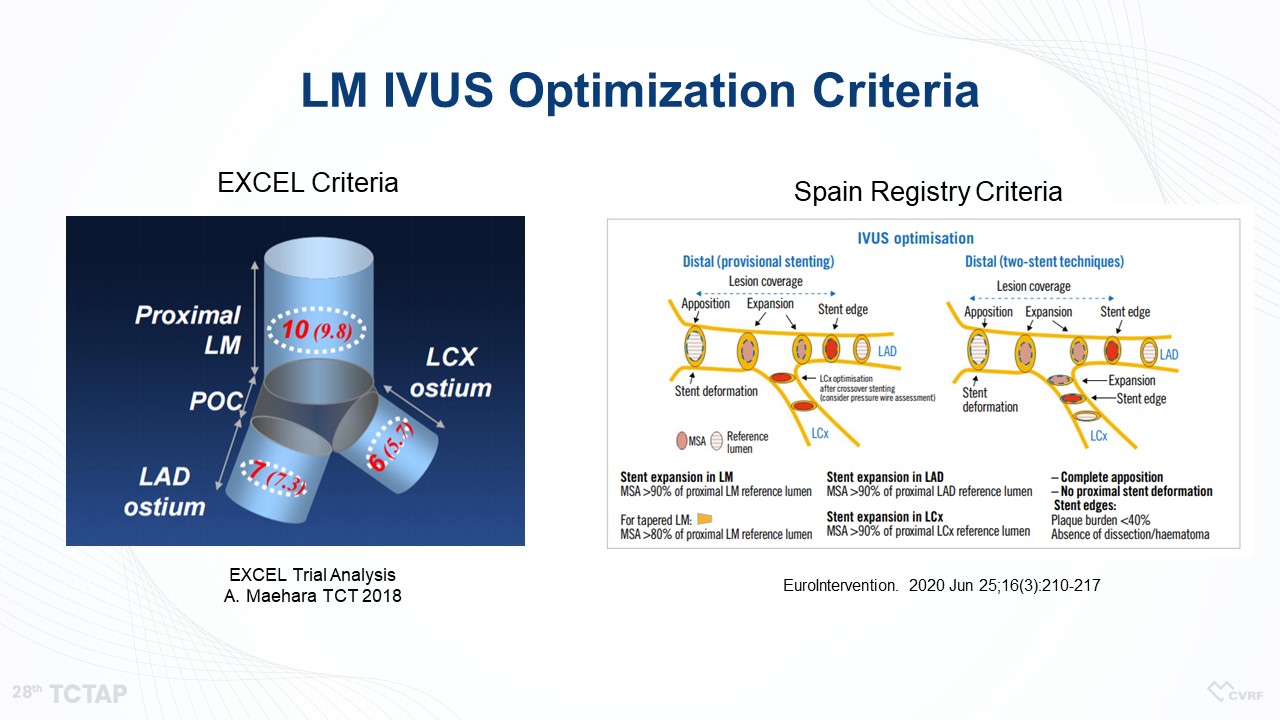
In 2011, Kang et al. reported LM intravascular ultrasound (IVUS) minimal stent area (MSA) criteria based on the result of a total of 403 patients treated with LM percutaneous coronary intervention (PCI) (Figure 3). However, the previous study included a heterogeneous group of patients, and therefore, we needed specific MSA criteria for the LM crush technique based on the long-term follow-up data. Also, the EXCEL and Spain Registry Criteria suggested a bigger MSA compared with the LM IVUS MSA criteria.
“So, we needed new MSA criteria for the LM crush technique,” Ahn said (Figure 4).
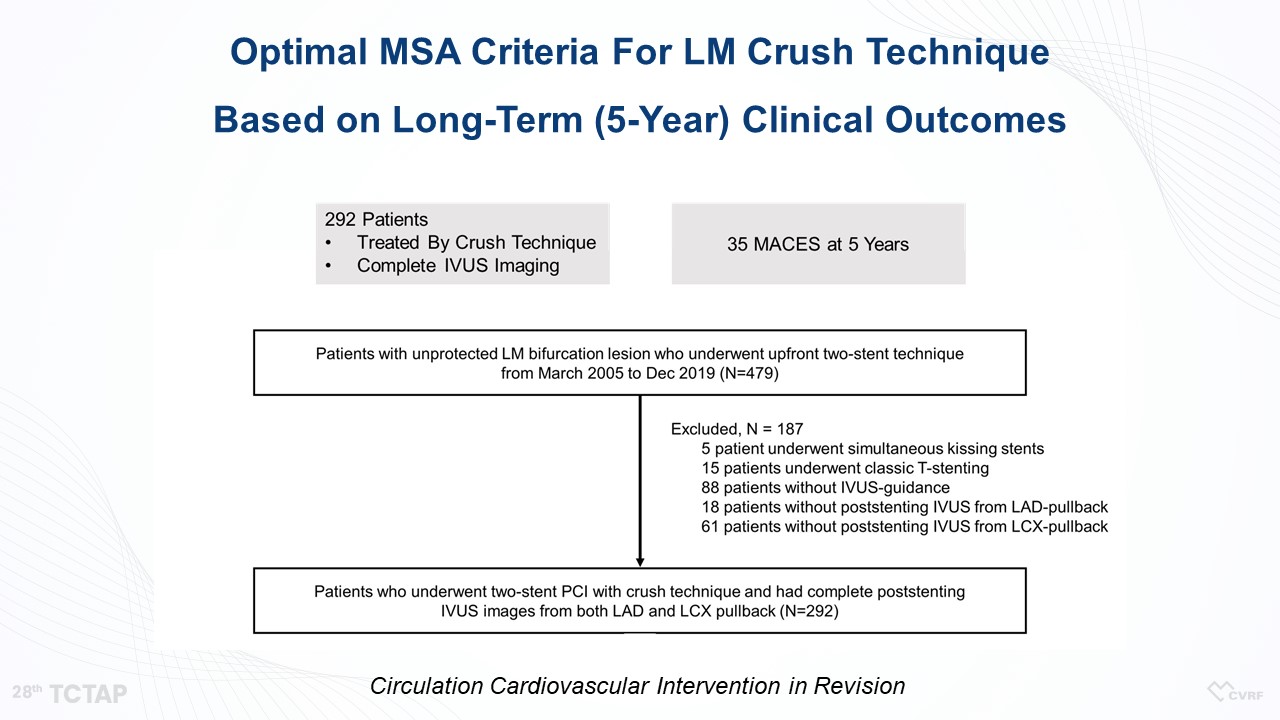
“We included a total of 292 patients with unprotected LMCAD treated with crush technique who had completed post-stenting IVUS and analyzed a major adverse cardiovascular event (MACE), a composite of death, myocardial infarction, or repeat revascularization (Figure 5).”
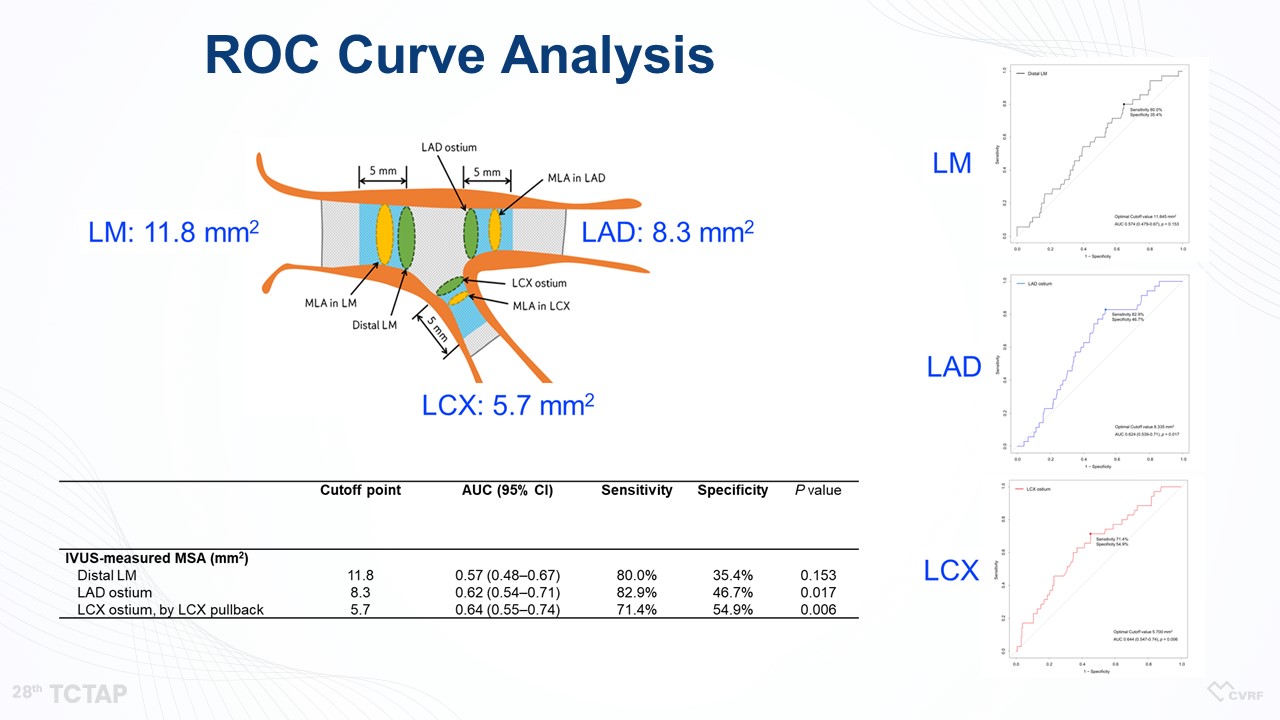
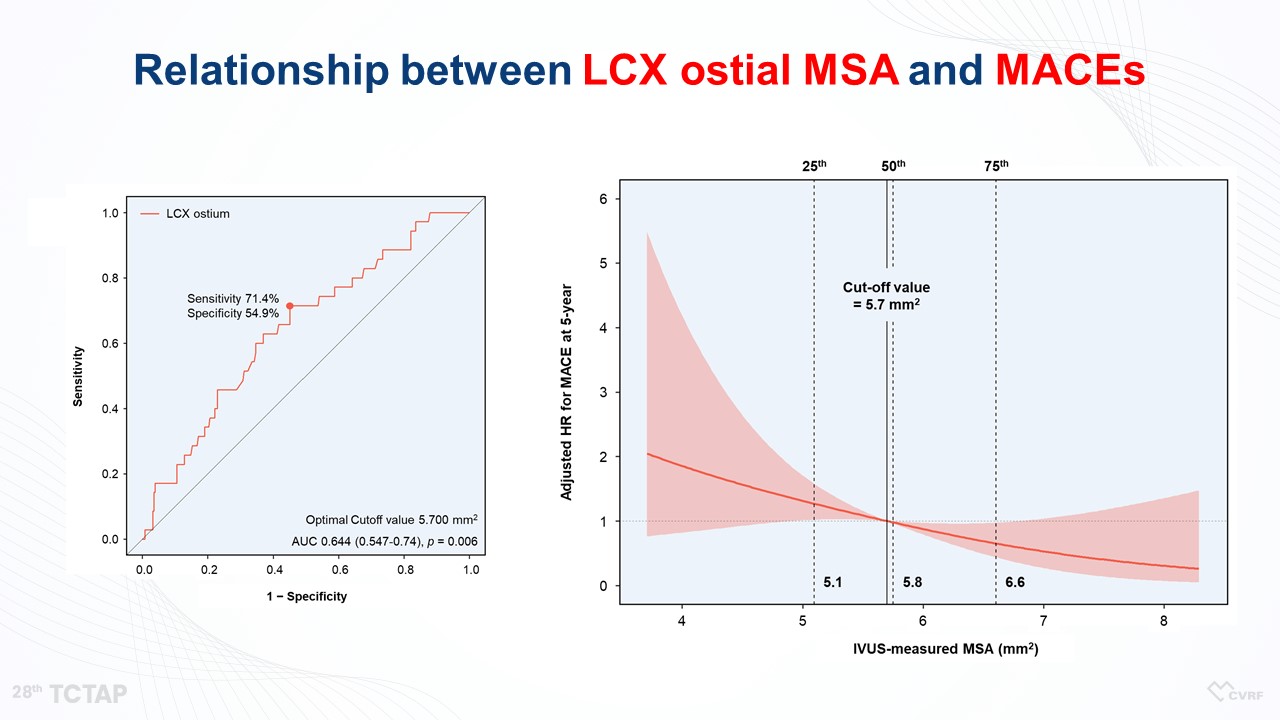
“Based on the 5-year MACE outcomes, we determined the best cut-off value to predict the 5-year clinical outcomes,” he said (Figure 6).
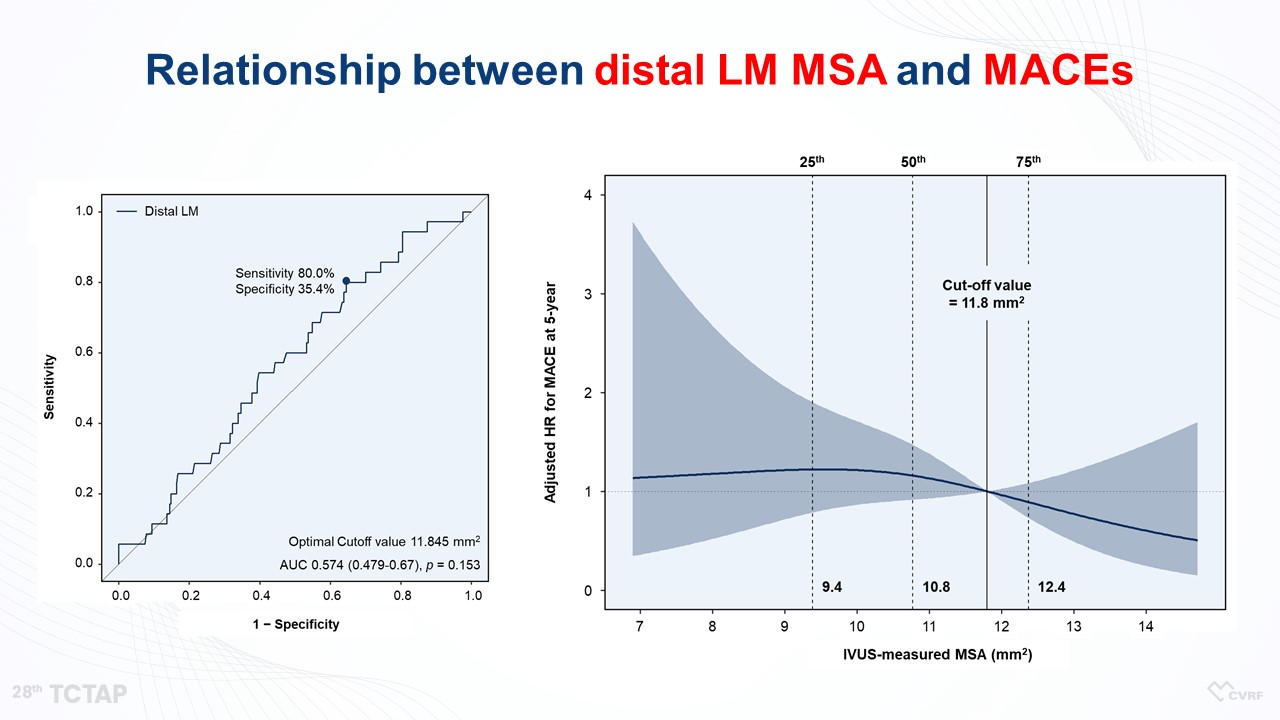
“LM did not show any association between LM MSA and MACEs, because LM MSA was large enough not to occur any cardiovascular events (Figure 7, 8). However, the MSA of LAD and LCX was linearly associated with MACEs (Figure 9). So, according to the aforementioned criteria, there was no significant difference in clinical outcomes between LM MSA >11.8 mm2 and LM MSA <11.8 mm2, but the 5-year MACE rates in the LAD MSA <8.3 mm2 and LCX MSA <5.7 mm2 were higher compared with the patients in the LAD MSA >8.3 mm2 and LCX MSA >5.7 mm2, respectively, (Figure 10)” he said.
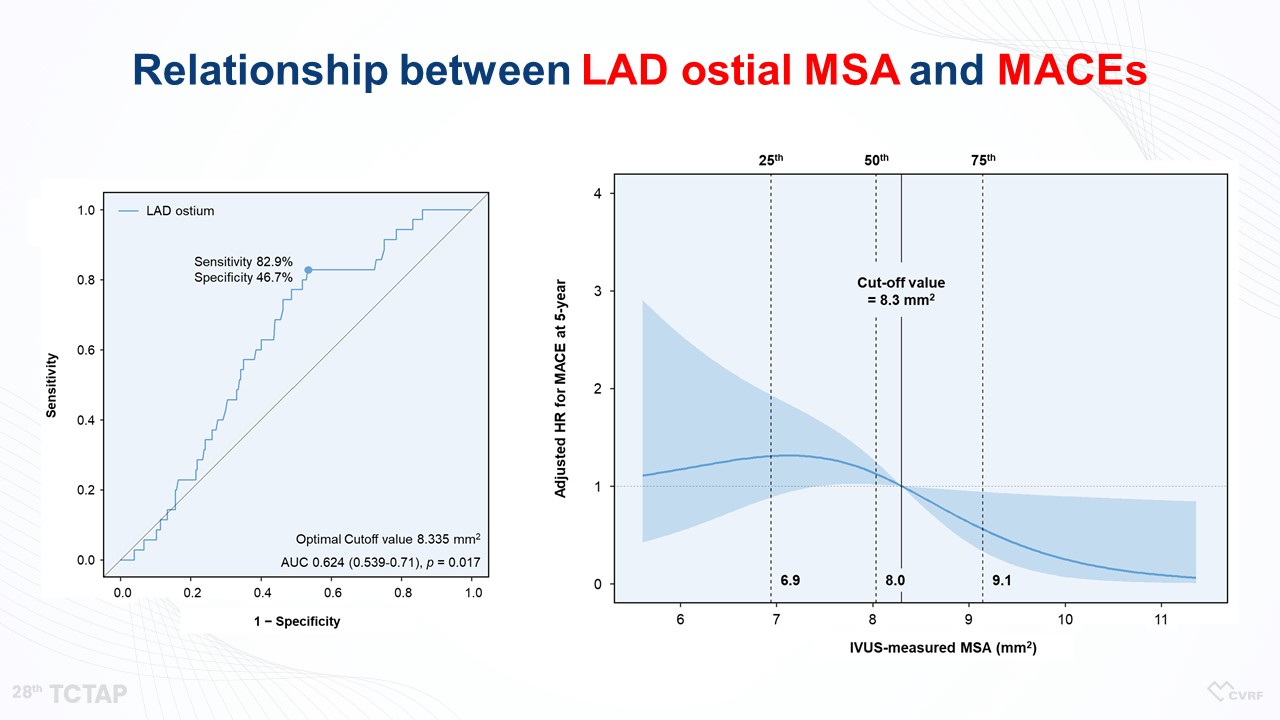
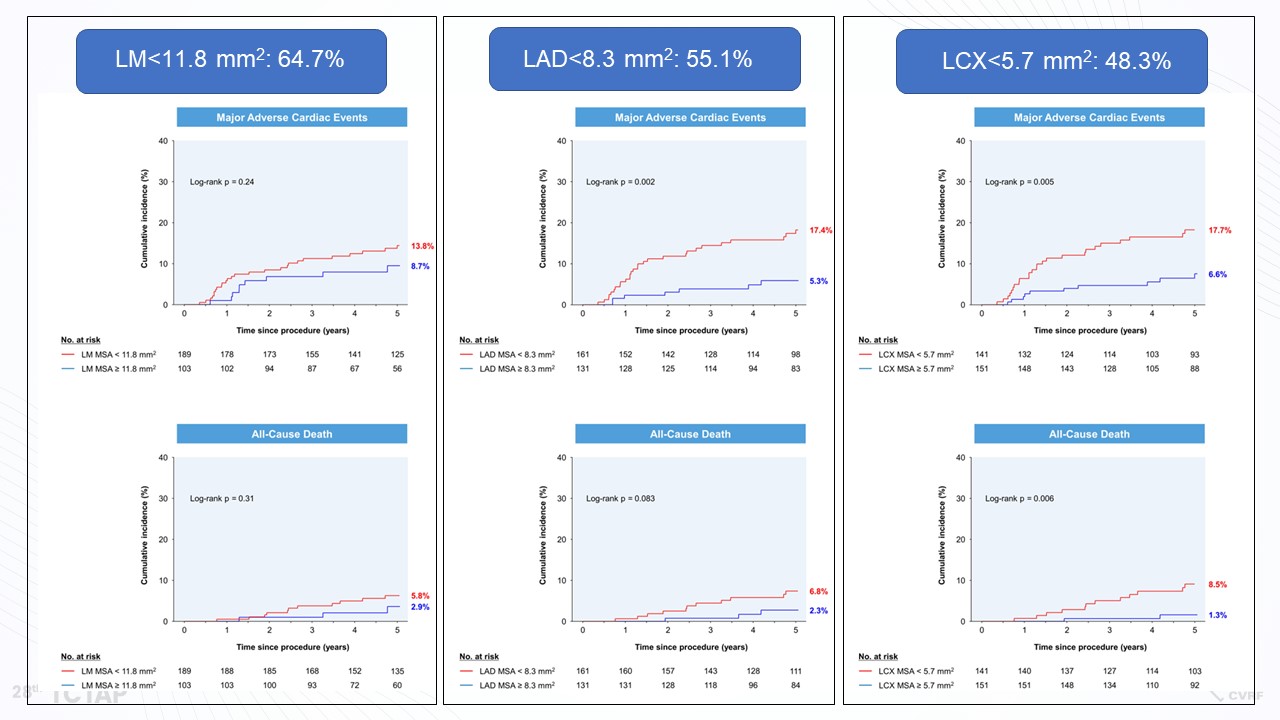
“In patients undergoing LM two-stenting with the crush technique, the final IVUS-MSA within LAD and LCX ostium showed a linear relationship with the hazard of 5-year MACE. larger IVUS-MSA was associated with better clinical outcomes. The optimal IVUS-MSA criteria that predicted 5-year MACE on a segmental basis were 11.8 mm2 for the distal LM, 8.3 mm2 for the LAD ostium, and 5.7 mm2 for the LCX ostium. Obtaining a sufficiently large MSA could be pivotal in preventing adverse clinical events in patients undergoing LM two-stenting procedures. Therefore, interventionists should make an effort to achieve sufficient MSA under the IVUS guidance,” He concluded.
Hot Topics
Left Main & Multi-Vessel (Practice Changes After ISCHEMIA)
Sunday, May 7, 4:20 PM ~ 5:50 PM
Presentation Theater 1, Vista 3, B2
Edited by

Hoyun Kim, MD
Bucheon Sejong Hospital, Korea (Republic of)