
Kyung Woo Park, MD
Seoul National University Hospital, Korea (Republic of)
Kyung Woo Park, MD (Seoul National University College of Medicine, Korea) introduced the latest evidence on long-term antiplatelet management, including their HOST-EXAM trial at TCTAP 2023 on May 7th.
Antiplatelet therapy is the mainstay of treatment to reduce the ischemic risk in patients undergoing percutaneous coronary intervention (PCI). The current guidelines recommend life-long single antiplatelet therapy (usually aspirin as the first-line treatment) following a period of dual antiplatelet therapy (DAPT). However, this recommendation was not based on a large, randomized trial. Therefore, the comparative efficacy and safety of monotherapy with a P2Y12 inhibitor or aspirin after a due duration of DAPT still remains incompletely understood in post-PCI patients.
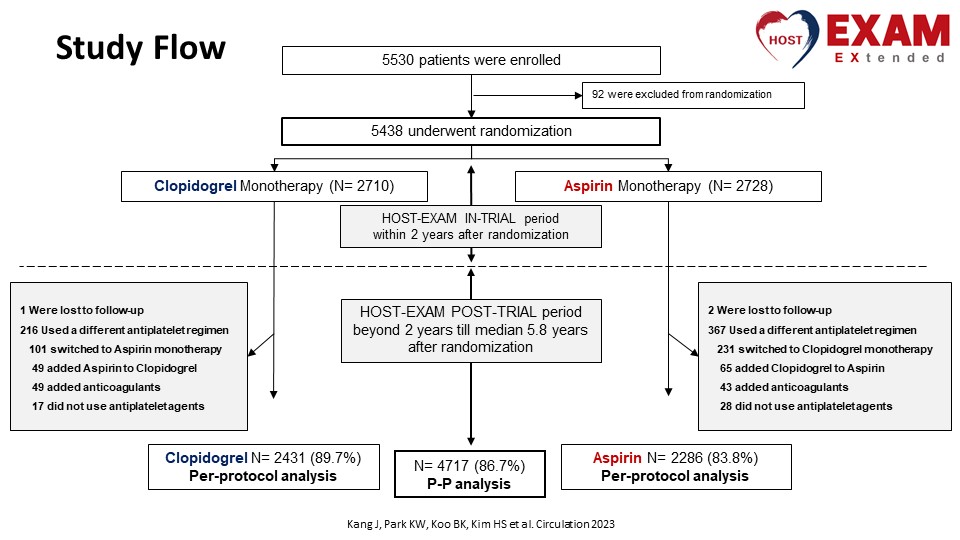
In the HOST-EXAM trial, patients undergoing PCI with a drug-eluting stent who completed 6-18 months of DAPT without any ischemic or major bleeding complications were randomized to monotherapy with clopidogrel or aspirin. The primary endpoint was a composite of all-cause death, non-fatal myocardial infarction (MI), stroke, readmission due to acute coronary syndrome, and bleeding academic research consortium (BARC) type ≥3 bleeding. At 24 months, the use of clopidogrel was associated with a 27% relative reduction in risk of the primary composite endpoint. The benefit of clopidogrel was also observed for the thrombotic composite outcomes as well as any bleeding.
“In the HOST-EXAM Extended study, we extended follow-up of these patients up to median 5.8 years after initial randomization,” Park mentioned (Figure 2).
In the HOST-EXAM Extended study, the composite primary endpoint occurred in 12.8% of the clopidogrel group compared to 16.9% of the aspirin group at a median follow-up of 5.8 years. (HR 0.74; 95% CI 0.63-0.86; p <0.001), giving an absolute risk reduction of 4.1% (number needed to treat 24) (Figure 2).
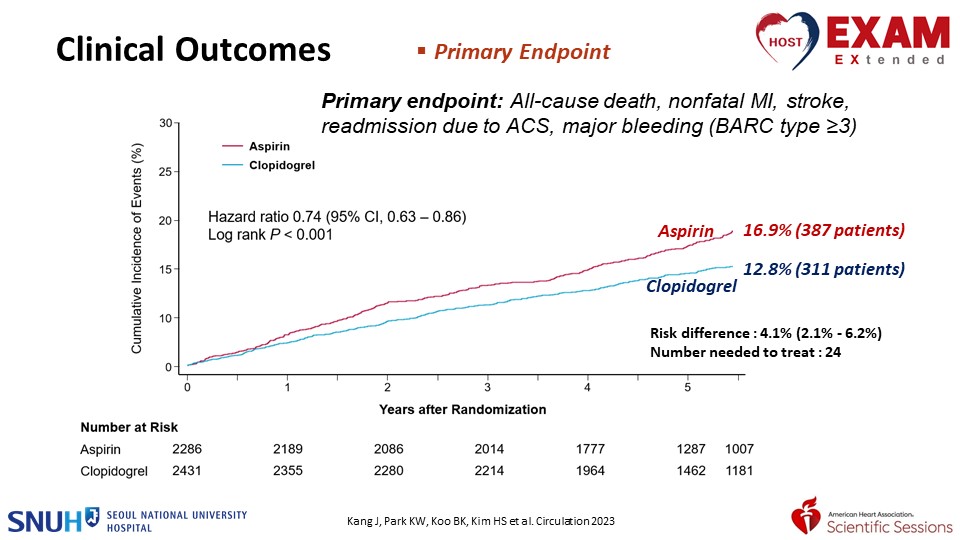
“Extended follow-up of the HOST-EXAM showed the continued benefit of clopidogrel over aspirin,” Park explained.
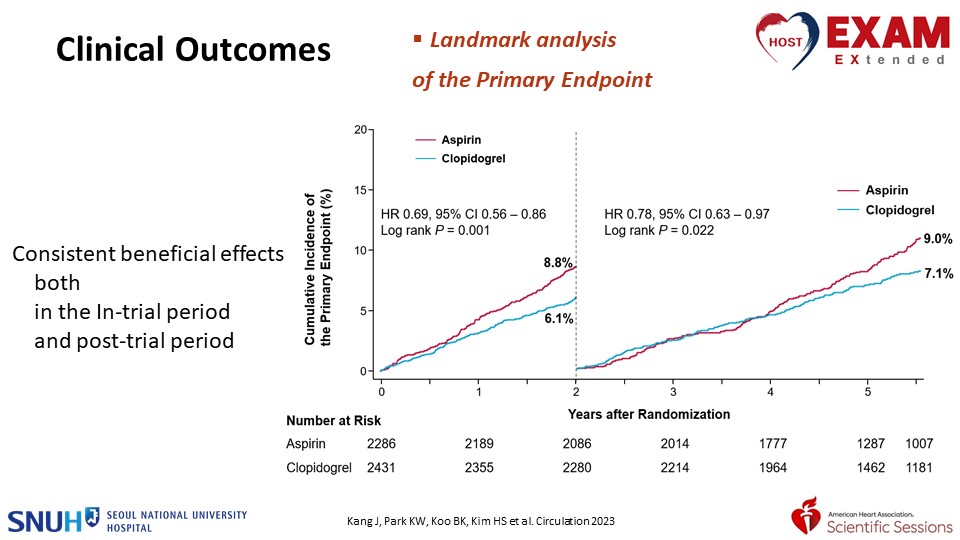
Park continued, “Also when we did the landmark analysis, there were consistent beneficial effects of clopidogrel both in the in-trial period (0 to 2 years) and post-trial period (2 to 5.8 years). There was consistent effect favoring clopidogrel over aspirin with no interaction between the treatment effect and subgroups.” (Figure 3).
In the initial two-year results of the HOST-EXAM trial, there was a numerically higher rate of all-cause mortality in the clopidogrel group despite the trial was not powered for mortality. However, in the extended follow-up result, there were no significant differences in all-cause death between the groups (clopidogrel 6.2% vs. aspirin 6.0%; hazard ratio [HR] 1.04; 95% confidence interval [CI] 0.82-1.31; p=0.742).
The PANTHER trial, led by Dr. Marco Valgimigli and colleagues, was the most comprehensive individual participant data (IPD) meta-analysis to date of randomized controlled trials evaluating the effect of monotherapy with currently recommended oral P2Y12 inhibitors (clopidogrel, prasugrel, or ticagrelor) versus aspirin on adjudicated ischemic and bleeding outcomes in patients with established coronary artery disease. In the result of the PANTHER analysis, P2Y12 inhibitor monotherapy was associated with significantly lower rates of composite cardiovascular death, MI, and stroke compared with aspirin monotherapy (5.5% vs. 6.3%; HR 0.88; 95% CI 0.79-0.97; p=0.014), mainly due to lower rates of MI. Major bleeding was similar (1.2% vs. 1.4%; HR 0.87; 95% CI 0.70-1.09; p=0.23), but the hemorrhagic stroke was lower with P2Y12 inhibitor monotherapy. The risk of net adverse clinical events was reduced with P2Y12 inhibitor monotherapy compared with aspirin monotherapy (6.4% vs. 7.2%; HR 0.89; 95% CI 0.81-0.98; p=0.020).
Park concluded. “Based on the HOST-EXAM trial and the PANTHER analysis, I believe that it may be reasonable to use clopidogrel over aspirin as chronic antiplatelet monotherapy in patients with stabilized coronary artery disease.”
Hot Topics
All About New Data of Antithrombotics
Sunday, May 7, 2:40 PM ~ 4:10 PM
Valve & Endovascular Theater, Vista 1, B2
Edited by

Sangwoo Park, MD
Ulsan University Hospital, Korea (Republic of)