
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-160
Optical Coherence Tomography Guided Percutaneous Coronary Intervention of Spontaneous Recanalized Coronary Thrombus
By Chen Shih-Chung
Presenter
CHEN SHIH-CHUNG
Authors
Chen Shih-Chung1
Affiliation
Cheng Hsin General Hospital, Taiwan1,
View Study Report
TCTAP C-160
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular
Optical Coherence Tomography Guided Percutaneous Coronary Intervention of Spontaneous Recanalized Coronary Thrombus
Chen Shih-Chung1
Cheng Hsin General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
56 years old woman
Relevant Clinical History and Physical Exam
A 56-years-old woman with underlying history of hyperlipidemia without medical treatment. She experienced effort precordial tightness and shortness of breath for 8 months after COVID-19 vaccination. She received exercise TI 201 myocardial perfusion scan showed myocardial ischemia. EKG found old anterior wall myocardial infarction. Echocardiogram showed left ventricle anterior wall hypokinesia, LVEF 38%.

Relevant Test Results Prior to Catheterization
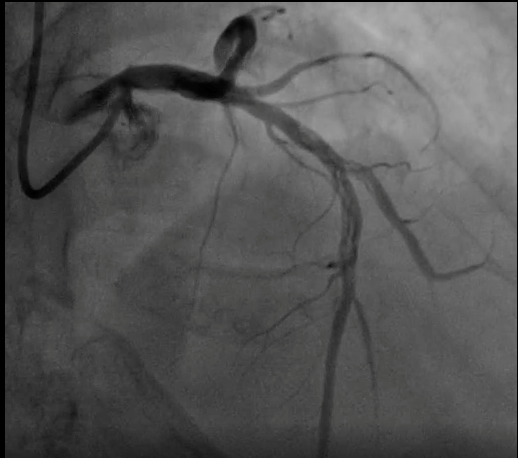
Coronary angiogram found left anterior descending artery from proximal to middle 70~80% long diffuse stenosis with spontaneous recanalized coronary thrombus. Also left anterior descending artery diagonal 2 branch bifurcation was 70% stenosis with spontaneous recanalized coronary thrombus (Medina 1.1.1)

Relevant Catheterization Findings
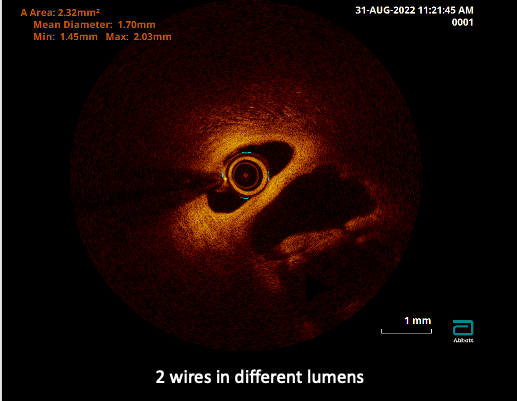
Coronary angiogram found left coronary artery middle and diagonal branch braided apperance. OCT found recanalized thrombi, high backscattered septa that divided the lumen into multiple small cavities, created “lotus root” appearance
Interventional Management
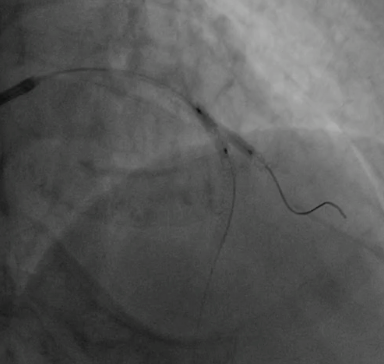
Procedural Step
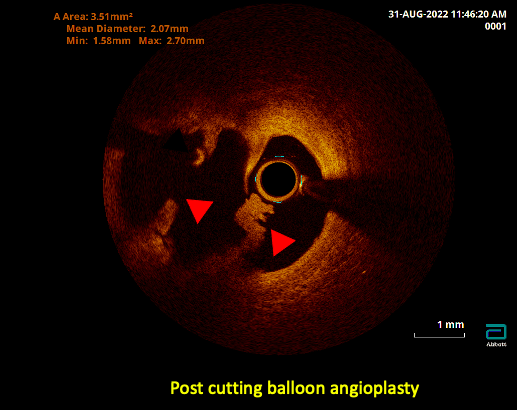
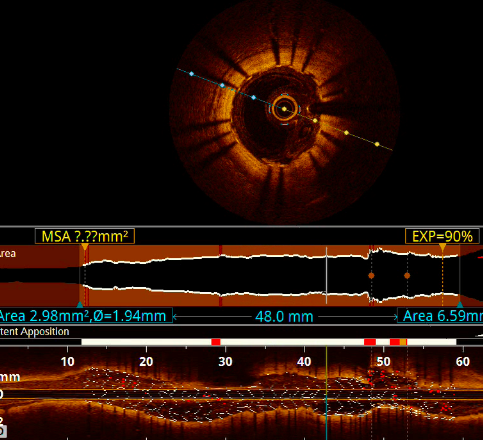
Left main coronary artery was engaged with EBU3.5/7F guiding catheter. We advanced Runthrough to LAD-D and second wire Sion to LAD-DB2 but can't advance. TThen we used with Sasuke double lumen catheter and successful advance Pilot 50 to LAD-DB2 distal. OCT found multiple channels with LAD-D and DB2 branch wires are at different channels so we used cutting balloon 2.5 x 10mm as unconventional method. OCT was rechecked again and successfully destroyed to multiple channel of SRCT between LAD and Diagonal 2 branch. Long diffuse dissection found after POBA so we deployed to LAD-DB2 branch with DES Synergy 2.5 x 16mm and advanced LAD-M bifurcation to Pantera LEO 3.0 x 20mm and done Mini-Crush technique. Deployed for main vessel LAD-P to M long diffuse lesion with DES Xience 2.75 x 48mm at 14atm. Then we rewire Fielder XTR to DB2 branch with the support of Sasuke but difficult to deliver to Diagonal 2 branch. POT with Pantera LEO 3.0 x 20mm to LAD stent proximal site. Then successfully advance Fielder XTR to DB2 branch. Final kissing balloon technique with Pantera 2.75 x 12mm to LAD main vessel and MINI TREK 1.5 x15mm to LAD-DB2.
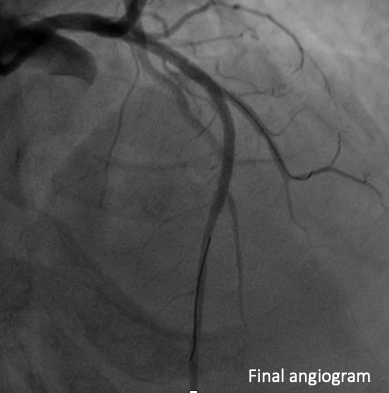
Case Summary
This is a case of SRCT (Spontaneous Recannalized Coronary Thrombus) that was confirmed with OCT. For secure side branch patency, main trunk & side branch wire must be in same channel. Due to relatively unstable hemodynamic, we chosed to use unconventional method with 2.5 x 10mm Wolverine cutting balloon. Relatively large side-branch diagonal branch, possible dissection at ostial diagonal branch, we chosed upfront 2 stents, bifurcation stenting technique we used Mini-crush stenting. Some difficult when rewire to side branch and initial POT to main branch stent proximal and then successfully delivered. If without guidewire recross, unrescuable side-branch occlusion can be occurred.