
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-020
Nightmares in Primary PCI in a STEMI Patient
By Wei-Chun Huang, Meitzu Wang
Presenter
Wei-Chun Huang
Authors
Wei-Chun Huang1, Meitzu Wang1
Affiliation
Kaohsiung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-020
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Nightmares in Primary PCI in a STEMI Patient
Wei-Chun Huang1, Meitzu Wang1
Kaohsiung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Mr Lu
Relevant Clinical History and Physical Exam
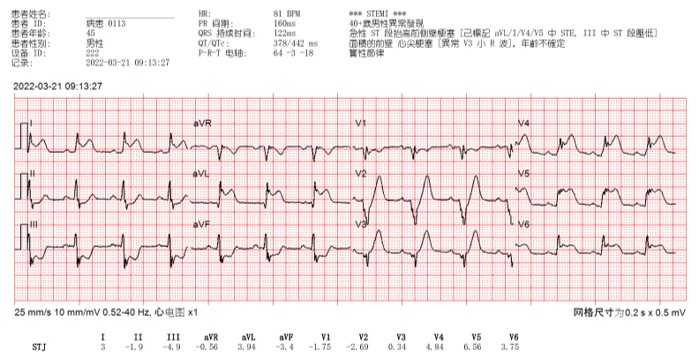
This 38 year-old man is a cigarette smoker for decades (1-2 PPD for 15 years) and denied other systemic disease before. According to the medical chart statement, he suffered from chest pain, palpitation with cold sweating since this morning prior to ER. His family called ambulance for help. At the Ambulance, 12-lead ECG was done and showed ST elevation in V2-6, I aVL and ST depression in II, II, aVF.
Relevant Test Results Prior to Catheterization
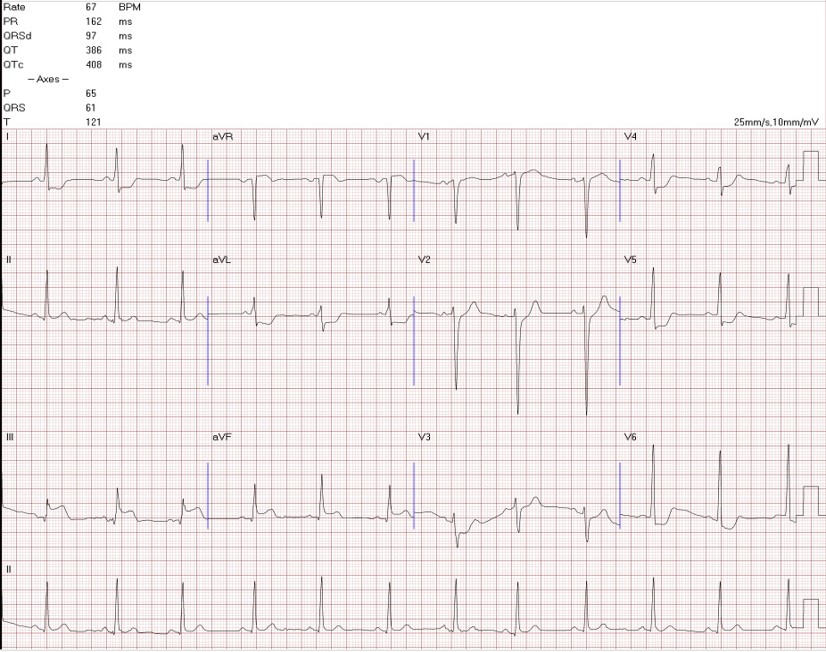
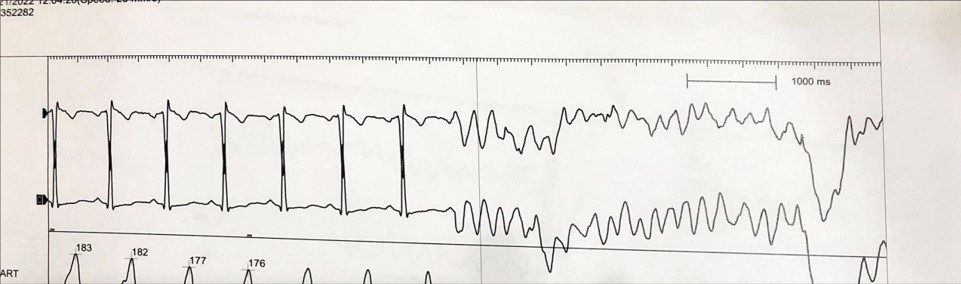
Unfortunately, the patient collapsed at triage. ECG showed ventricular fibrillation. After CPR for 5 minutes and defibrillation, his consciousness regained. After resuscitation, 12 lead ECG showed ST elevation over II, III, aVF and ST depression over V3-6, I, aVL. After brain CT showed no ICH and Chest CT showed no aortic dissection, the patient was sent to cath room.
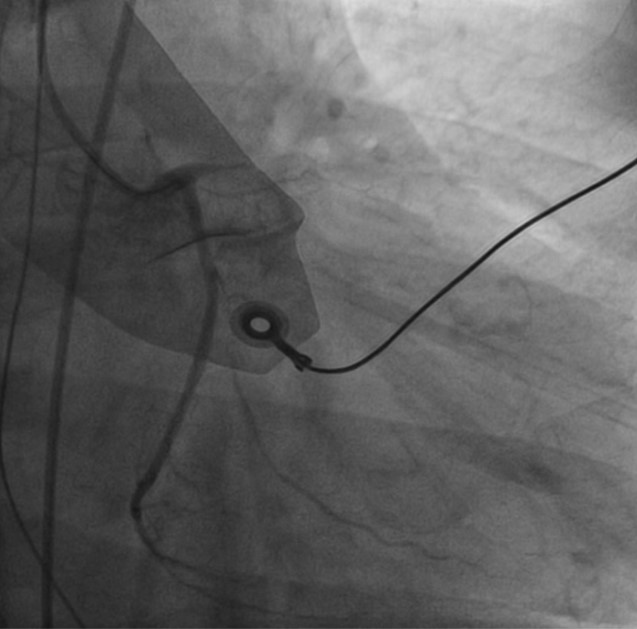
Relevant Catheterization Findings
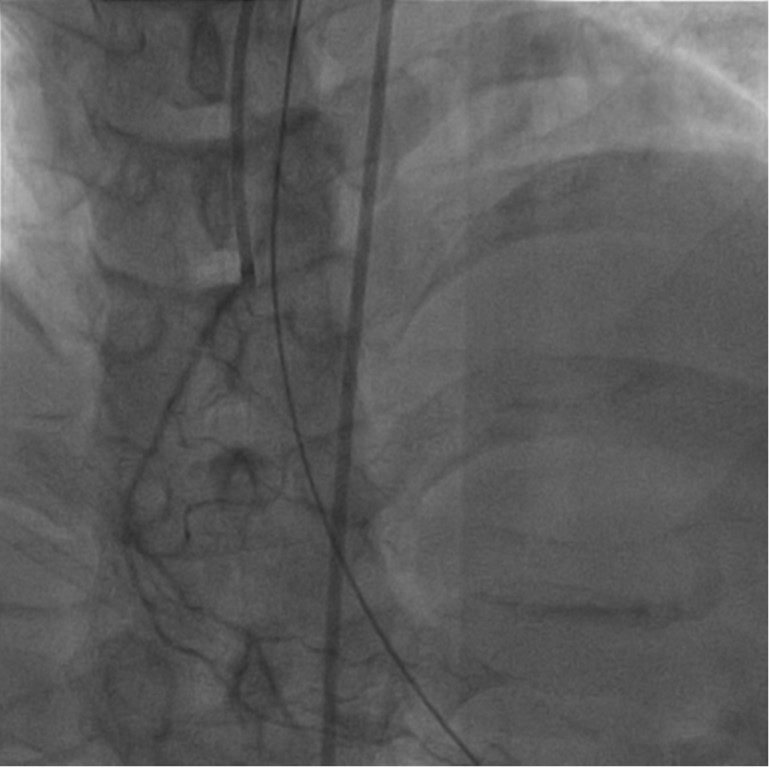
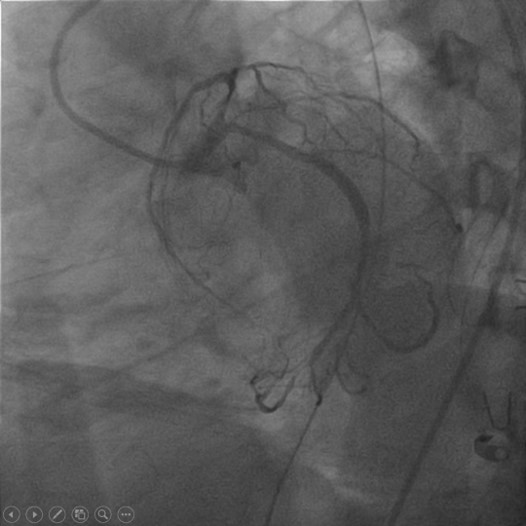
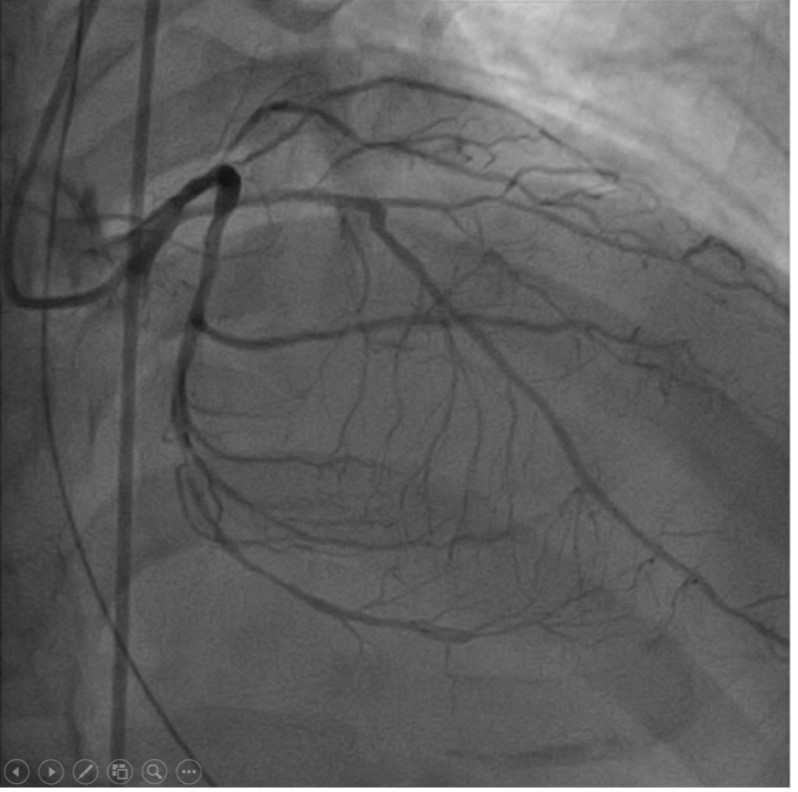
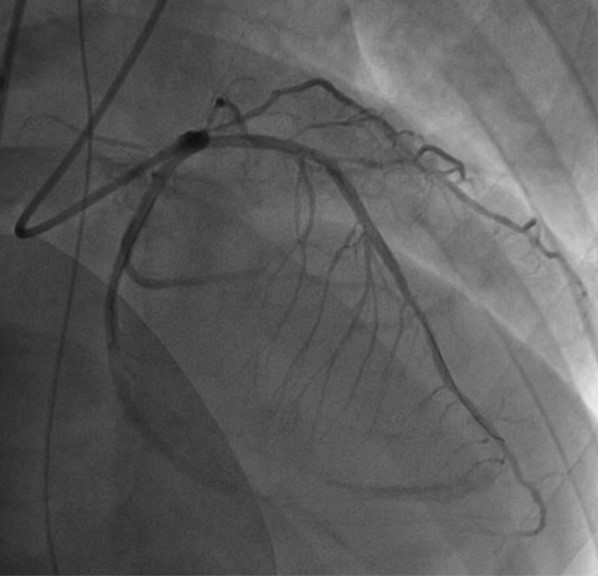
The angiography showed diffuse atherosclerosis with small caliber over right coronary artery (Segment 1-3). Short left main was noted. There was a diffuse lesion over proximal part of left descending coronary artery (Segment 6). A discrete lesion over distal part of left circuflex coronary artery (Segment 13-14) was identified
Interventional Management
Procedural Step
It is very difficult to decide which one is culprit lesion, because ECG change from ST elevation over V2-6, I aVL to ST elevation over II, III, aVF and the coronary image was not clear. Due to severe stenosis of LCX lesion, PCI was performed. However, sudden onset of ventricular fibrillation was noted. After CPR and defibrillation, urgent ECMO was performed. After ECMO, angiography showed acute closure of LAD. Therefore, thrombus was aspirated. However, recurrent ventricular fibrillation was still noted. After stent of LAD-P and LCX-D. IABP was performed. The patient was transferred to ICU care. After cirtical care, the patient finally was discharged about 3 weeks later.
Case Summary
The patient's ECG change from antero-lateral STEMI to inferior STEMI. It is very difficult to identify culprit lesion. ECPR is effective in cath room for cardiac arrest patients. Adequate CPR and medication is important to save the patients in cath room.