
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-125
Conquering the Caravel-Induced Crisis: Retrograde Dissection Involving Left Coronary System
By Raghav Sharma, Harsimran Singh, Shaweta Vohra, Deepak Basia
Presenter
Harsimran Singh
Authors
Raghav Sharma1, Harsimran Singh2, Shaweta Vohra1, Deepak Basia1
Affiliation
Meditrina Hospital, India1, Pancham Hospital, India2,
View Study Report
TCTAP C-125
CORONARY - Complications (Coronary)
Conquering the Caravel-Induced Crisis: Retrograde Dissection Involving Left Coronary System
Raghav Sharma1, Harsimran Singh2, Shaweta Vohra1, Deepak Basia1
Meditrina Hospital, India1, Pancham Hospital, India2,
Clinical Information
Patient initials or Identifier Number
AR
Relevant Clinical History and Physical Exam
A 57-year-old female known case of diabetes and hypertension was admitted with a history of chest pain for 4 days. Pain was a central, compressive type, nonradiating. No family history of coronary artery disease. Vitals were stable.On systemic examination CVS- S1S2 normal, no added sounds, no murmur.RS- Air entry bilateral clear. No added sounds.
Relevant Test Results Prior to Catheterization
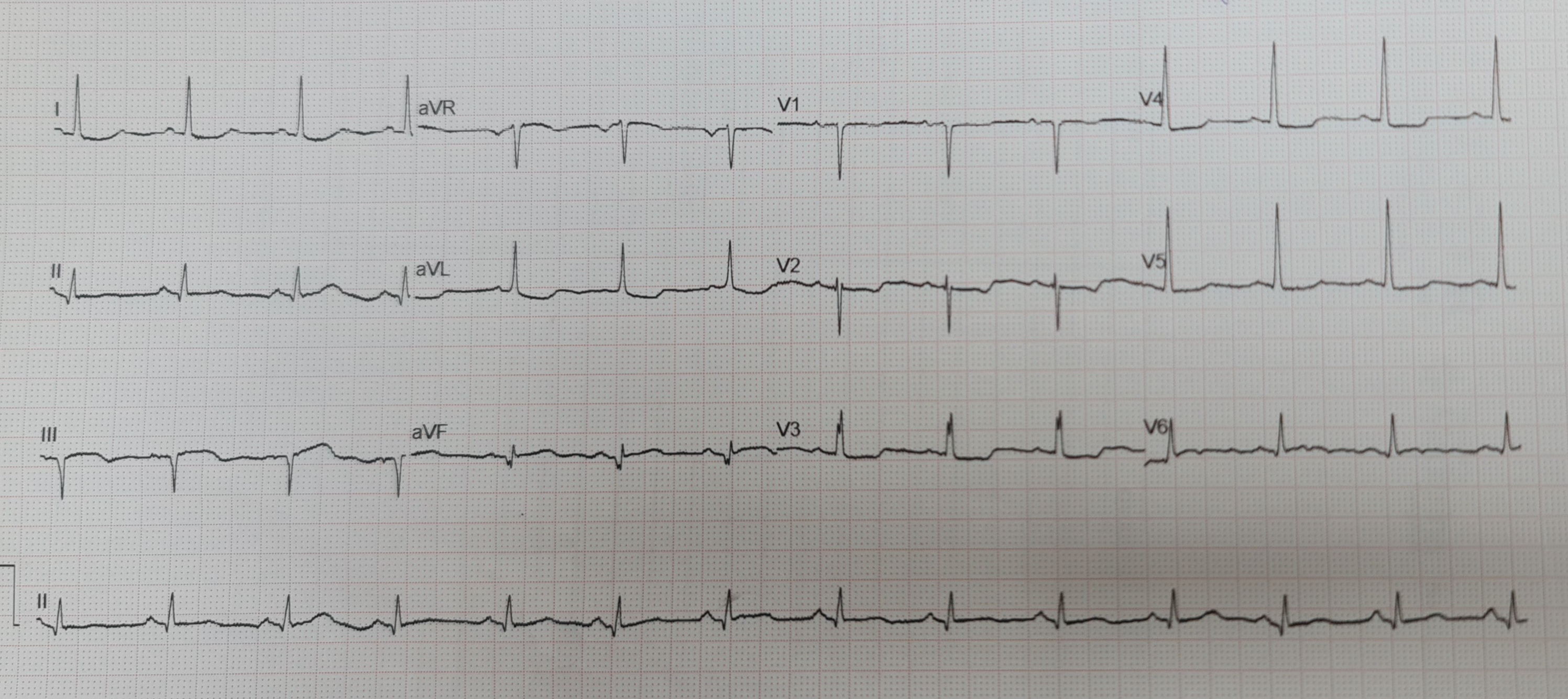
Hemoglobin- 11 gm/dlPlatelets- 2.8 Lacs Total count - 9000Blood urea - 13 mg/dlS.Creatinine- 0.8 mg/dlECG: Normal sinus rhythm, ST depression in antero lateral leads2D-ECHO- No regional wall motion abnormality. Ejection fraction - 50%
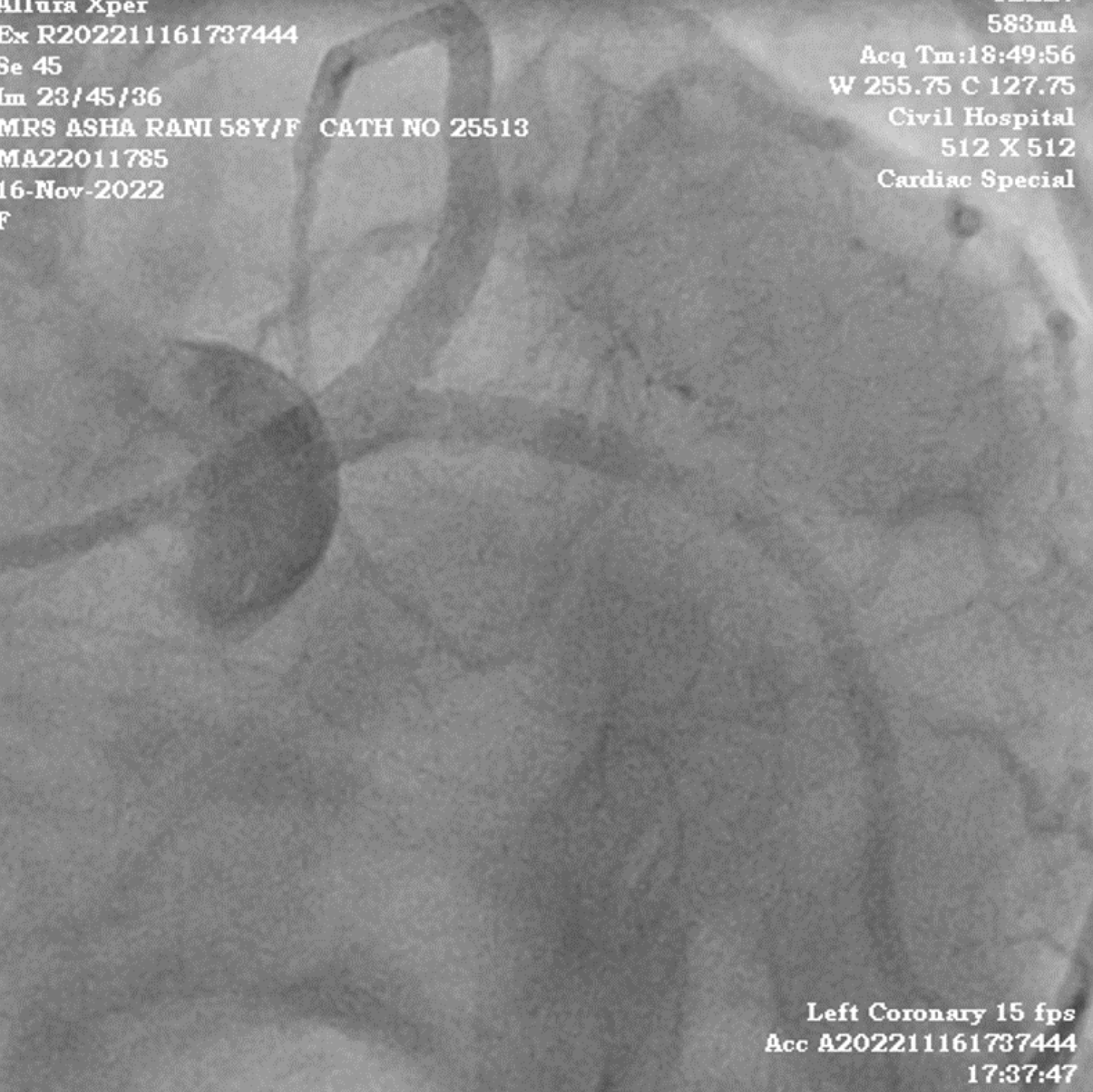
Relevant Catheterization Findings
Coronary angiogram showed
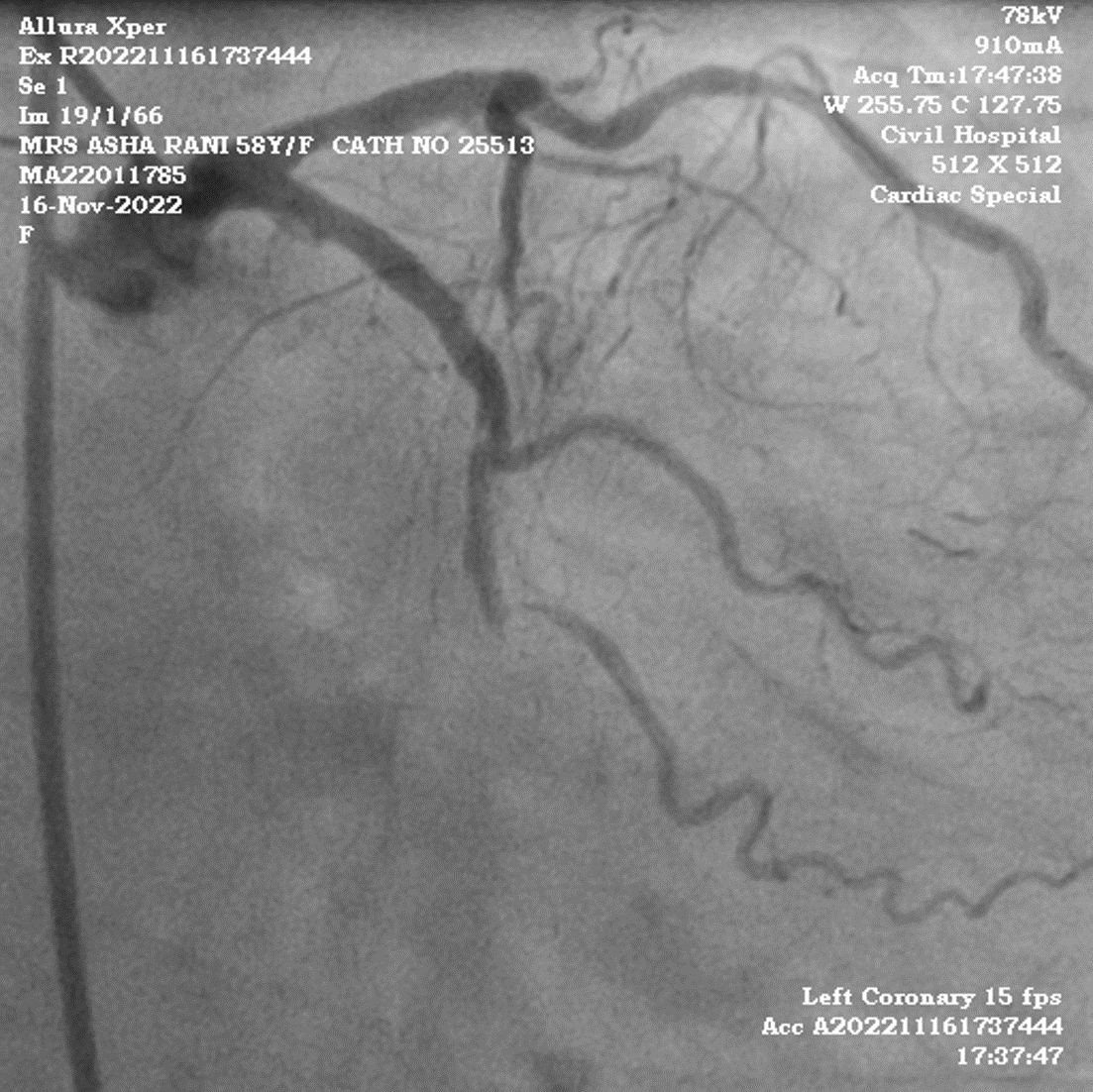
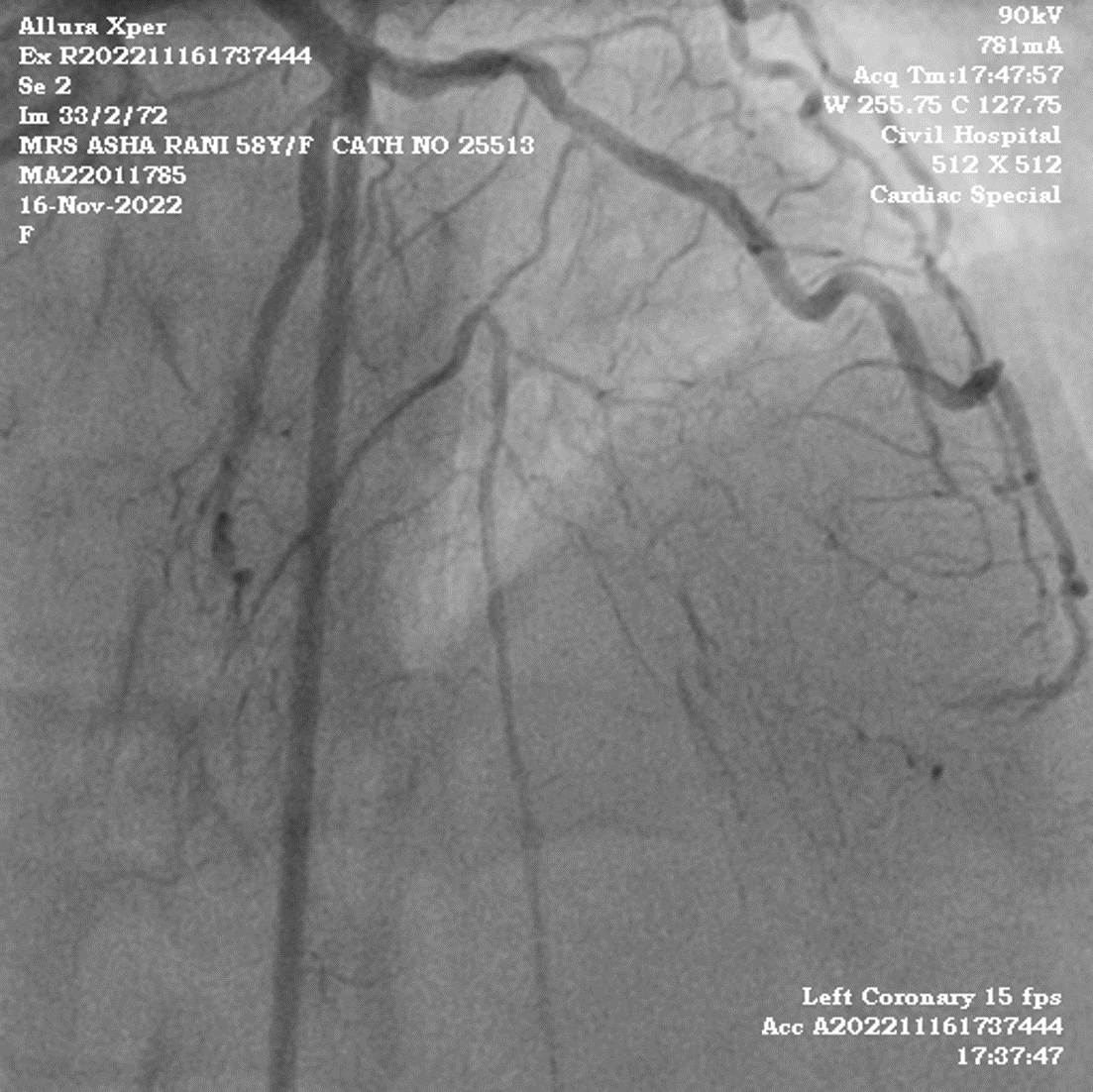
LM- Normal
LAD- Diffuse lesion in the mid segment (99% stenosis) with both antegrade and retrograde filling.
LCX- Sub total occlusion
RCA- 70 % lesion in the mid segment
Interventional Management
Procedural Step
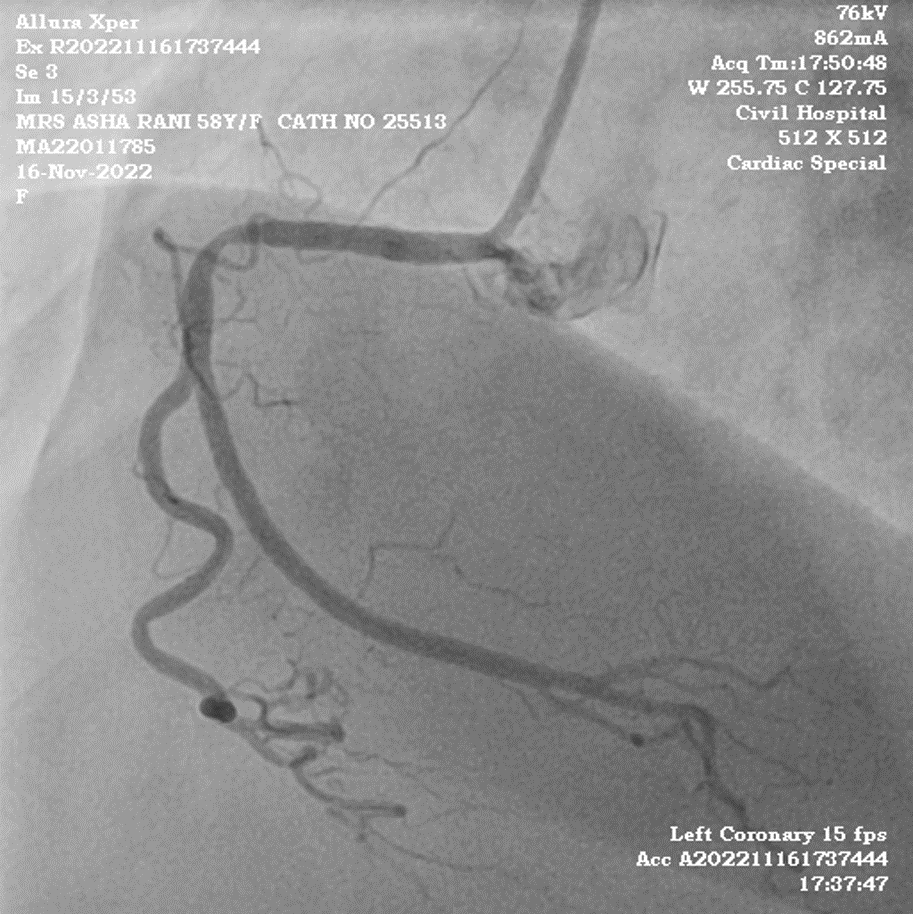
1. EBU (Medtronic, USA) guide was used to engage the left coronary. 2. Miracle wire (Asahi, japan) tried to cross LAD along with the caravel microcatheter (Asahi, Japan).3. Check shot through caravel leads to retrograde dissection involving LM, LAD & LCX.4. As vitals were stable, LCX was opened using 2.5x36mm DES.5. Using the mini crush technique bifurcation stenting was done in LCX (3.5X16mm)and LM to LAD (4.0x20mm), followed by POT in LM.6. Fielder FC (Asahi, Japan) wire crossed in the lesion in LAD.7. Angio shot taken from RCA to confirm the position of LAD wire in the true lumen. Pre dilatation did using a 2.0x10 mm NC (Sapphire, CSI, USA) balloon.8. 2.5x48 mm DES was deployed from mid to distal LAD.9. Proximal to mid LAD stented with 3x32mm DES overlapping the distal edge of proximal stent and proximal edge of distal stent.10. Post dilatation from proximal to mid LAD done using 3.5x12 mm NC Balloon.11. Fielder FC wire reintroduced in LCX & ostium was dilated with 1.25x10 mm NC balloon.12. Final KBI done using 4.0x12mm NC in LAD and 3.5x12mm NC in LCX.13. TIMI 3 flow achieved


Case Summary
Nightmares in cath labs are rare especially when retrograde dissection is extending into the left main and origin of LCX, one has to be careful not to lose access to the main vessel and skillful enough to wire the side branch. Calm mind, and proper awareness of material and stenting techniques should be known to the operator in order to bail out patients from critical conditions and prevent mortality. Henceforth maturity and experience are required during critical complications which come with repeated practice and excellent exposure.