
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-108
Last but Not Least
By Samrany San, Sokha Chan, Chour Sok
Presenter
Samrany San
Authors
Samrany San1, Sokha Chan1, Chour Sok1
Affiliation
Calmette Hospital, Cambodia1,
View Study Report
TCTAP C-108
CORONARY - Complications (Coronary)
Last but Not Least
Samrany San1, Sokha Chan1, Chour Sok1
Calmette Hospital, Cambodia1,
Clinical Information
Patient initials or Identifier Number
P.R, male, 61 years-old
Relevant Clinical History and Physical Exam
A 61 year-old male hospitalized for anterior AMI with 28 hours onset. He had a history of smoking, hypertension and type 2 diabetes. Physical examination was unremarkable. Emergency coronary angiography was proceed.
Relevant Test Results Prior to Catheterization
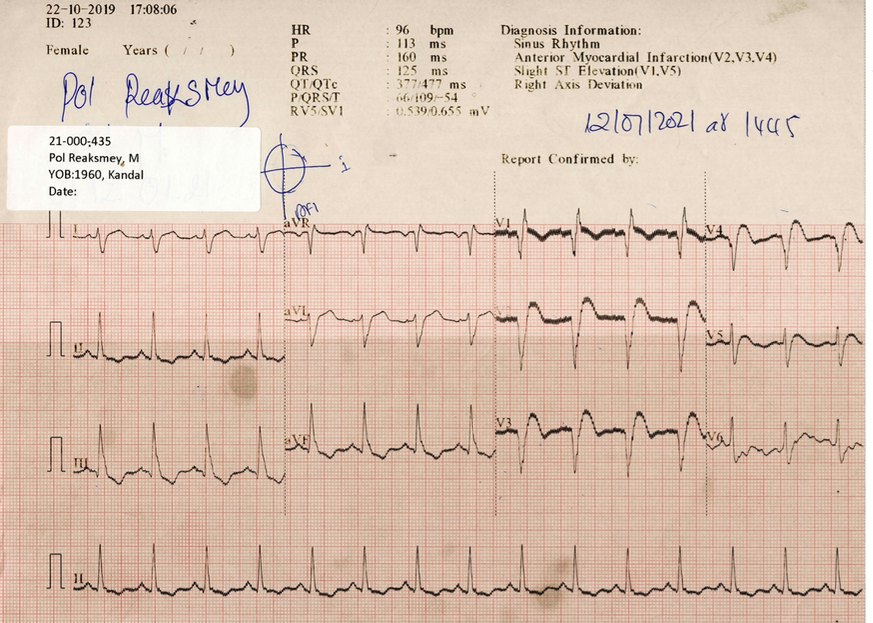
Electrocardiography (ECG) revealed bifascicular block (complete right bundle block-CRBBB and left posterior fascicular block-LPFB) with ST segment elevation in V1 to V5(Fig 1.). Echocardiogram revealed a systolic dysfunction (EF = 30%).
Relevant Catheterization Findings
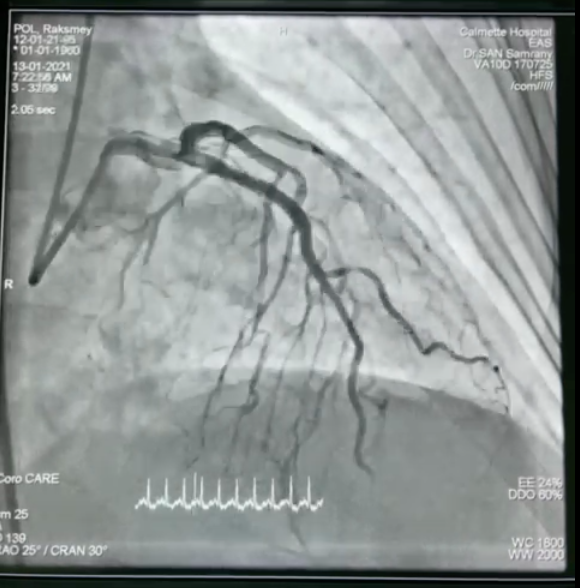
Left coronary angiography showed thrombotic occlusion proximal LAD (Fig.2).



Right coronary angiography demonstrated no lesion (Fig.3).
A 6F sheaths were inserted through right femoral artery. A guide wire was passed through the lesion. After pre-dilatation by balloon Sprinter Legend 2.25 x 10 mm at 12 atm. Integrity 3.5 mm x 26 mm stent was deployed in the proximal LAD. The final angiography showed a good result with TIMI 3 flow (Fig. 4).
Interventional Management
Procedural Step
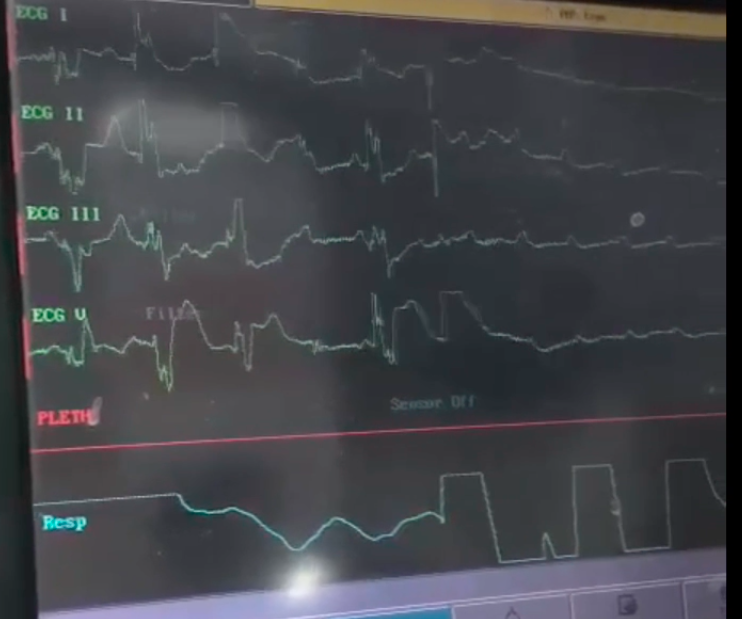
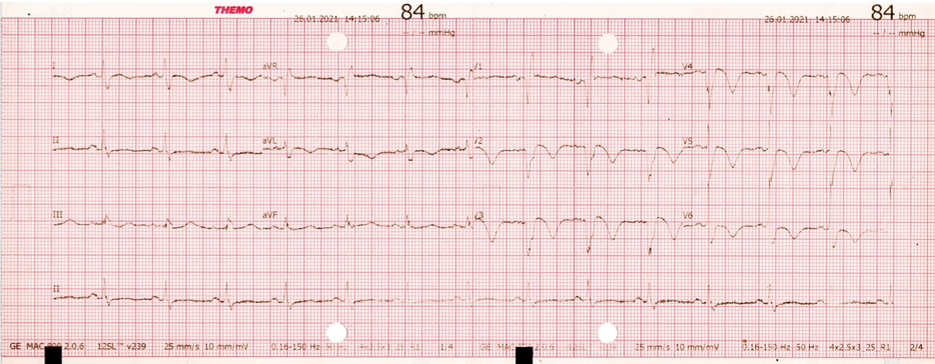
12 hours after, he developed an episode of unresponsiveness. On an ECG monitoring, he lost his escape rhythm and showed cardiac arrest. He received cardio-pulmonary resuscitation (CPR) for 1 min, resulting in the return of spontaneous circulation. An ECG after recovery showed rhythm strip with alternating bundle branch block and complete heart block followed with asystole (Fig. 5). Emergency coronary angiography showed potency of the stent LAD (Fig. 6). and right coronary artery (RCA) remained unchanged. After reviewing compare to previous angiography, revealed occlusion of the septal branch of LAD. Temporary pacemaker (TPI) in the femoral vein was placed. 72 hours later, he was sinus rhythm, with CRBBB, rate of 86 bpm and TPI was removed (Fig. 7). The patient showed a good course and was discharged home 11 days after PCI without need for permanent pacemaker implantation.5 days later, he was taken back to the emergency room with respiratory distress, fever and faiblesse at left side. An ECG showed similar to previous, furthermore, echocardiogram revealed apical LV thrombus with diameter 3 x 4 mm. Brain CT scan showed thrombus at anterior cerebral artery in segment M 2. Unfortunately, He was died 7 days hospitalization due to septic shock by inhaled pneumonia and extended ischemic stroke.
Case Summary
This case represents an example of the extended anterior AMI presented with RBBB and LPFB, despite successful revascularization of the LAD, the patient had alternating bundle branch block and complete heart block resulting cardiac arrest. When performing PCI to the LAD with conduction abnormalities, attention should be given not only to preservation of the diagonal branch but also septal perforators. Although relatively uncommon, occlusion of a septal perforator may lead to conduction abnormalities that cause complete heart block and generally associated with acute reduction systolic function due to myocardial damage. Even it delayed or temporary, it may lead to increase in mortality.