
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-072
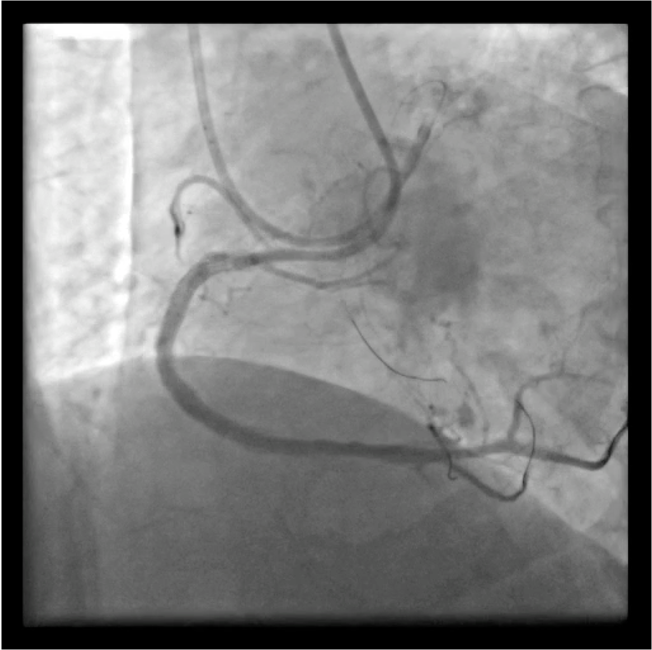
Recannalization of RCA Chronic Total Occlusion Lesion
By Tien Ping Tsao, Hao Neng Fu
Presenter
Hao Neng Fu
Authors
Tien Ping Tsao1, Hao Neng Fu1
Affiliation
Cheng Hsin General Hospital, Taiwan1,
View Study Report
TCTAP C-072
CORONARY - Chronic Total Occlusion
Recannalization of RCA Chronic Total Occlusion Lesion
Tien Ping Tsao1, Hao Neng Fu1
Cheng Hsin General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
XMK
Relevant Clinical History and Physical Exam
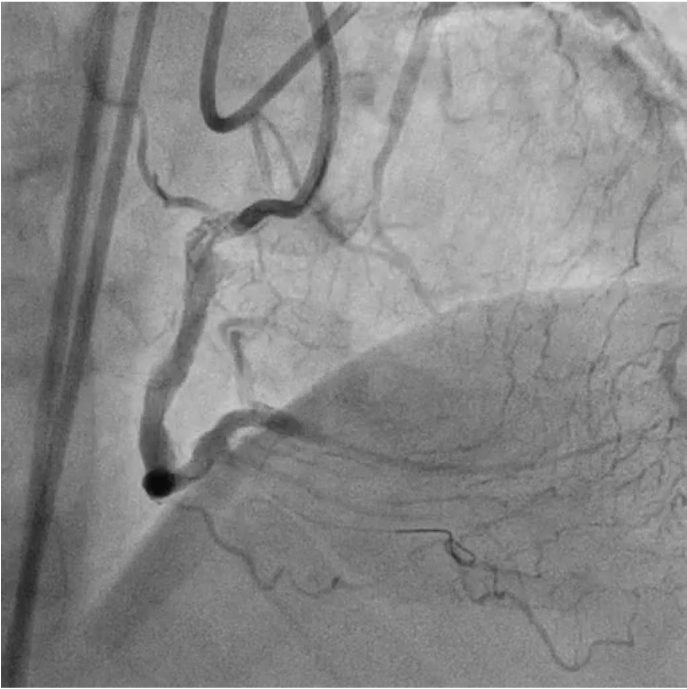
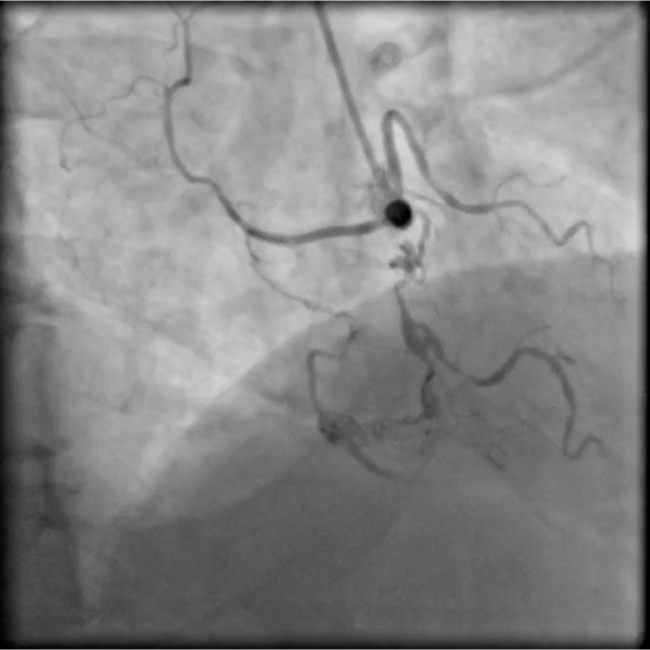
A 63-year-old man with underlying history of hypertension, hyperlipidemia and diabetes mellitus, presented with effort angina. He had history of multivessel coronary artery disease. In 2017, PCI for RCA CTO lesion was done with ADR technique & 4 bare metal stents deployed from distal to proximal RCA. Almost all of stent segment are in subintimal space (Figure A: Pre-PCI, Figure B: Post-PCI).
Relevant Test Results Prior to Catheterization
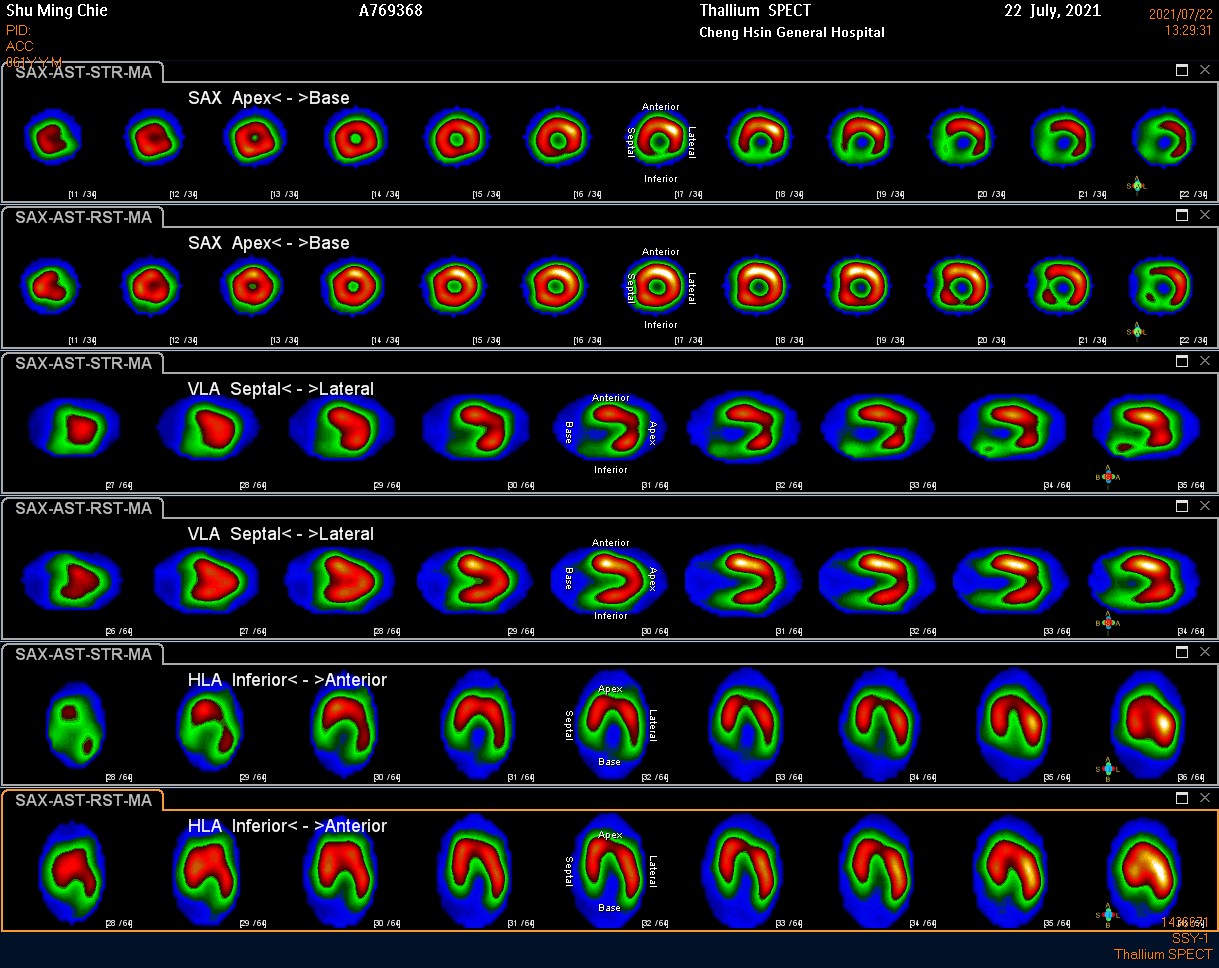
Stress myocardial perfusion scan illustrated reversible ischemia in inferior, inferolateral and inferoseptal wall. (Fig-A)
Relevant Catheterization Findings
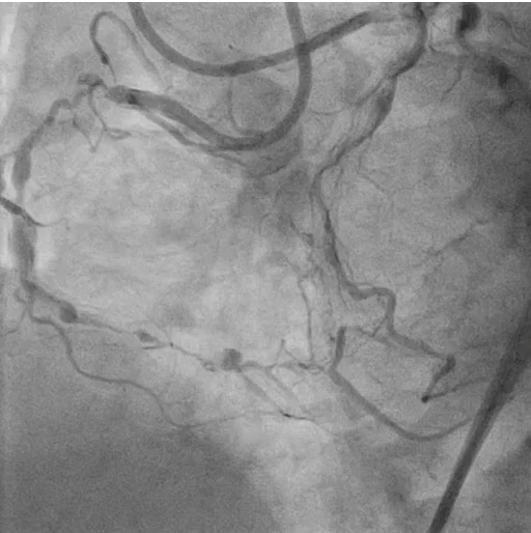
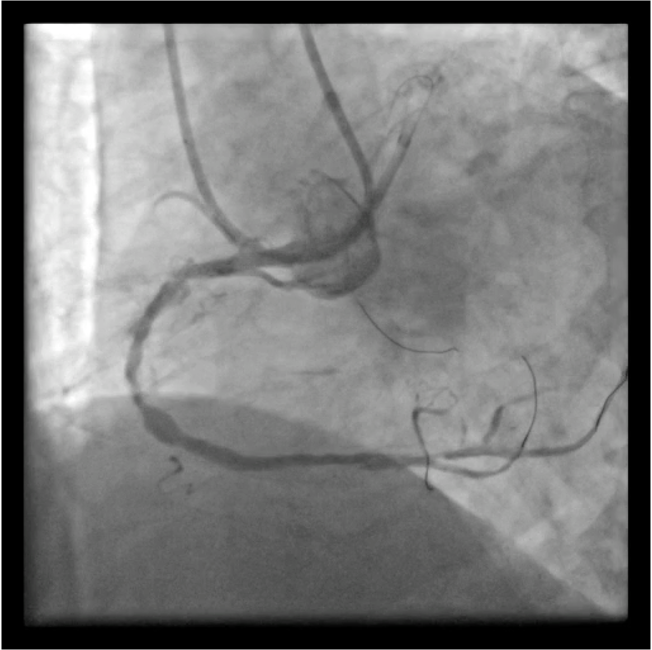
Coronary angiogram result were as follow: (Figure A, Figure B & Figure C))
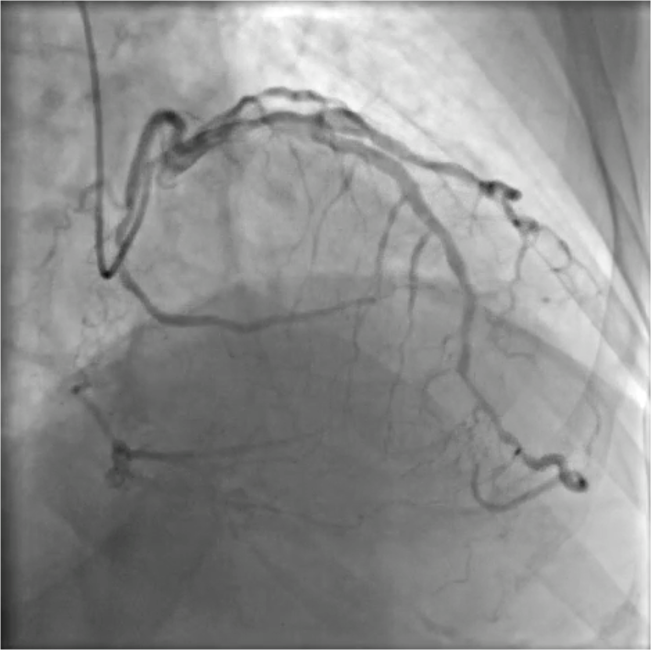
- Patent left main;
- Proximal LAD 50% stenosis with heavy calcification
- Distal LAD 70% diffuse stenosis
- Septal collaterals to PDA
- Mid LCX stent patent
- Distal LCX 70% segmental stenosis
- Epicardial AV groove collateral to PL
- Proximal RCA total occlusion with bridging collateral to mid portion
Interventional Management
Procedural Step
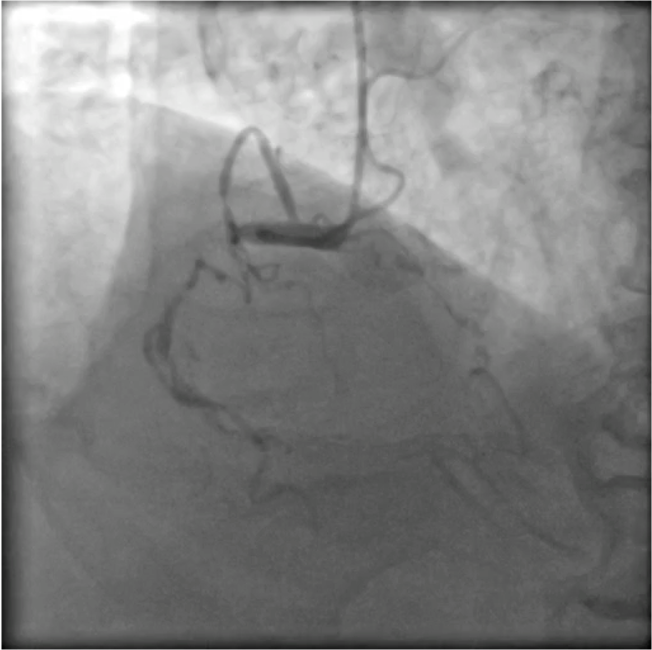
By the support of EBU 3.5/7F and AL 1.0/7F, advanced Sion GW & Finecross MC into epicardial collateral channel.Tried to advance SUHO-3, Sion and FielderFC GWs but failed & noted contrast extravasation.
Case Summary
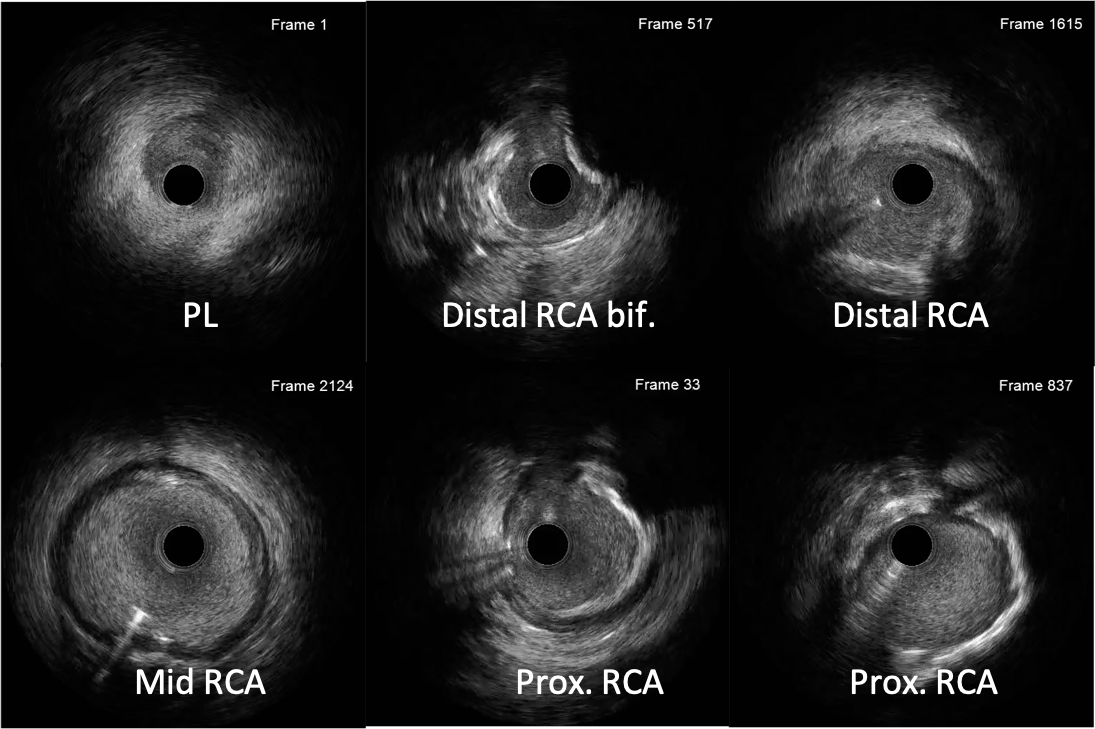
We present a challenging CTO PCI case. As previously deployed stents were in subintimal space, we choose primary retrograde approach in order to recannalize true lumen. Unfortunately, attempts via collateral channels was failed. So, antegrade approach was performed with the support of micro catheter and dual lumen catheter. IVUS analysis confirmed wire position in true lumen. 1 DES was deployed at mid RCA and DCB balloon angioplasty was done for mid to distal RCA segments. Procedure was complicated with distal RCA perforation which was successfully treated by stent.