
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-055
Lets Save the Heart : A Complex Coronary Intervention in a Patient With Distal Left Main Stenosis and Heart Failure With Reduced Ejection Fraction
By Kumutha Gobal, Muhamad Ali SK Abdul Kader, Adelyn Nisha Henry, Vicknesan Kulasingham, Gurudevan Mahadevan, Tee Choon Keong
Presenter
Kumutha Gobal
Authors
Kumutha Gobal1, Muhamad Ali SK Abdul Kader2, Adelyn Nisha Henry1, Vicknesan Kulasingham3, Gurudevan Mahadevan1, Tee Choon Keong1
Affiliation
Sultanah Aminah Hospital, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, Ministry of Health Malaysia, Malaysia3,
View Study Report
TCTAP C-055
CORONARY - Bifurcation/Left Main Diseases and Intervention
Lets Save the Heart : A Complex Coronary Intervention in a Patient With Distal Left Main Stenosis and Heart Failure With Reduced Ejection Fraction
Kumutha Gobal1, Muhamad Ali SK Abdul Kader2, Adelyn Nisha Henry1, Vicknesan Kulasingham3, Gurudevan Mahadevan1, Tee Choon Keong1
Sultanah Aminah Hospital, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, Ministry of Health Malaysia, Malaysia3,
Clinical Information
Patient initials or Identifier Number
JJ
Relevant Clinical History and Physical Exam
70 years old malay gentleman, with background history of T2DM and Hypertension. Patient is an ex smoker. He is under the heart failure clinic follow up for heart failure reduced ejection fraction secondary to ischemic dilated cardiomyopathy. Clinically patient is in CCS class I and NYHA class II. A myocardial perfusion scan shows a significant inducible ischemia along the LAD and RCA/PDA territory with viable myocardial tissues and suggested for coronary intervention.
BP : 146/81
HR : 90bpm
Relevant Test Results Prior to Catheterization
Hb/PLT/WCC : 12.7/260/8.9
BUSE/Creat : 4.8/138/4.2/108/110
FBS : 8.7
Triglyceride/T.Chol/LDL/ : 3.2/5.7/3.1
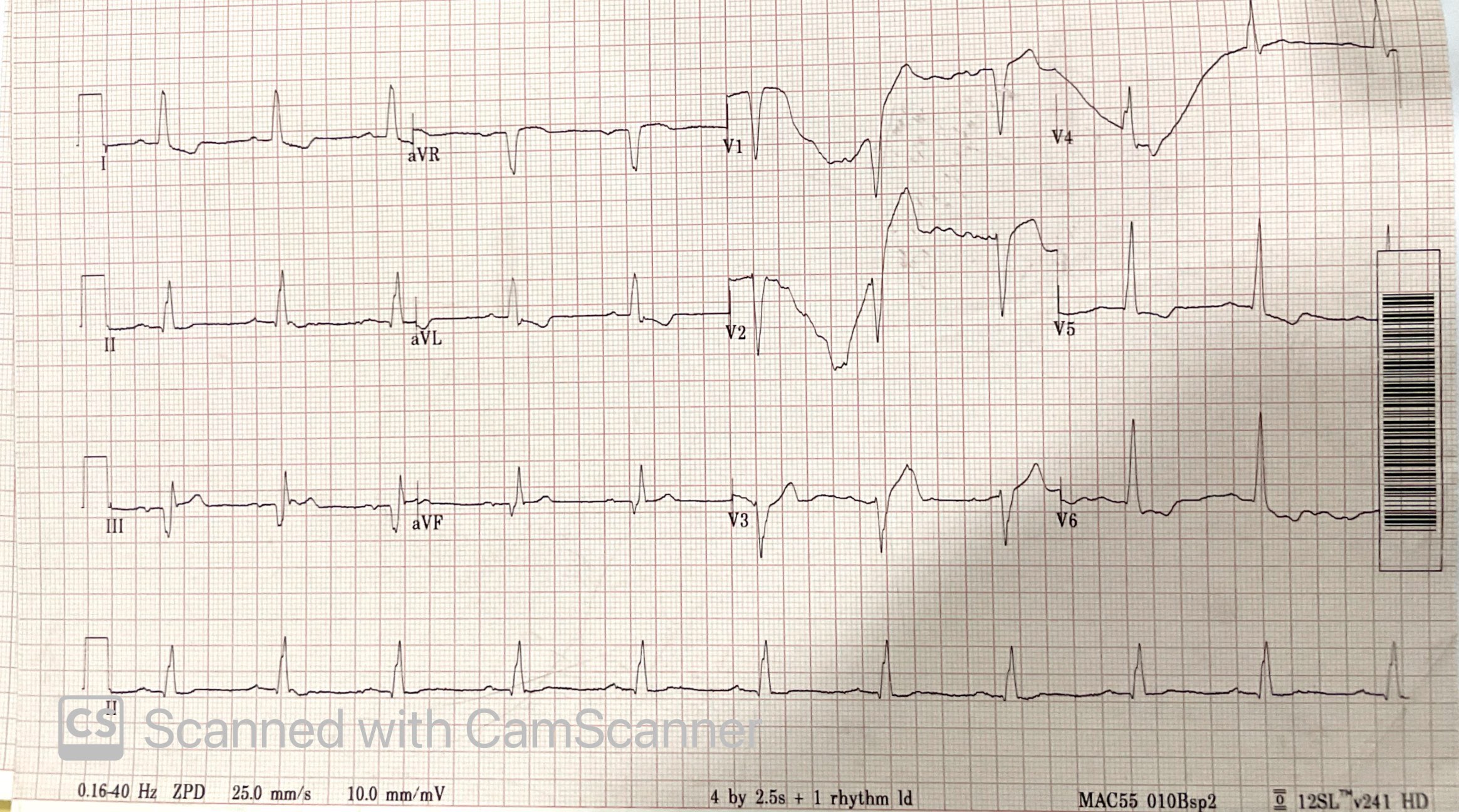
ECG : Sinus rhythm, ST depression I, avL, V4-V6, Q waves in II,III,avF
CXRay : Clear
Echocardiogram : LVEF 20-25%, hypokinesia over anterior and inferior wall, LA/LV dilated, no pericardial effusion, no thrombus.
Relevant Catheterization Findings
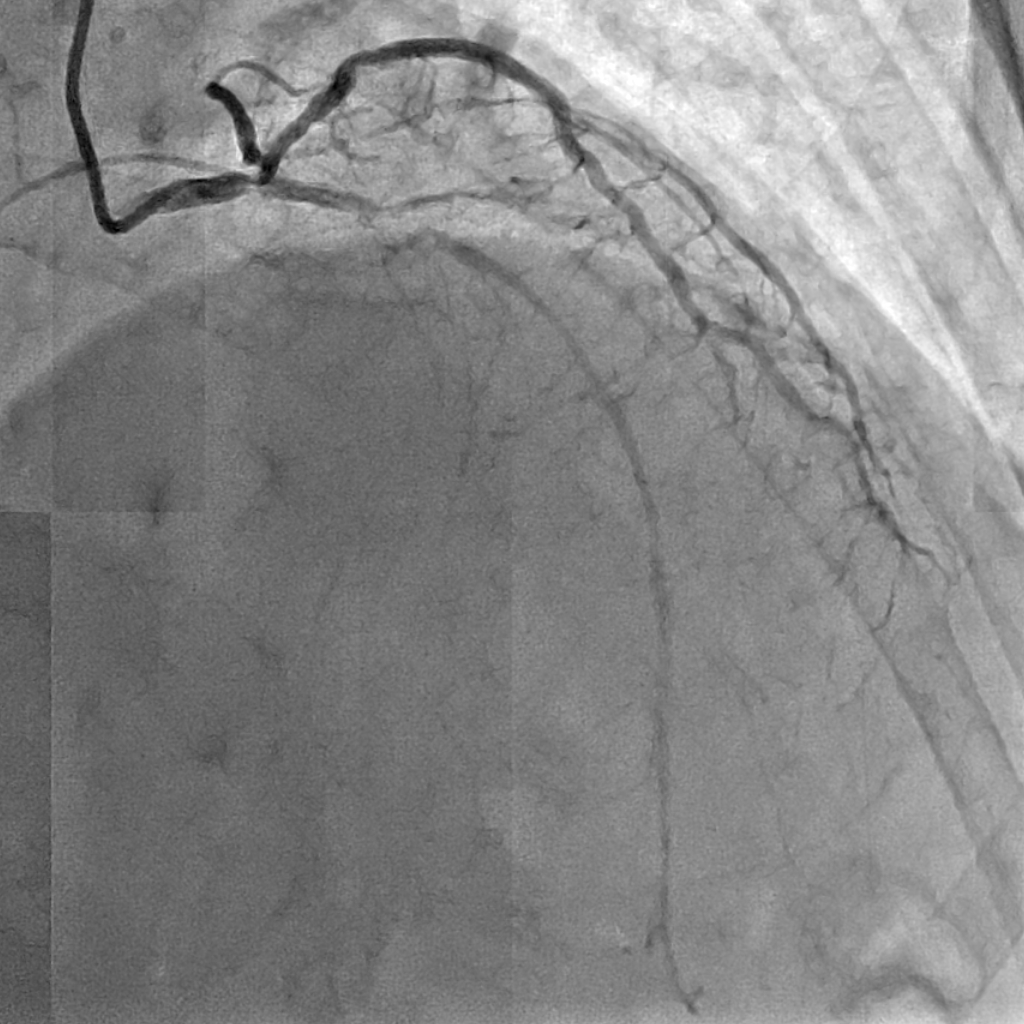
Left system

 laocraright00001.jpg
laocraright00001.jpg
-------------
Distal Left Main : 90% stenosis
Ostial LAD : 70-80% stenosis
Mid LAD : CTO
Ostial LCX 70-80% stenosis
Mid LCX : 80% stenosis
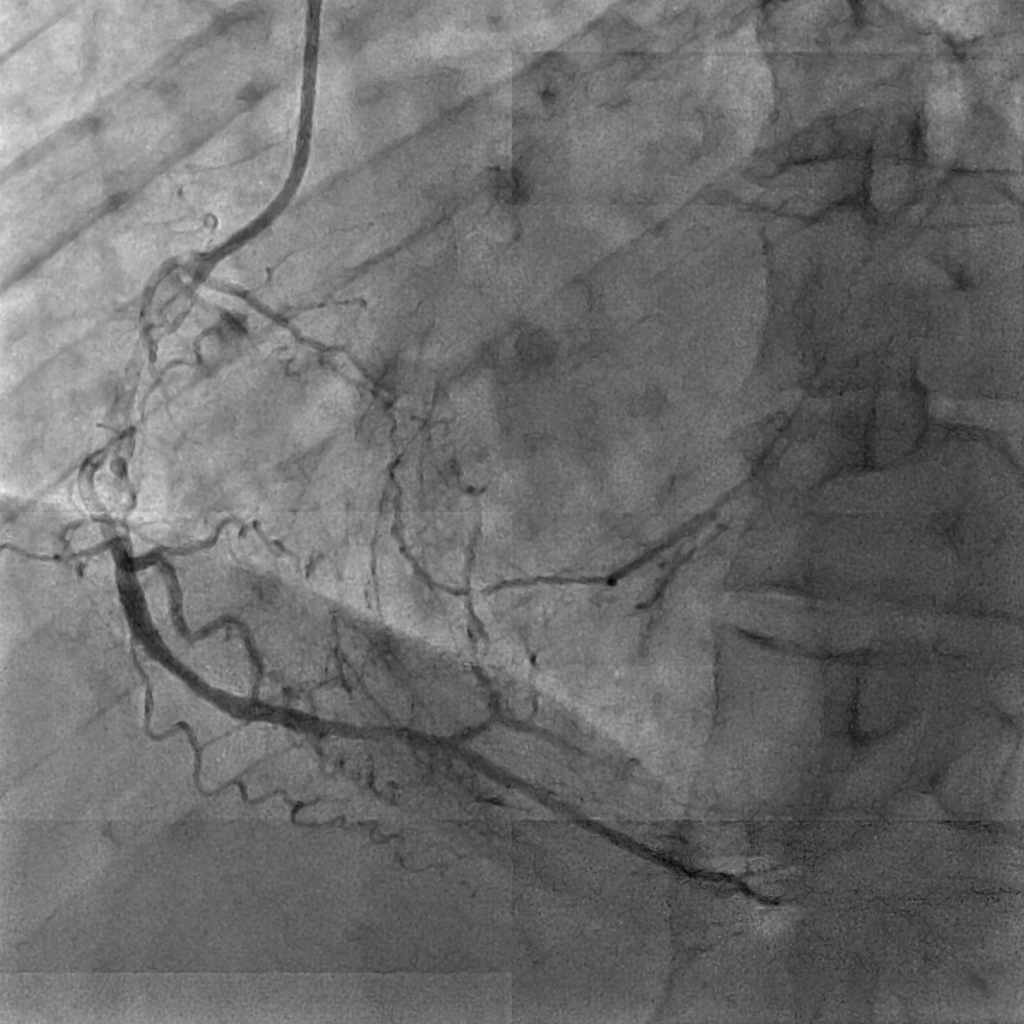
Right system (providing collaterals to the LAD)
---------------
Proximal RCA : 70-80%
Mid RCA : Subtotal Occlusion
Interventional Management
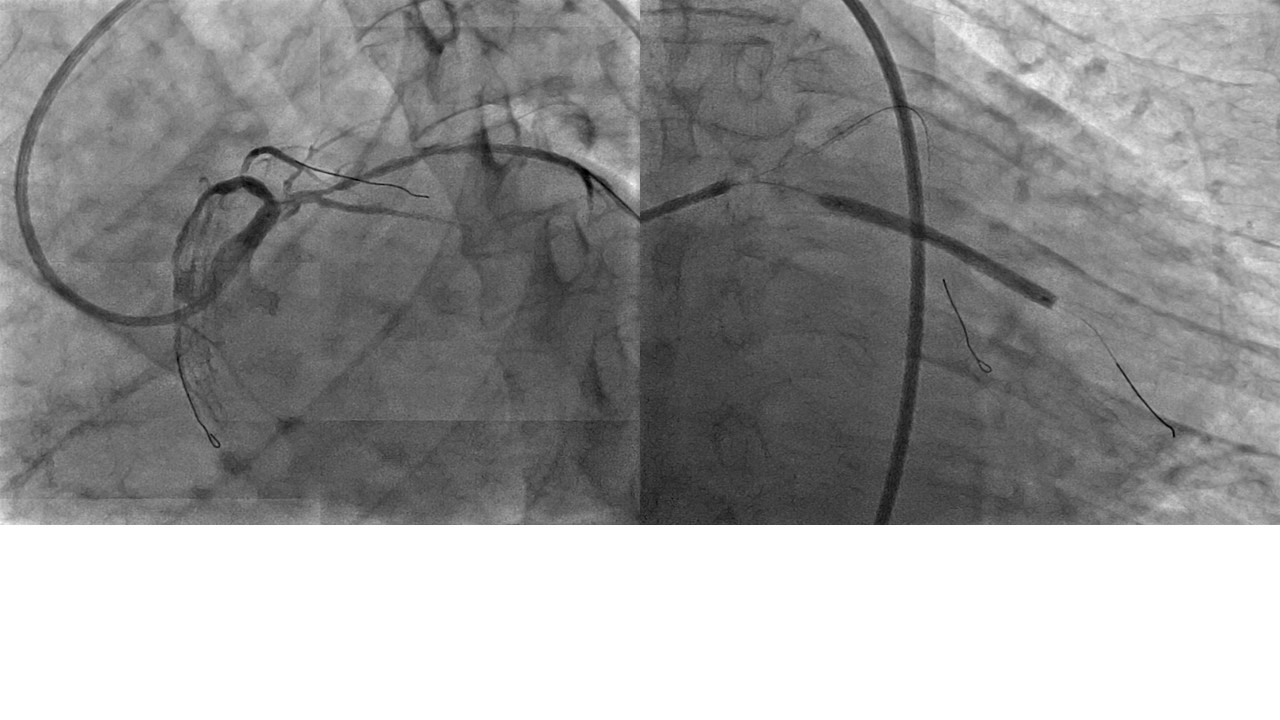
Procedural Step
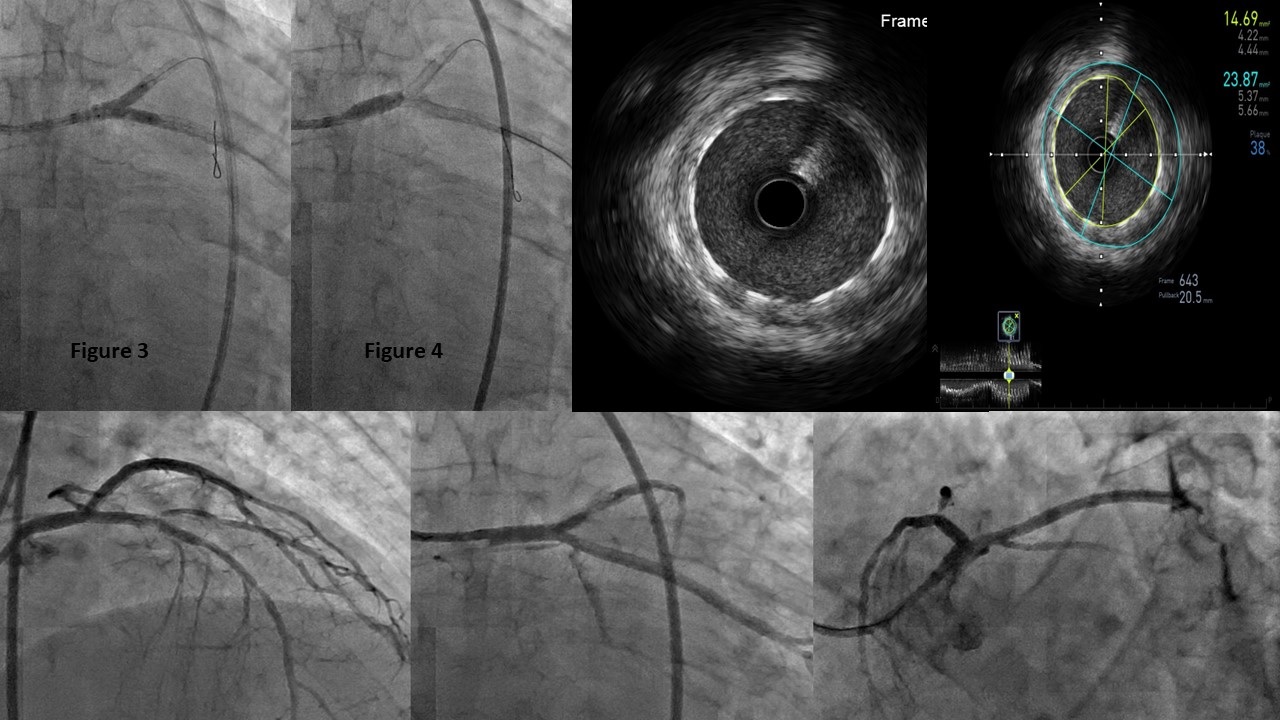
Engaged LCA using 7Fr EBU 3.5 guiding catheter via left femoral artery, wire the LAD using a microcatheter with Gaia 3 wire and subsequently switched to Runthrough wire and wire the LCX with sion blue.Predilated LAD with 2.0x15mm NC balloon(Fig 1), post predilatation noted pinching of ostial D1, wired the D1 and POBA with same NC balloon. Stented the proximal LAD with Firehawk 3.5x18mm.Predilated LCX with 3.0x15mm NC balloon(Fig 2). Stented the proximal to mid LCX with Firehawk 3.5x38mm. Subsequently stented the ostial LCX with Firehawk 3.5x21mm with T-stenting technique. Kissing ballooninflation done with NC 3.5x15mm in LCX and NC 3.0x15mm in LAD . Followed by LM-LAD stenting with Firehawk 3.5x26mm. Proximal optimization technique at LM using NC 4.0x10mm at high pressure. Then done final kissing balloon inflation with 3.5x15mm NC balloon(Fig 3). IVUS showed well opposed stent over the LM/LAD.Final proximal optimization done with NC 4.5x10mm at LM(Fig 4). Repeat IVUS showed stents are very well opposed, good MSA and no distal stent edge dissection. Good angiographic results(Fig 5) with TIMI 3 flow.

Case Summary
This is a case of a patient having a tight distal left main lesion with reduced left ventricular function, who remained remained stable through out procedure. Hence proper planning and advocating a safe strategy (ie T stenting/kissing balloon/POT) is vital. Patient was well through out the hospital stay and is planned for a stage PCI to the RCA in 3 months time.