
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-121
Expect the Unexpected and Be Prepared.
By Mohd Khairi Othman, Siti Aisyah Hussin, Muhammad Nabil Alhanis Ab Kadir, Zurkurnai Yusof, W Yus Haniff W Isa
Presenter
Mohd Khairi Othman
Authors
Mohd Khairi Othman1, Siti Aisyah Hussin2, Muhammad Nabil Alhanis Ab Kadir2, Zurkurnai Yusof1, W Yus Haniff W Isa1
Affiliation
Universiti Sains Malaysia Hospital, Malaysia1, Hospital Universiti Sains Malaysia, Malaysia2,
View Study Report
TCTAP C-121
CORONARY - Complications (Coronary)
Expect the Unexpected and Be Prepared.
Mohd Khairi Othman1, Siti Aisyah Hussin2, Muhammad Nabil Alhanis Ab Kadir2, Zurkurnai Yusof1, W Yus Haniff W Isa1
Universiti Sains Malaysia Hospital, Malaysia1, Hospital Universiti Sains Malaysia, Malaysia2,
Clinical Information
Patient initials or Identifier Number
HI
Relevant Clinical History and Physical Exam
72 years old man with underlying hypertension and dyslipidemia. He had been complaint of sudden onset central chest pain for 1 day prior to admission. The pain describe as crushing in nature with pain score 6/10. The pain associated with diaphoresis and nausea. Further history reveal that he had been complaint intermittent chest pain for 3 months duration with CCS class III.On clinical examination, his blood pressure 178/89 mmHg and pulse rate 92 bpm. Others are unremarkable.
Relevant Test Results Prior to Catheterization
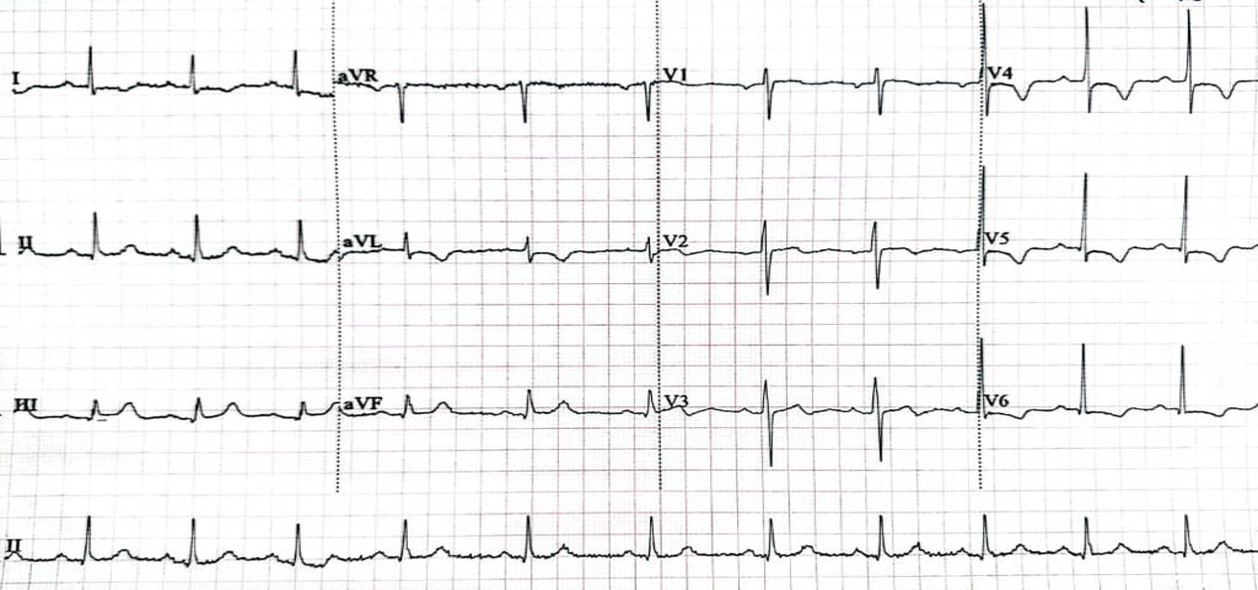
His hsTroponin leve 16ng/l ( <14 ng/l) and LDL level was 3.52 mmol/l. His electrocardiogram showed sinus rhythm with T inversion in lateral lead. Echocardiography showed normal left ventricular ejection fraction with no regional wall motion abnormalities.
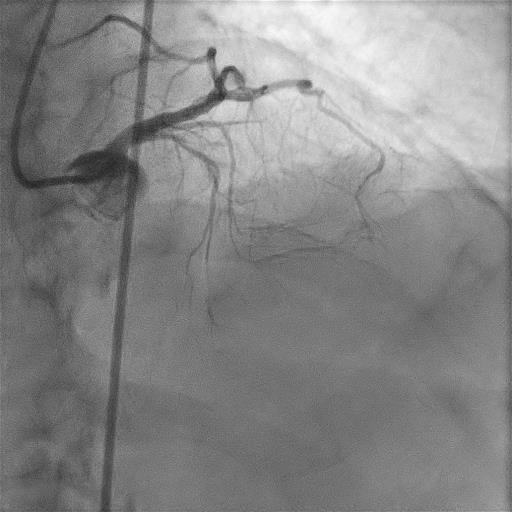
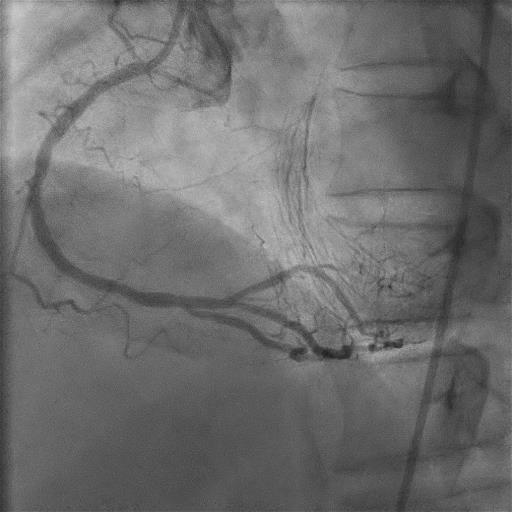
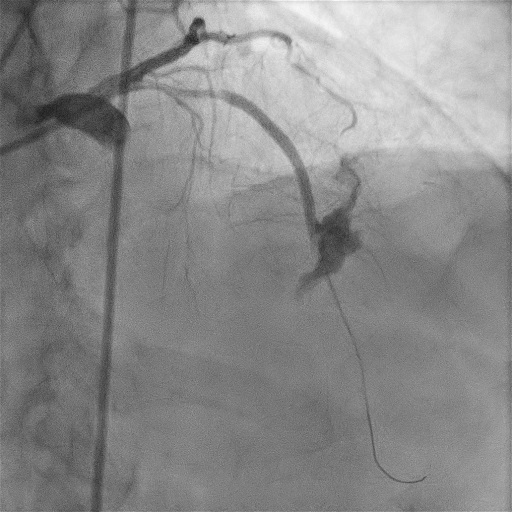
Relevant Catheterization Findings
Interventional Management
Procedural Step
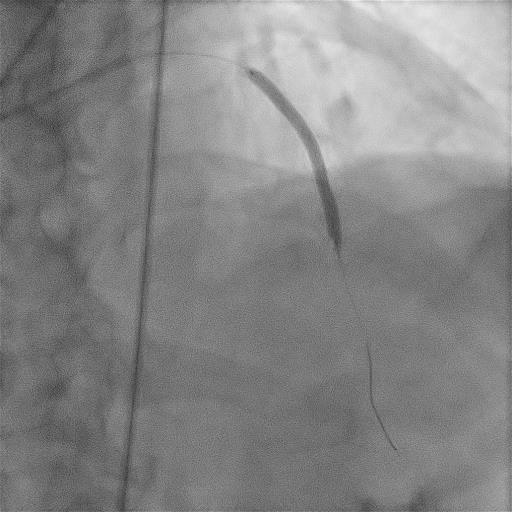
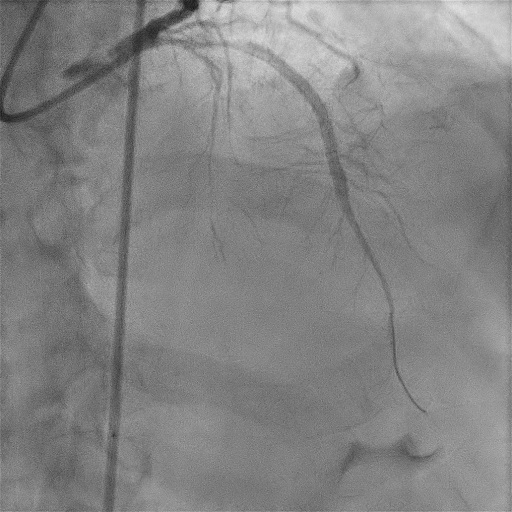
The right radial artery was punctured, and the LAD wa sengaged with 6Fr CLS 3.5 guiding catheter. Whisper extra support wire was first used however not able to cross the proximal LAD CTO. It was parked in the first septal perforator. GAIA second wire were introduced and managed to cross the proximal LAD CTO and advanced to distal LAD. Proximal LAD up to mid LAD was predilated with Ryurei 1.25x10mm followed by Sapphire 3 2.00x10mm at 10-14 atm. First stenting to mid-LAD lesion using Promus Premier 3.00x38mm was done. After contrast injection, noted perforation at distal end of mid LAD stent and immediately balloon tamponade for 10 minutes using stent balloon was done. Another contrast injection after balloon deflation showed no more leaking of contrast at distal end of mid LAD stent. Following that, stenting to proximal LAD was done Promus Premier 3.00x24mm without complication. While in recovery bay, the patient developed chest pain post-procedure, and echocardiography showed minimal pericardial effusion. Repeat coronary angiogram was done and showed patent stent with no contrast leak. The patient was then transferred to CCU for closed observation. He was subsequently diagnosed with acute pericarditis due to hemopericardium and treated with colchicine. Serial echocardiography showed pericardial effusion not worsening.
Case Summary
Coronary artery perforation is a rare complication associated with a percutaneous coronary intervention. Based on classification of coronary perforation, our patient is fall on Ellis class III. It is associated with pericardial effusion which potentiallly requiring pericardiocentesis. Coronary perforation post PCI commonly due to excessive overdilation or oversize stent size. In this condition, inital treatment include prolonged balloon stent inflation and usage of protamine sulphate for coagulation reversal. Covered stent, coils or fat can be used to causing tamponade at the site of perforation.