
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-127
A Complicated Case: When the Perforation Doesn’t Seal…
By Benjamin Tao Xiung Lim, Abdul Raqib Abd Ghani, Julian Tey, Meei Wah Chan, Asri Ranga
Presenter
Benjamin Tao Xiung Lim
Authors
Benjamin Tao Xiung Lim1, Abdul Raqib Abd Ghani1, Julian Tey1, Meei Wah Chan1, Asri Ranga2
Affiliation
Hospital Serdang, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2,
View Study Report
TCTAP C-127
CORONARY - Complications (Coronary)
A Complicated Case: When the Perforation Doesn’t Seal…
Benjamin Tao Xiung Lim1, Abdul Raqib Abd Ghani1, Julian Tey1, Meei Wah Chan1, Asri Ranga2
Hospital Serdang, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Mr NR
Relevant Clinical History and Physical Exam
A 46 year old Indian gentleman with a history of lacunar stroke in February 2022 and ischaemic heart disease. In April 2022 COROS showed 2VD and PCI to RCA was done. He is still symptomatic with angina on exertion. He was planned for a stage PCI to CTO LAD. Physical examination was unremarkable.

Relevant Test Results Prior to Catheterization
ECG showed he was in sinus rhythm with Q waves present over the inferior leads with poor R wave progression over chest leads. Echocardiography revealed a dilated left ventricle with EF 40% and several areas of regional wall motion abnormalities.
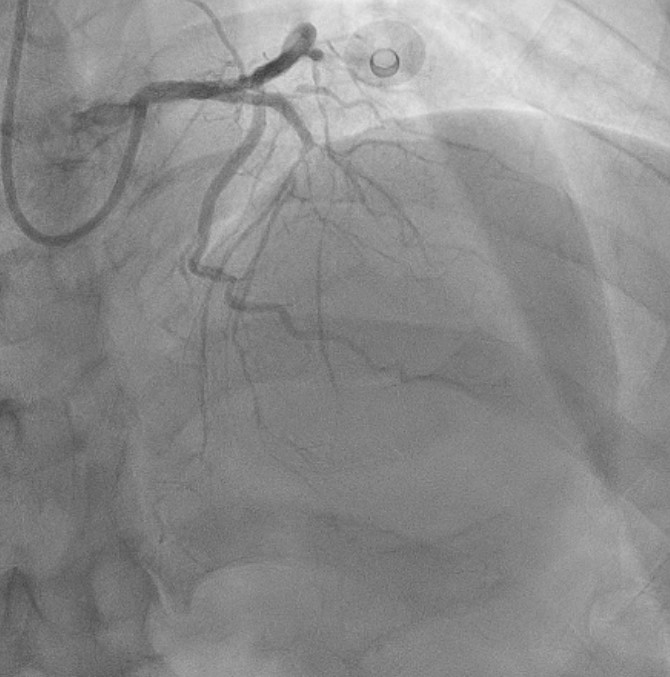
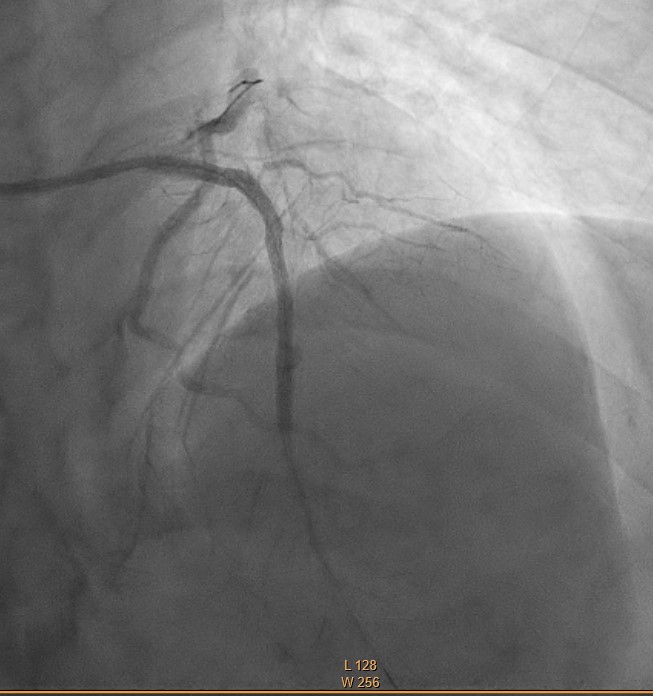
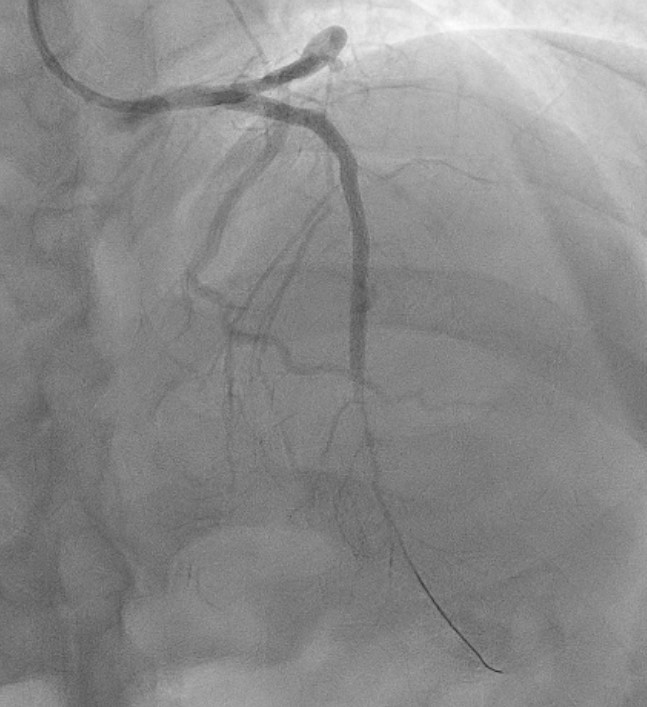
Relevant Catheterization Findings
Coronary angiogram done showed calcified 2 vessel disease with a dominant left system.
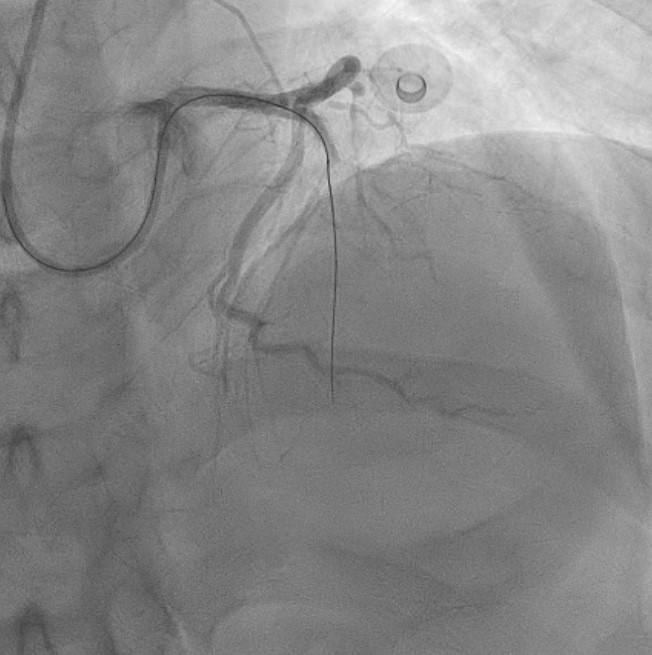
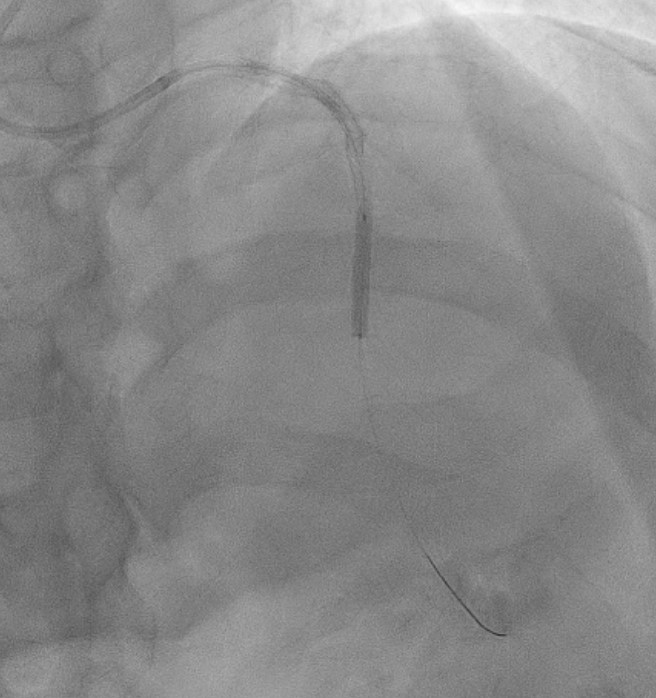
Interventional Management
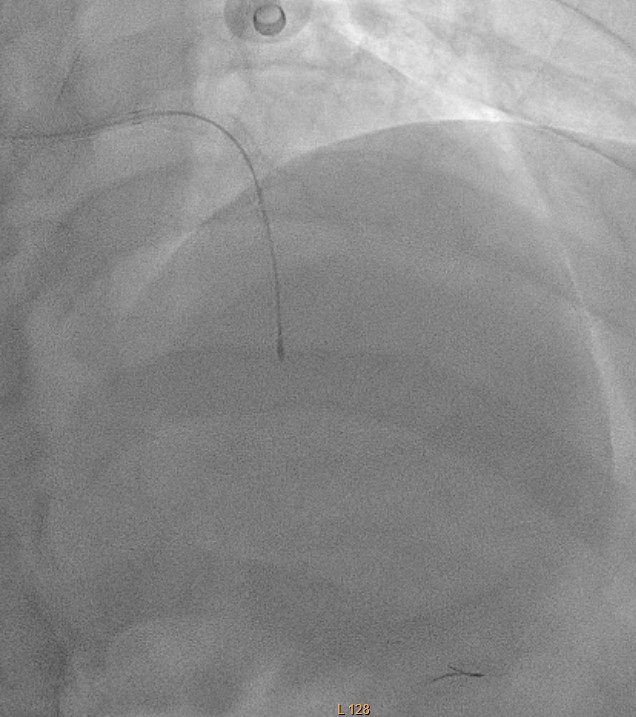
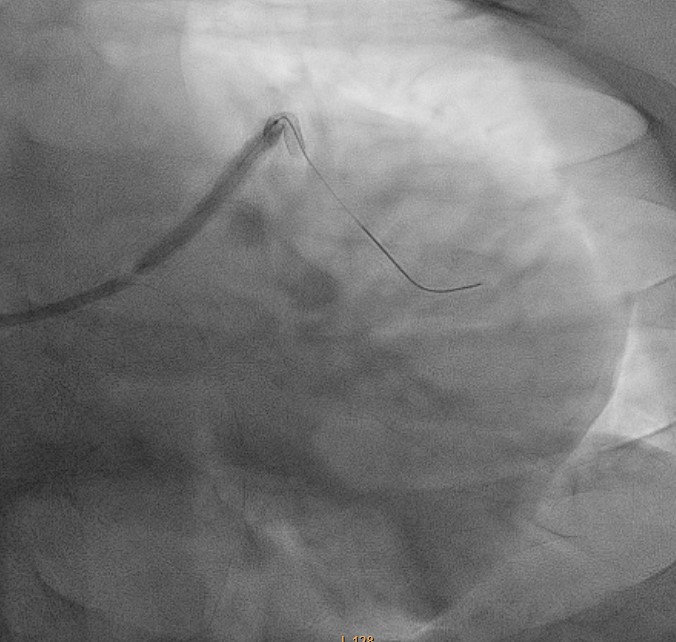
Procedural Step
EBU 3.5 6Fr engaged.
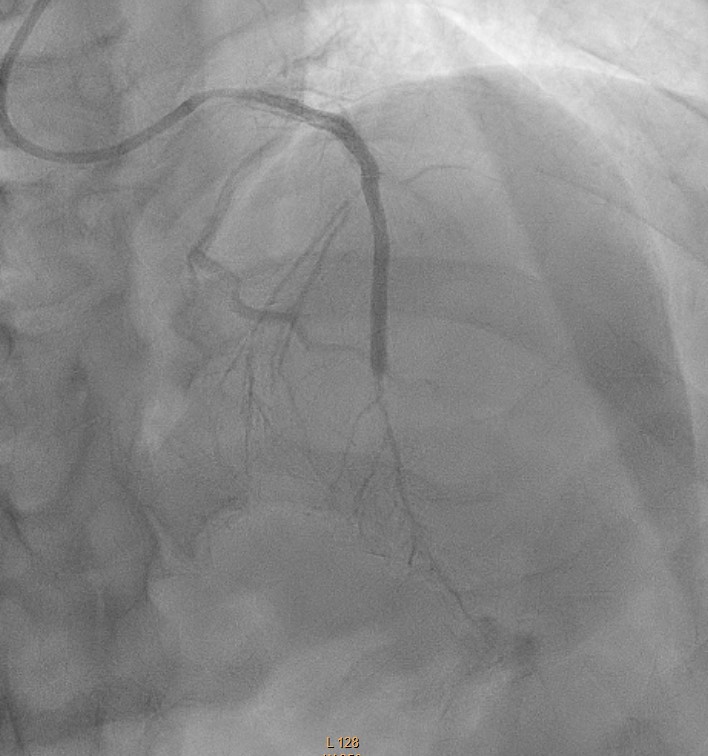
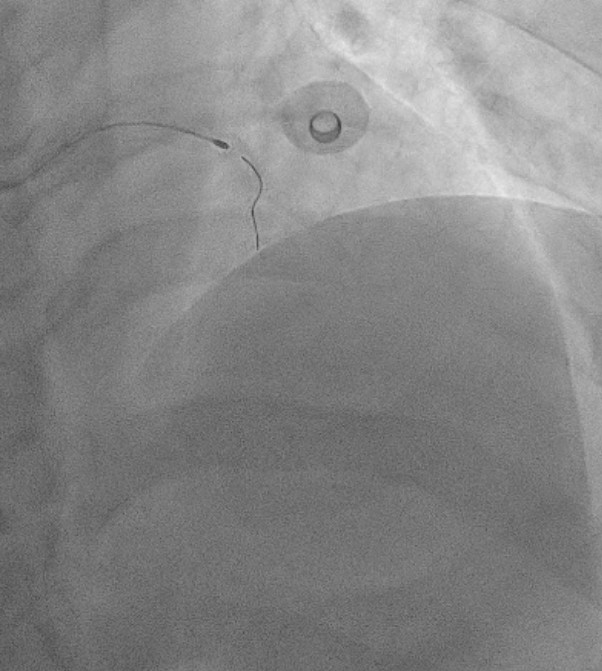
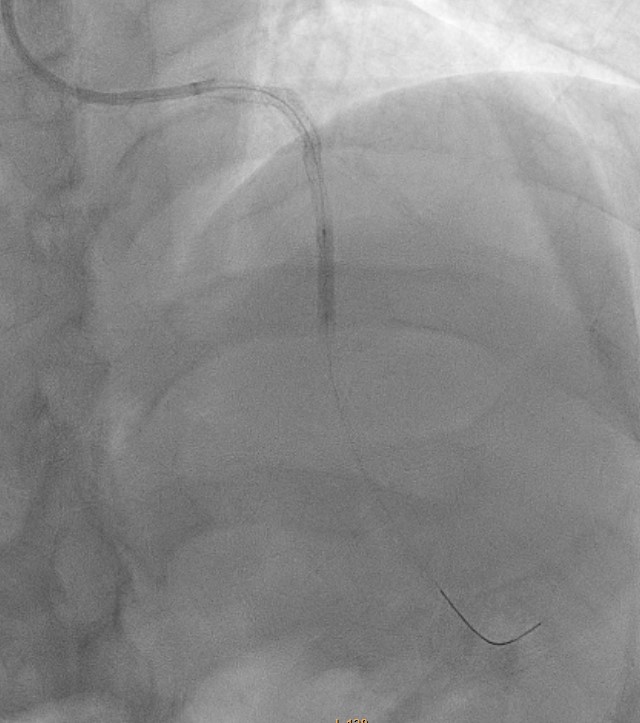
Case Summary
No further leaking noted.