
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-106
A Challenge Case Report: A 51-Year-Old Man With Acute Coronary Syndrome
By Ching-Yu Hsiao, Chih-Fan Yeh
Presenter
CHING-YU HSIAO
Authors
Ching-Yu Hsiao1, Chih-Fan Yeh1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-106
CORONARY - Complications (Coronary)
A Challenge Case Report: A 51-Year-Old Man With Acute Coronary Syndrome
Ching-Yu Hsiao1, Chih-Fan Yeh1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
6620504
Relevant Clinical History and Physical Exam
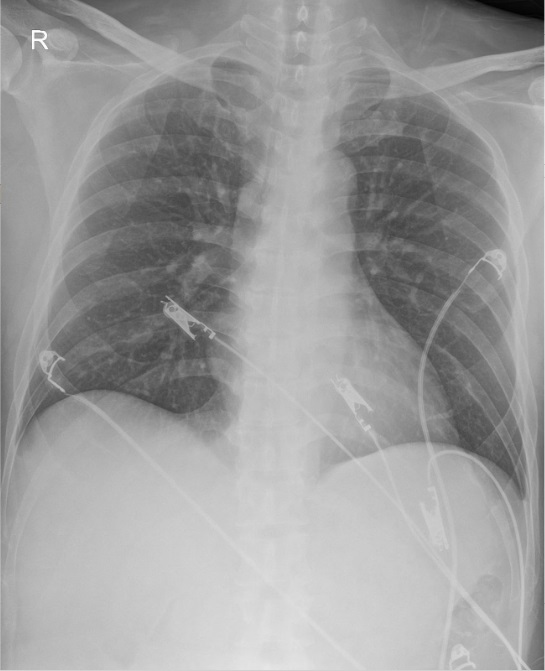
A 51-year-old man with past history of hyperlipidemia. He smoked 0.5 PPD for 30 years. One month prior to admission, the patient suffered from shortness of breath with exercise intolerence. One week prior to admission, he had intermittent chest tightness with bilateral shoulder pain and shortness of breath. He visited ER due to progressive chest pain.Ill-looking with cold sweats. Regular heart beats with no audible murmur.
Relevant Test Results Prior to Catheterization
Hb 16.9 g/dL, WBC 13.36 k/μL, PLT 339 k/μLTroponin-T 272.8 ng/L (0 hr), cre 1.5 mg/dL
UCG: LVEDD 41 mm, LVESD 28 mm. LVEF(MOD-bp) 63%. Regional wall motion abnormality (basal septal hypokinesia, basal inferior hypokinesia).
UCG: LVEDD 41 mm, LVESD 28 mm. LVEF(MOD-bp) 63%. Regional wall motion abnormality (basal septal hypokinesia, basal inferior hypokinesia).
Relevant Catheterization Findings
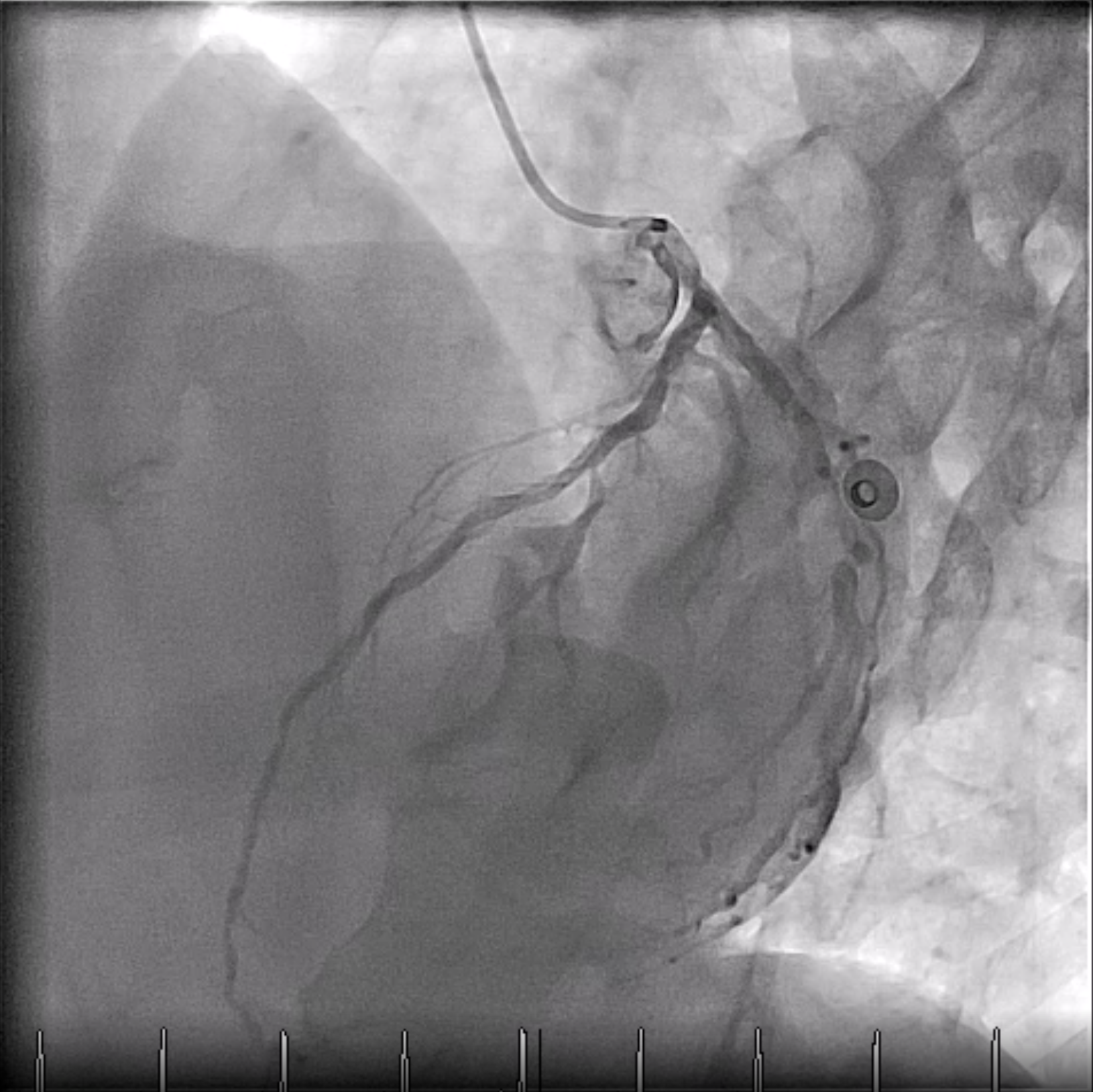
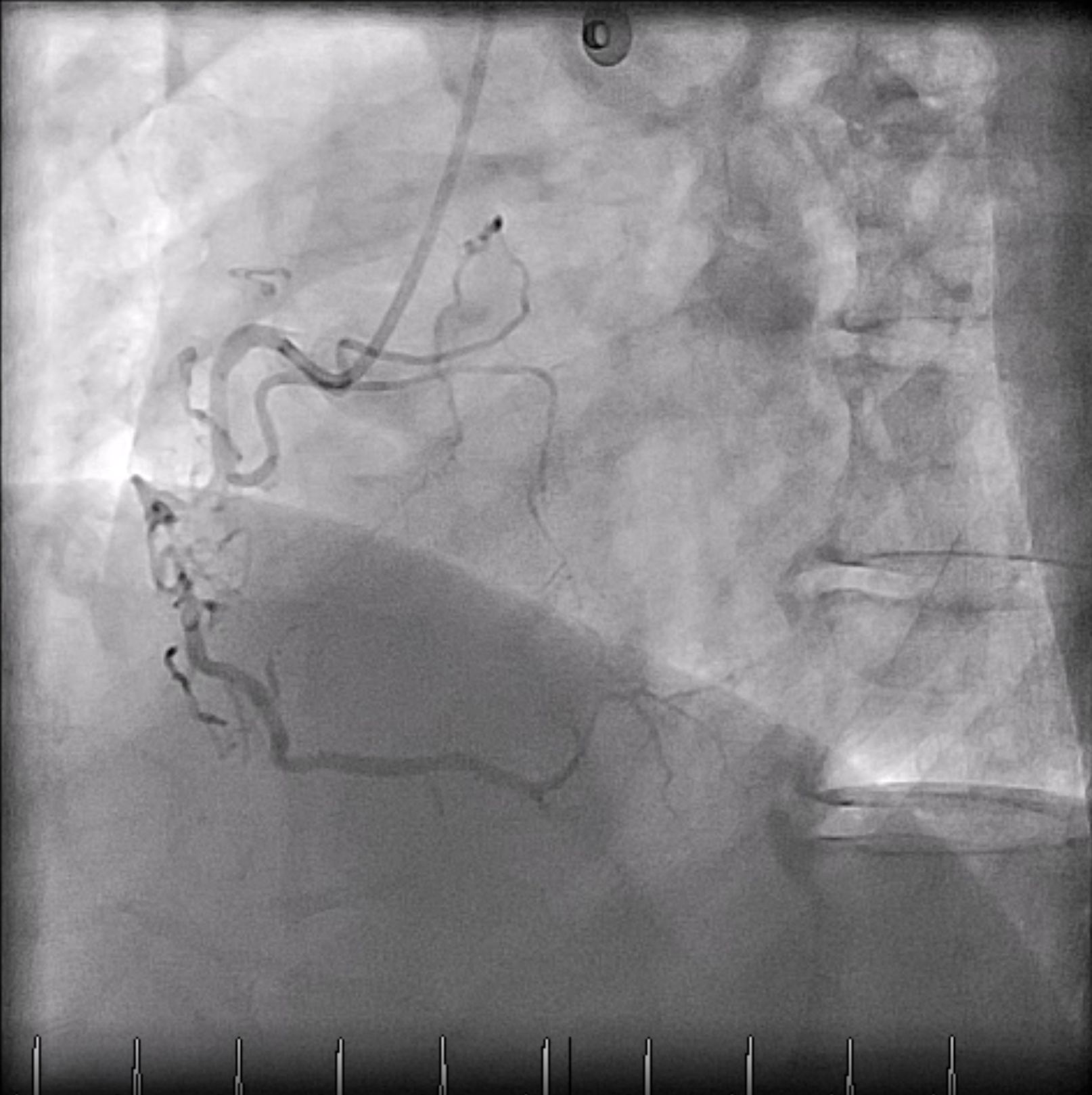
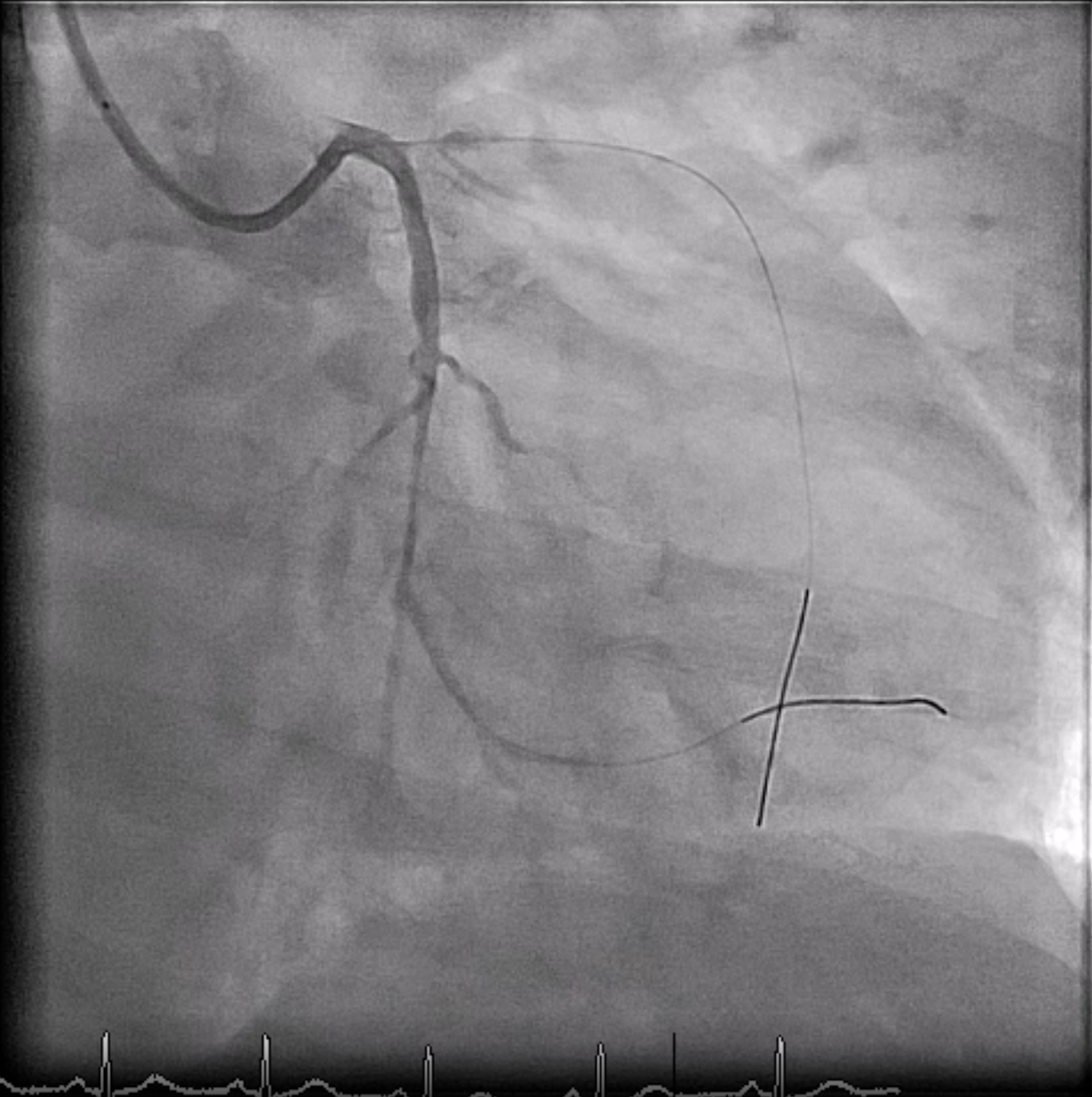
Coronary Angiography:LM: PatentLAD: ostial stenosis 95 %, D2 stenosis 80 %, distal stenosis 70 %LCX: distal stenosis 99 %, OM2 stenosis 70 %RCA: middle CTO, with bridging collateral

Interventional Management
Procedural Step
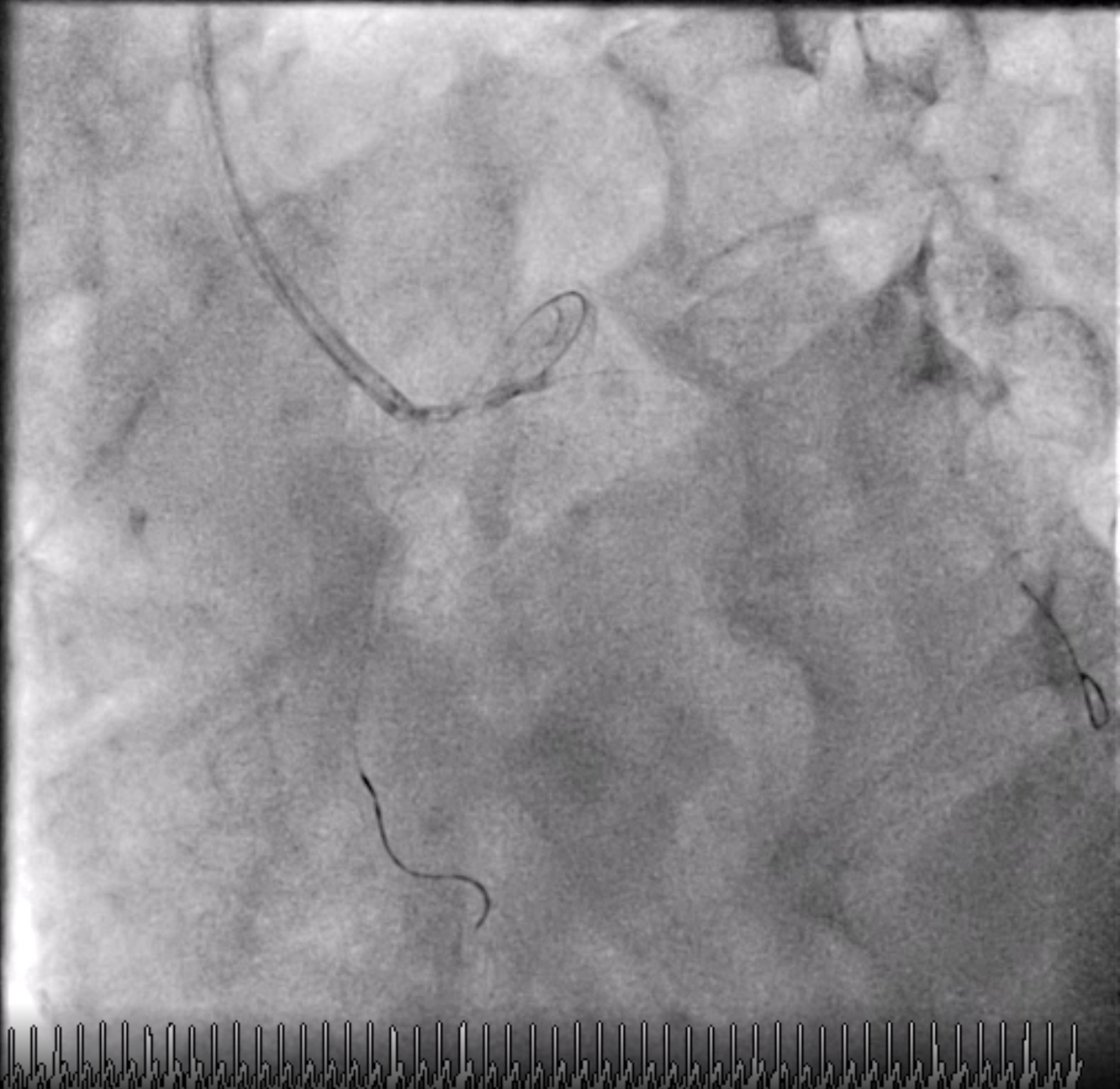
- Engaged GC to LCA and wired with GW1 to dLAD and GW2 to dLCx.- POBA at pLAD and dLCx.- Checked IVUS at LCX.- POBA at dLCx.- STE with hypotension was noted. Levophed was given. Angiogram showed compromised flow of LAD.- POBA at pLAD. LAD flow was restored.- Checked IVUS at LAD.- Angiogram showed dLCX flow was compromised.- Failed to advance balloon catheter to dLCX. Wired with GW3 to dLCX. Removed GW2.- POBA at dLCX. dLCX flow was restored.- Deployed DES1 "BIOTRONIK ORSIRO-2.5*40mm " at p-dLCX.- Angiogram showed LAD flow was compromised.- Deployed DES2 "Terumo stent Ultimaster 3.5*18mm " at LM-LAD. LAD flow was restored.- Checked IVUS at LAD, which showed stent underexpansion.- Post dilated at DES2.- Wired with GW2 to dLCX. Performed balloon angioplasty at LM-LCX for strut opening. Removed GW3. Post dilatated at DES1.- Angiogram showed thrombus at pLAD.- POBA at pLAD. dLAD flow was restored. However, thrombus was shifted to LCX ostium.- IVUS at LCX showed good stent expansion, but thrombus at LCX ostium was noted.- POBA at LM-LCX.- Failed to deliver DES to pLCX. DES was dislodged at LM-LCX.- Performed stent retrieval with coronary snare with success.- Rewired to LCX and LAD. Deployed DES3 "Terumo stent Ultimaster 3.5*15mm " at LM-LCX.- IVUS at LM-LCX showed stent under expansion.- Post dilated at LM-LCX.- Angiogram showed thrombus at pLAD.- Performed kissing balloon at LM-LAD-LCX bifurcation.- IVUS at LCX, LAD showed good stent expansion.- Final show was good. We closed the procedure.

Case Summary
This is a case of acute coronary syndrome. During primary coronary intervention, multiple thrombosis at different sites and different time was encountered. Treatment plan was reformed accordingly. Newly developed ST elevation after thrombosis was noted and cardiogenic shock ensued. Stent dislodge at left main artery further complicated the situation. All thrombotic events and mechanical complication were managed timely. We closed the procedure smoothly under stable condition of the patient.