
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-085
Total Occlusion With Ostial Dissection Simultaneously Happened in Right Coronary Artery With Diffuse Calcification
By Chiao-Chin Lee, Yen-Lien Chou
Presenter
Chiao-Chin Lee
Authors
Chiao-Chin Lee1, Yen-Lien Chou1
Affiliation
Tri-Service General Hospital, Taiwan1,
View Study Report
TCTAP C-085
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Total Occlusion With Ostial Dissection Simultaneously Happened in Right Coronary Artery With Diffuse Calcification
Chiao-Chin Lee1, Yen-Lien Chou1
Tri-Service General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
3372228
Relevant Clinical History and Physical Exam
A 89 Male


Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
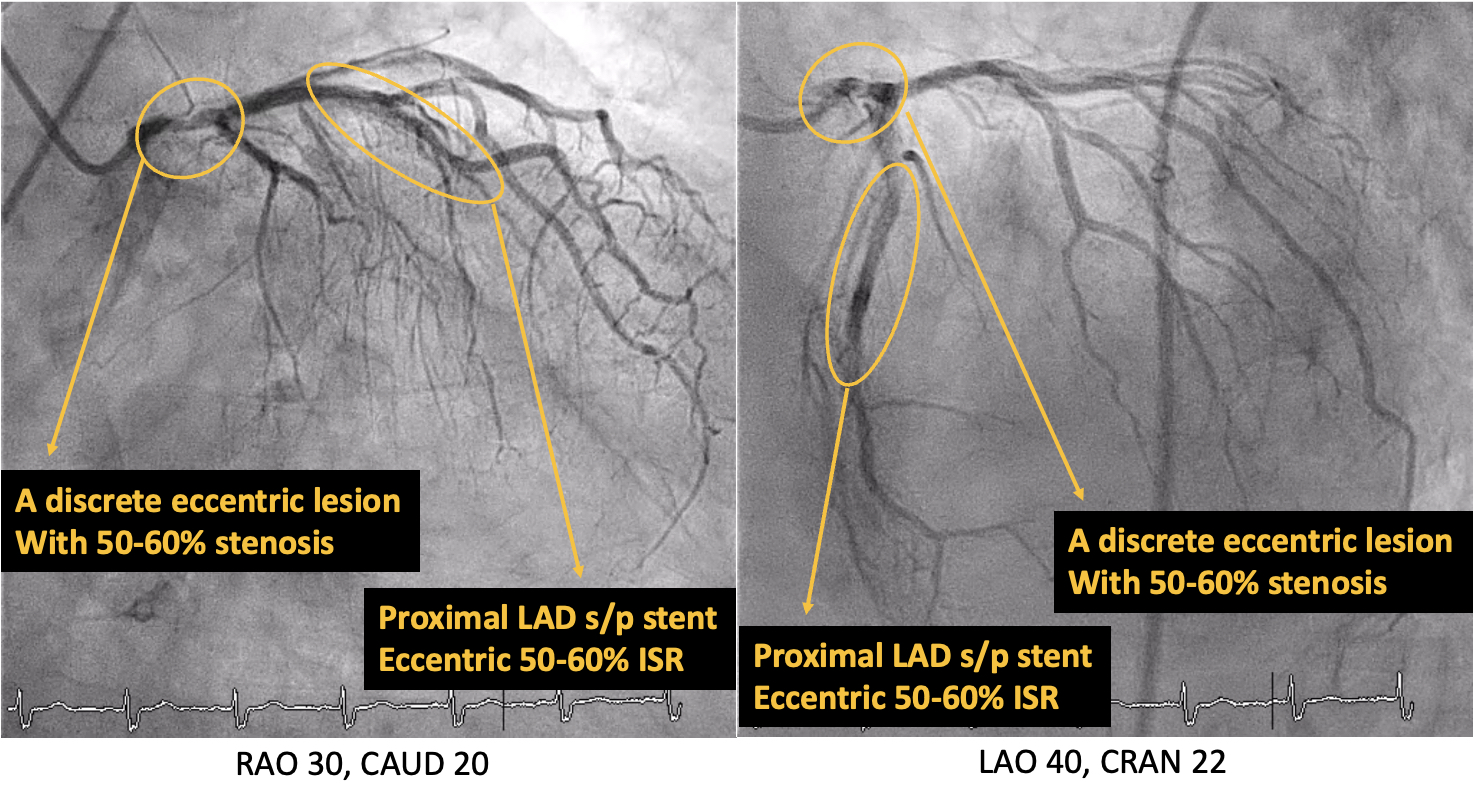
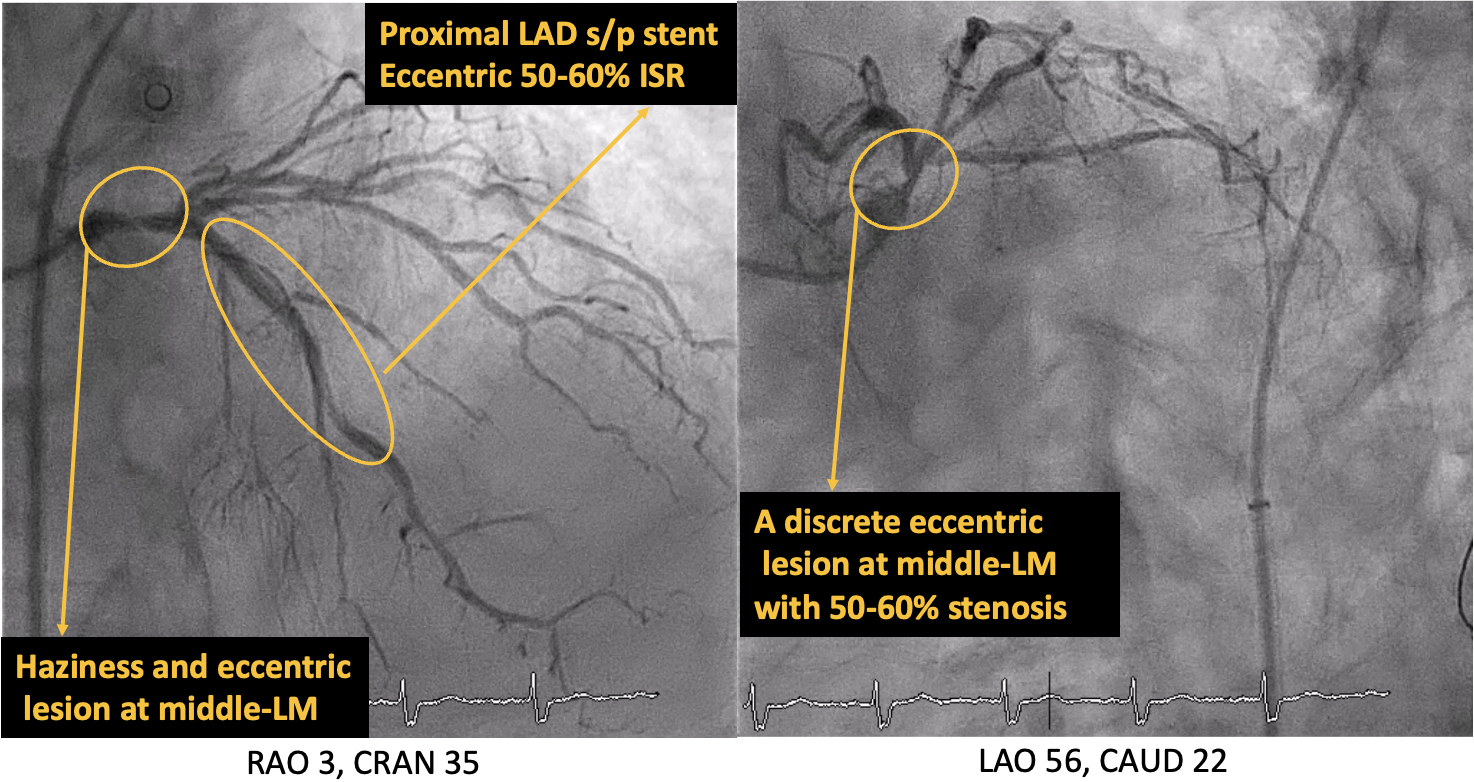
LM: A discrete 50-60% eccentric stenosis lesion at M/3
Interventional Management
Procedural Step
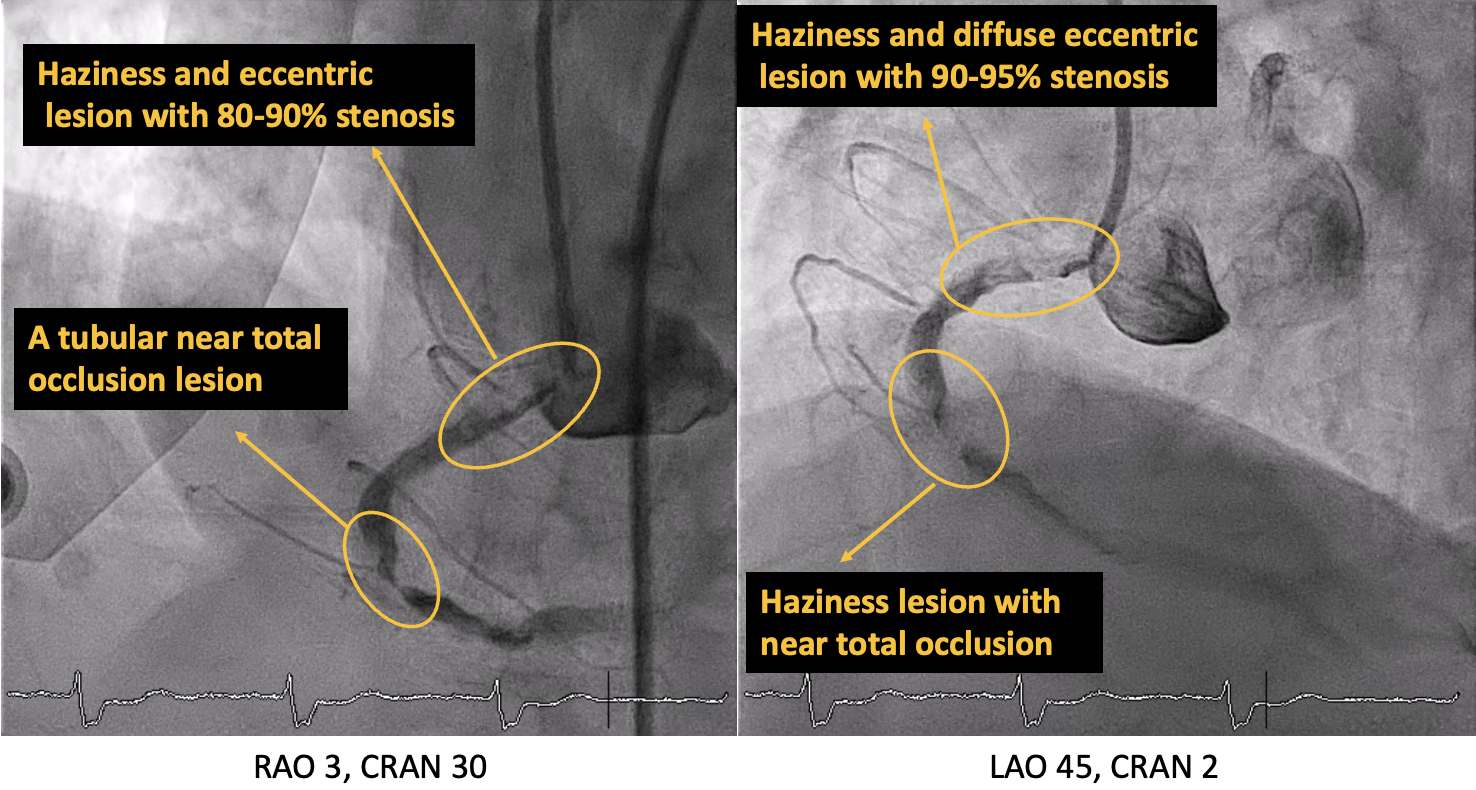
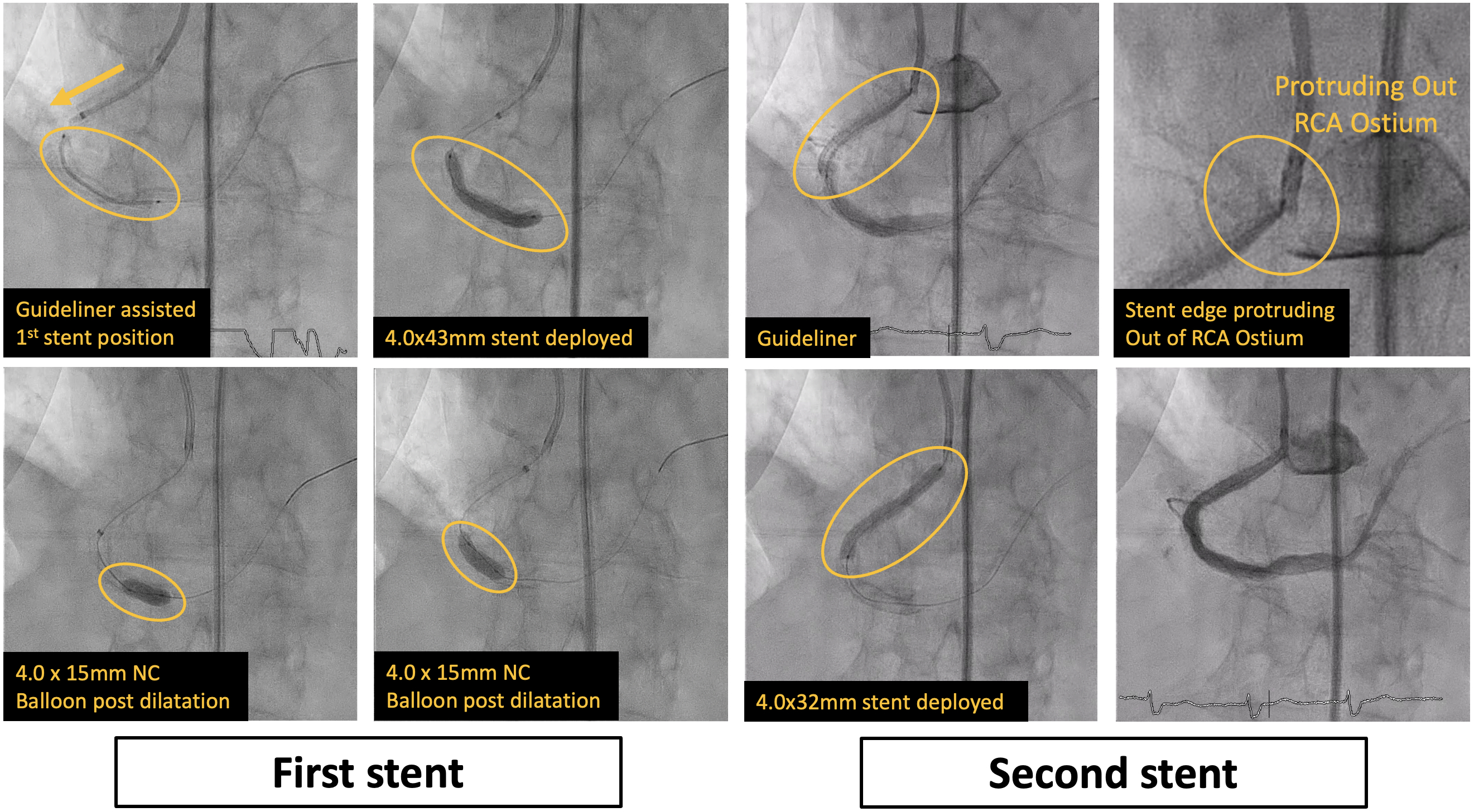
-The RCA ostium was engaged by SAL 1.0 guiding catheter.-A SION Black wire in a FineCross microcatheter was used to wire through the critical stenotic lesion at m-RCA and advanced to PDA.
Case Summary
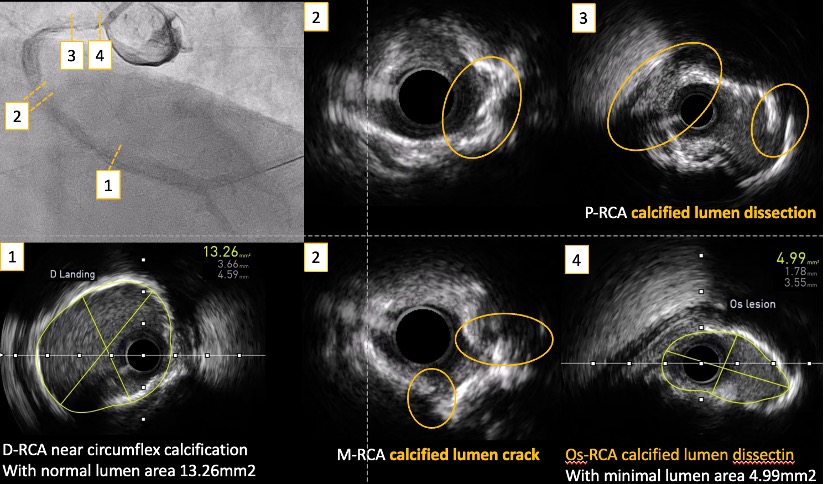
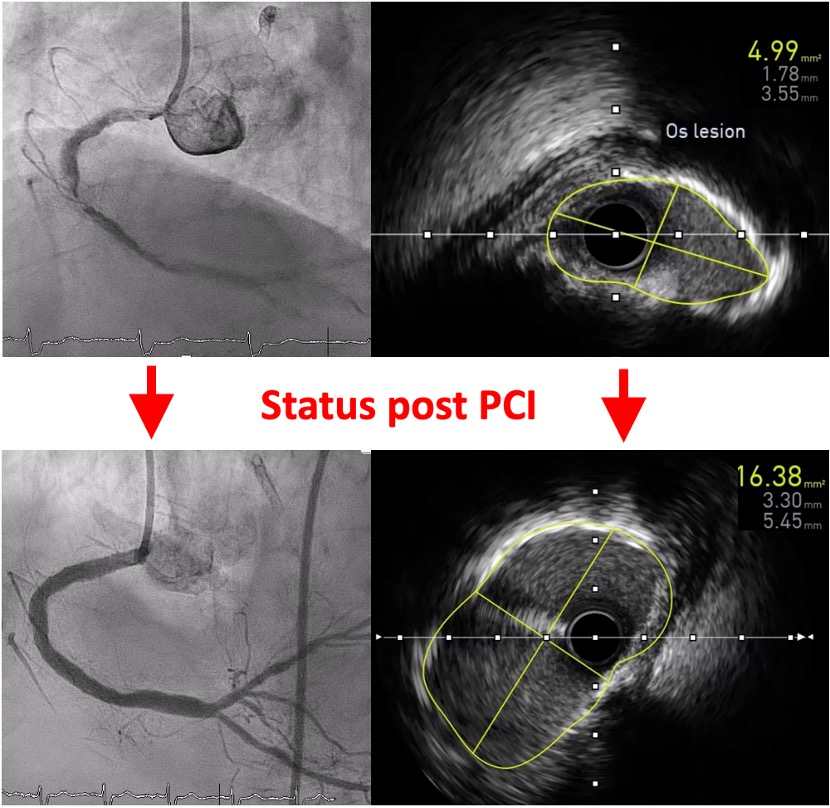
We present a CHIP case presenting with STEMI, inferior wall myocardial infarction, and culprit lesion at RCA. Mechanical support and temporary pacemaker always need to keep in mind to maintain the patient’s hemodynamic status when encountering such as CHIP case. A good choice of guiding would make the whole procedure more safe and smoothly. Although it was a STEMI case, the intra-procedural image still played an important role when facing to the long diffuse calcified lesion. Dedicated calcification modification was essential and associated with stent expansion rate. It was practicable to deliver the Guideliner catheter into the dissection lesion under balloon assistance without further injury.