
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-071
An Unusual Etiology of Coronary Stent CTO
By Yu-Ling Hsu
Presenter
Yu-Ling Hsu
Authors
Yu-Ling Hsu1
Affiliation
National Chen Kung University Hospital, Taiwan1,
View Study Report
TCTAP C-071
CORONARY - Chronic Total Occlusion
An Unusual Etiology of Coronary Stent CTO
Yu-Ling Hsu1
National Chen Kung University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Mr. Lu
Relevant Clinical History and Physical Exam
A 47-year-old male was a smoker and had diagnosis of tongue cancer stage I in June 2021 in another hospital. When he received a pre-operative evaluation, the patient mentioned he had dyspnea on exertion for a long time and a chest pain event one year ago. Physical examination including the general appearance, breathing sound, and heart sound revealed unremarkable findings.
Relevant Test Results Prior to Catheterization
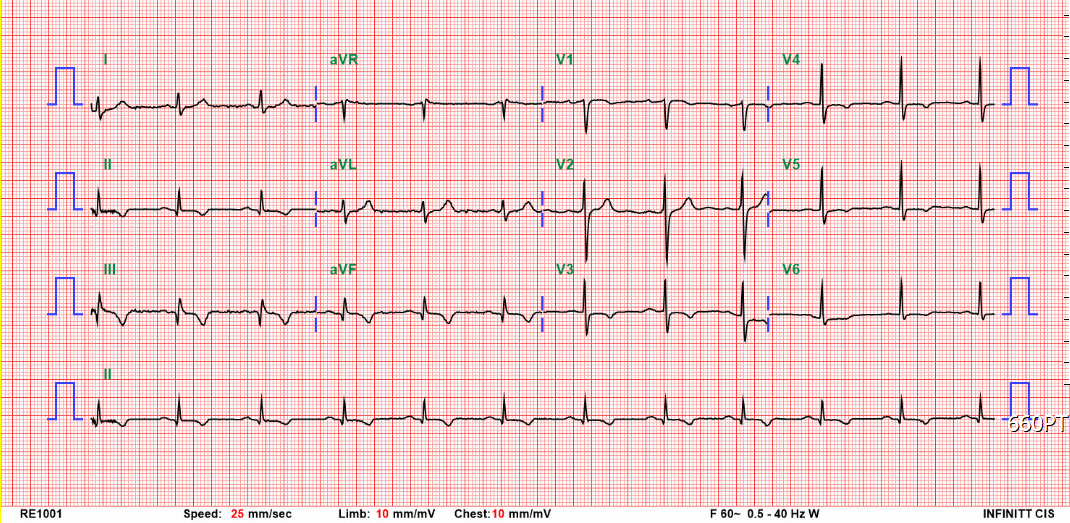
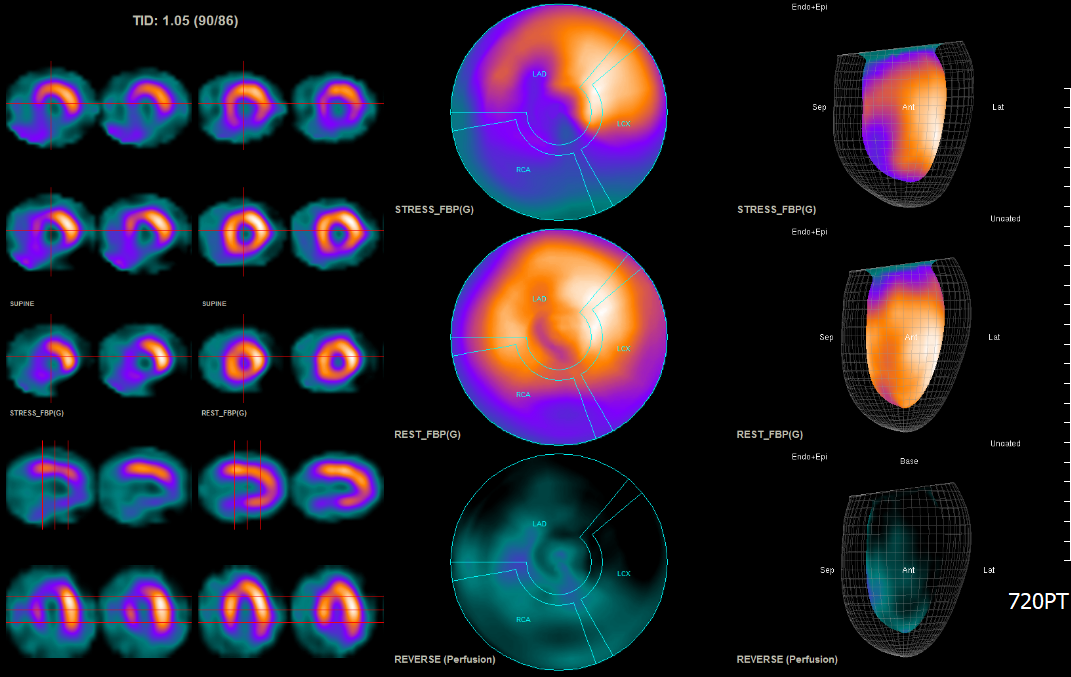
His chest X-ray showed no cardiomegaly. Electrocardiography revealed sinus rhythm with Q wave over the inferior leads. SPECT Dipyridamole stress test showed severe stress-induced ischemia in the apical-to-basal inferior, basal inferolateral, and mid-to-basal inferoseptal segments.
Relevant Catheterization Findings
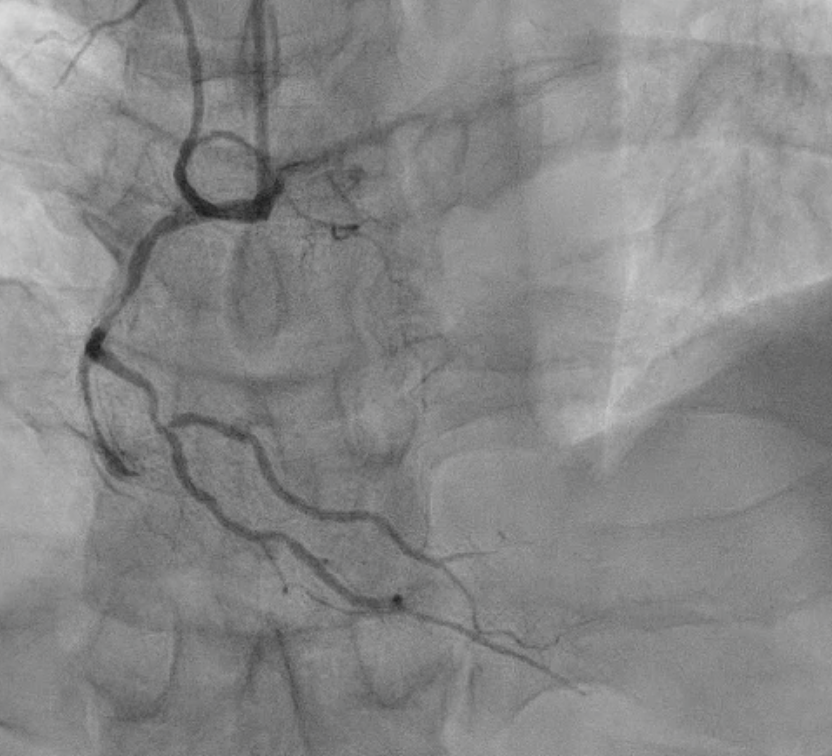
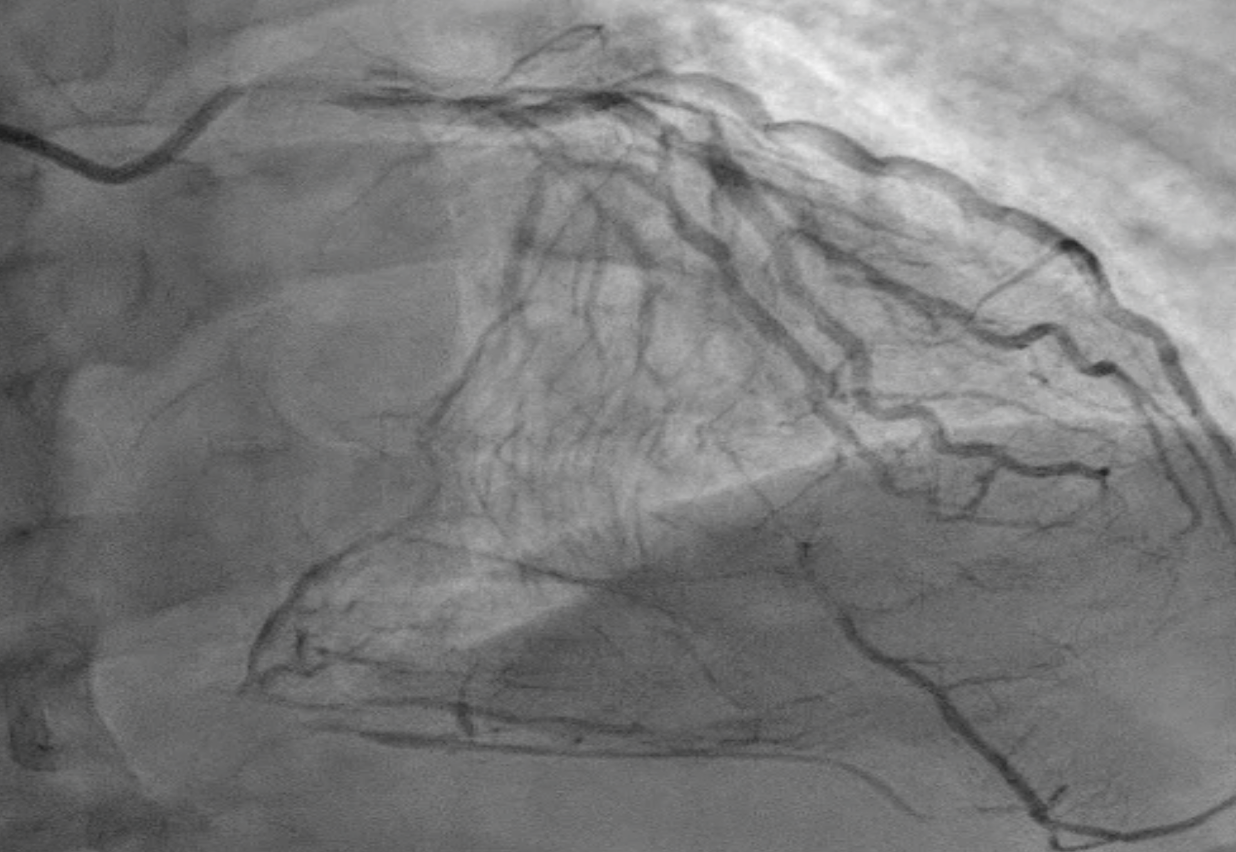
He received coronary angiography in June 2021 in another hospital which showed CAD/3VD, RCA total occlusion with collateral circulation from LAD and LCX; LAD total occlusion with collateral circulation from LCX and LCX insignificant stenosis. PCI for RCA was done with knuckle wire advanced to distal RCA without dual injection to check to distal wire position. A stent was deployed at m-dRCA. After 3 months, RCA ISR with total occlusion happened with collateral circulation from LAD.
Interventional Management
Procedural Step
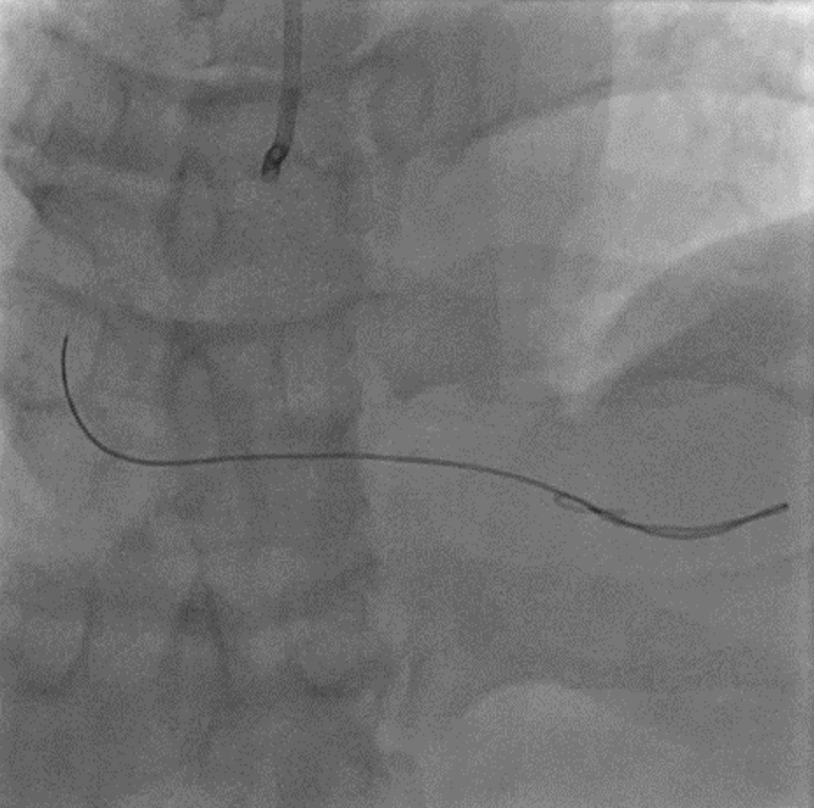
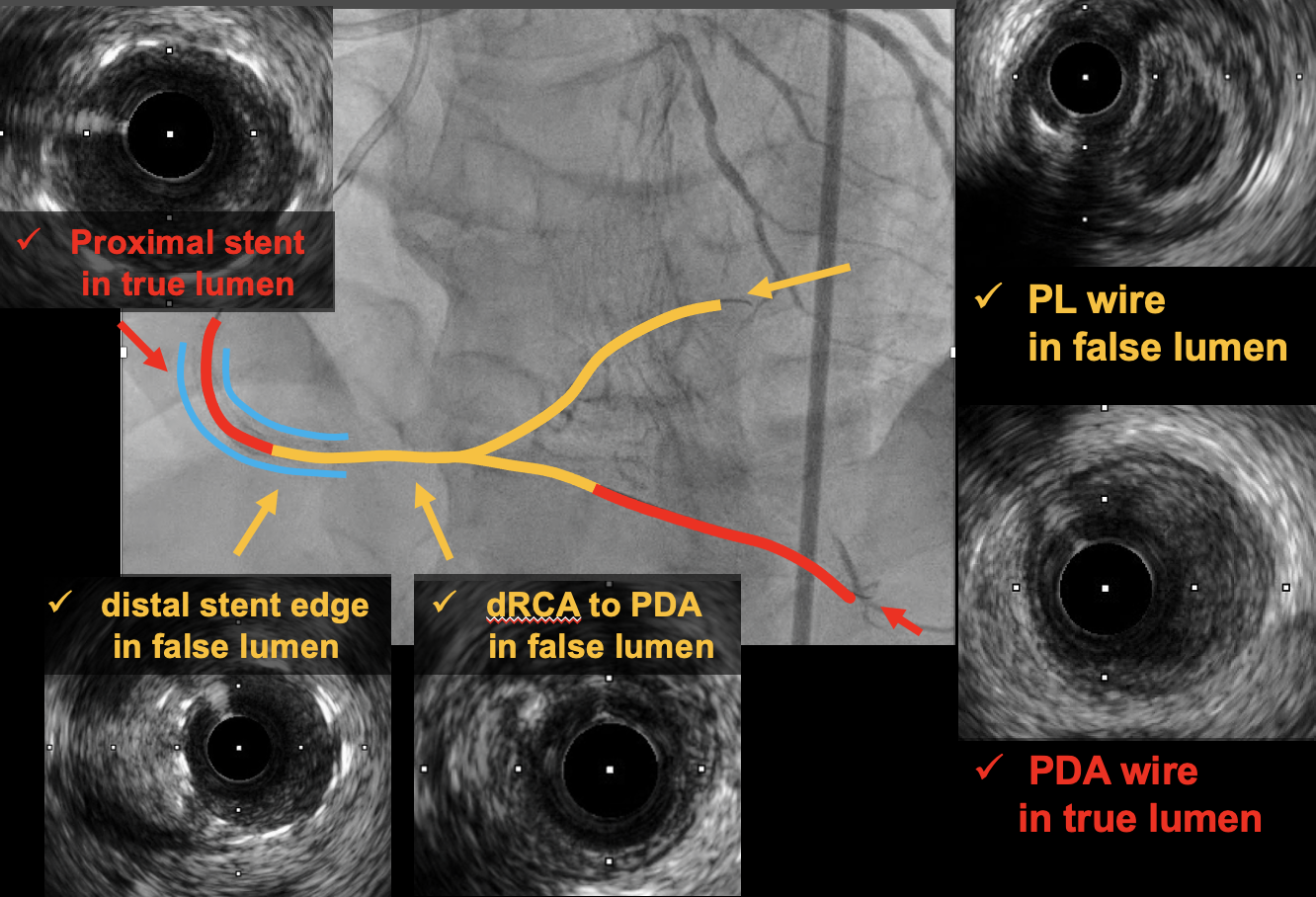
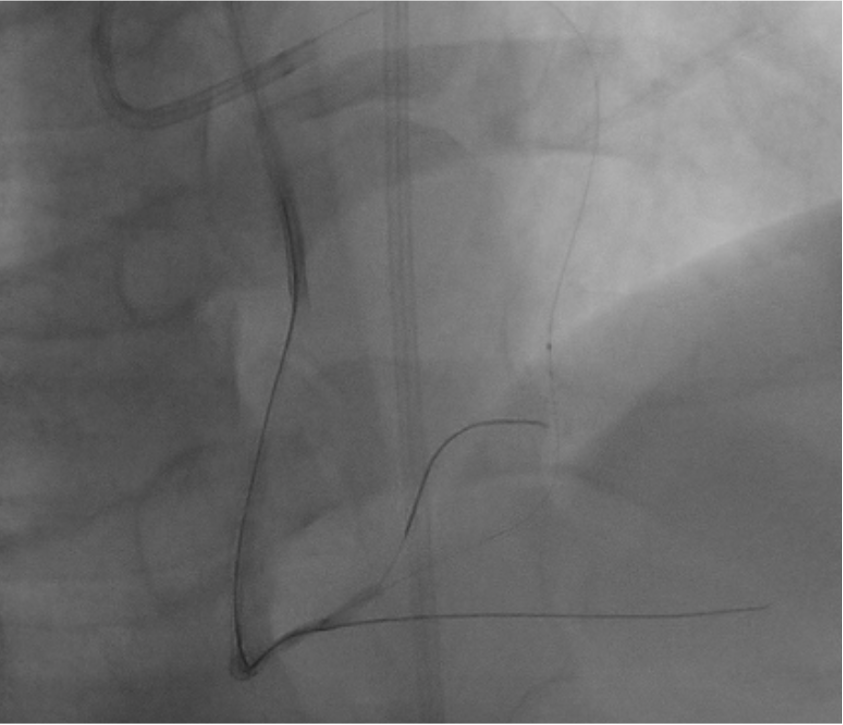
He visited our hospital for a second opinion. Coronary angiography revealed RCA total occlusion with LAD collateral. PCI was arranged and IVUS revealed the previous RCA stent deployed at the distal RCA was in the false lumen. Initially, we applied an antegrade approach, using XTA wire advancing to dRCA and Fielder FC wire advancing to the PL branch. IVUS revealed the Fielder FC in the false lumen. We finally applied a retrograde approach from LAD septal branch with Sion wire with Finecross microcatheter support to the PL branch, from true to false lumen and then advancing to mRCA into the true lumen. We shifted to RG3 wire, completing the externalization, and then antegradely advanced Fielder FC wire to distal PL. A DES was deployed at the previous distal stent edge into the PL branch, extending the stent in the false lumen into the true lumen. Another DES and a DEB were used at middle to distal RCA for the in-stent restenosis. Finally, we get a good flow and both of the PL and PDA branches were preserved.

Case Summary
We shared a case of unusual etiology of stent total occlusion due to previous stent deployment at false lumen. In CTO intervention, dual injection to check the distal wire position is important. In addition, using IVUS to check the stent was in the true lumen is essential. Antegrade, retrograde, dissection and re-entry, and other strategies can work together to help us to deal with the problem only when we figure out the lesion and the wire position clearly. Choosing and changing strategy immediately and appropriately in CTO intervention can make the procedure smoothly.