
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-053
Challenging Case of Left Main Bifurcation
By Hitendra M Bhagwatkar
Presenter
Hitendra M Bhagwatkar
Authors
Hitendra M Bhagwatkar1
Affiliation
NKPSIMS & RC, Lata Mangeshkar Hospital, Nagpur, India1,
View Study Report
TCTAP C-053
CORONARY - Bifurcation/Left Main Diseases and Intervention
Challenging Case of Left Main Bifurcation
Hitendra M Bhagwatkar1
NKPSIMS & RC, Lata Mangeshkar Hospital, Nagpur, India1,
Clinical Information
Patient initials or Identifier Number
NV
Relevant Clinical History and Physical Exam
56 year old male presented with chest pain of moderate intensity.
Relevant Test Results Prior to Catheterization
ECG showing Evolved AWMI , echo showing RWMA+(Anterior wall Akinetic with Preserved Thickness), Severe LV Dysfunction(EF-30%),
Relevant Catheterization Findings
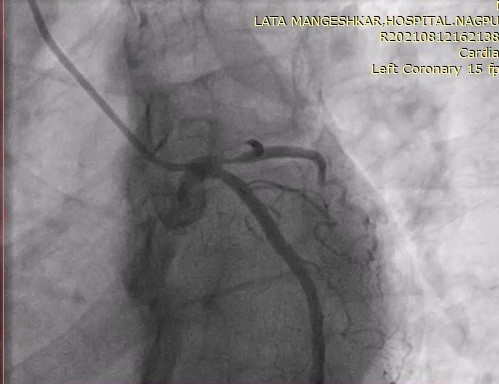
CAG – Showed LM –LAD , LCX Bifurcationlesion

Interventional Management
Procedural Step
LM was engaged with 6F 3.5 EBU guiding catheter which showed ostial LAD occluded 100 % and ostial Ramus 90% .
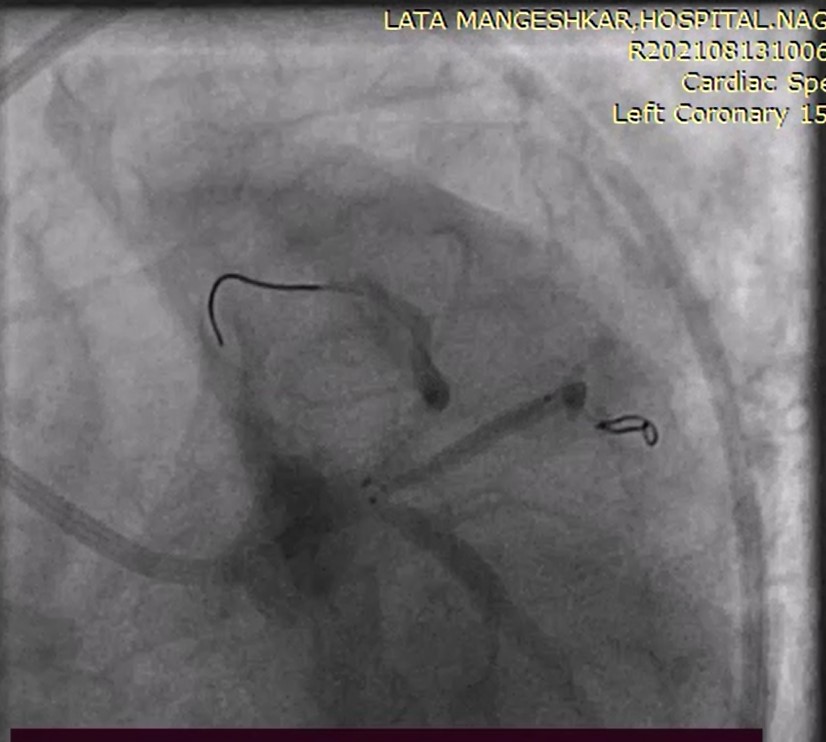
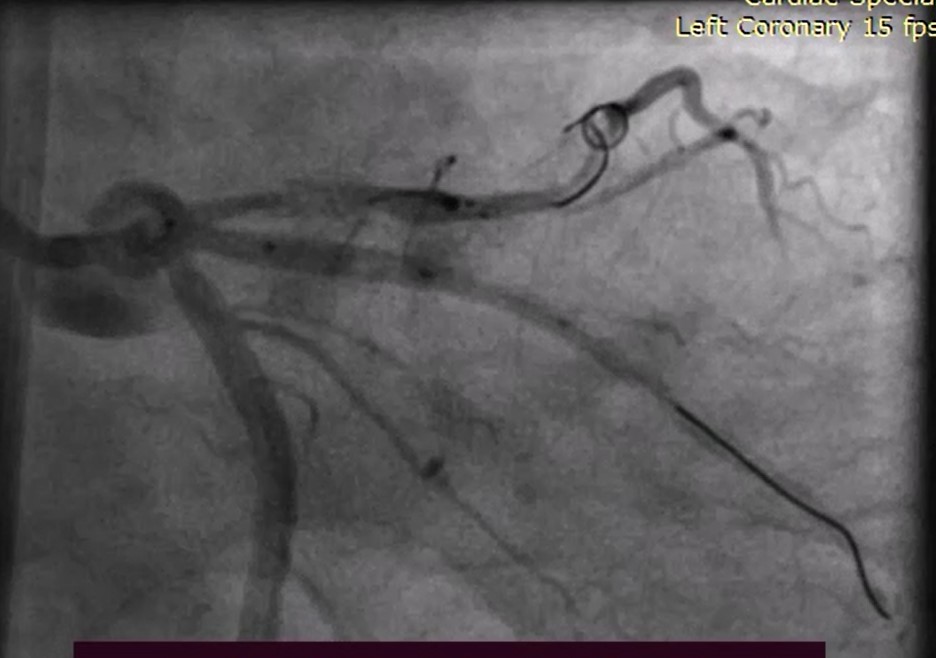
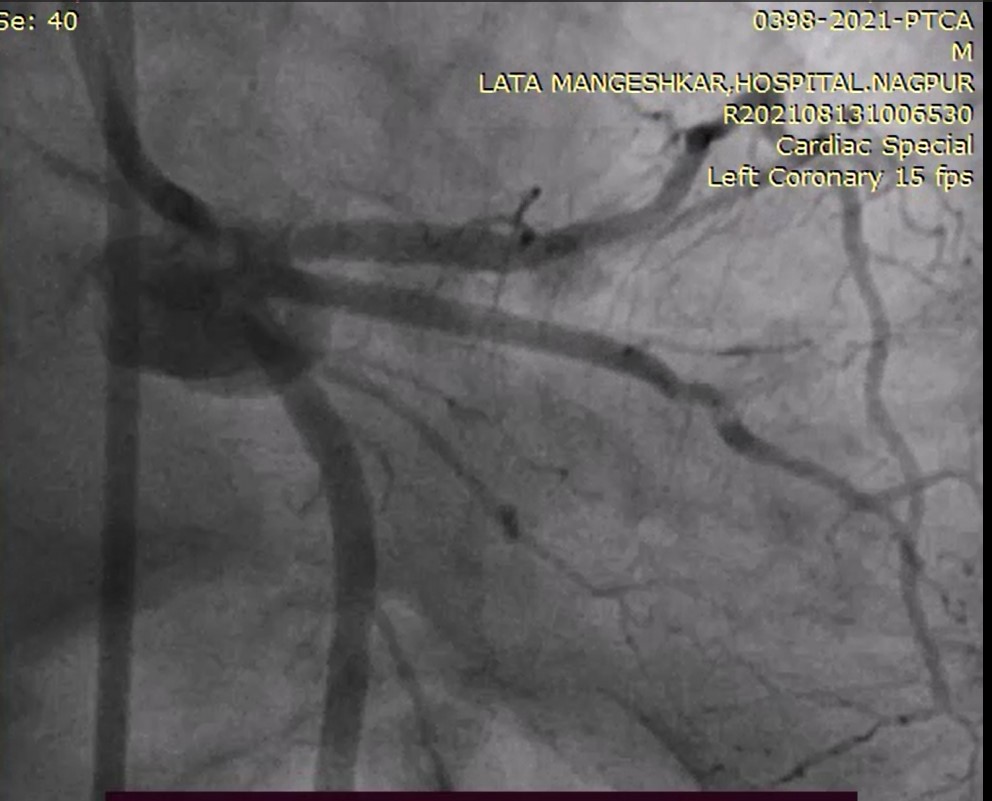
Two Runthrogh NS Guidewire crossed through LAD and Ramus across the lesion .After pre dilatation with 2.0x10 NC balloon TIMI 3 flow was achieved 3.0x24 mm DES was placed positioned across the Ramus artery and 2.5x15 NC balloon position across ostio proximal LAD and stent was dilated .while removing ramus stent balloon whole assembly including both GW and balloon came out and then we again recross Ramus stent and LAD lesion through two Run Through wires .and Pre dilated the ostio proximal LAD with 2.0X10 NC balloon to make way to stent to cross over .3.5x20mm DES was position at ostioproximal artery and 2.5x15 balloon across ostio proximal Ramus then stent was implanted and keeping the balloon into the LAD stent Ramus ostioproximal balloon was post dilated then both balloon removed and check shot taken .TIMI 3 flow achieved without pinching of Side branch
Two Runthrogh NS Guidewire crossed through LAD and Ramus across the lesion .After pre dilatation with 2.0x10 NC balloon TIMI 3 flow was achieved 3.0x24 mm DES was placed positioned across the Ramus artery and 2.5x15 NC balloon position across ostio proximal LAD and stent was dilated .while removing ramus stent balloon whole assembly including both GW and balloon came out and then we again recross Ramus stent and LAD lesion through two Run Through wires .and Pre dilated the ostio proximal LAD with 2.0X10 NC balloon to make way to stent to cross over .3.5x20mm DES was position at ostioproximal artery and 2.5x15 balloon across ostio proximal Ramus then stent was implanted and keeping the balloon into the LAD stent Ramus ostioproximal balloon was post dilated then both balloon removed and check shot taken .TIMI 3 flow achieved without pinching of Side branch
Case Summary
Femoral root should be preferred.NY York workhorse wire should be used for crossing and recrossing lesion and adequate pre dilatation should be done side branch balloon should be retained while stent implantation