
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-114
A Never Before Seen Complication of Transfemoral Angioplasty
By Ankur Gupta
Presenter
Ankur Gupta
Authors
Ankur Gupta1
Affiliation
PGIMER Chandigarh, India1,
View Study Report
TCTAP C-114
CORONARY - Complications (Coronary)
A Never Before Seen Complication of Transfemoral Angioplasty
Ankur Gupta1
PGIMER Chandigarh, India1,
Clinical Information
Patient initials or Identifier Number
D
Relevant Clinical History and Physical Exam
A 46 years old male with previous history of coronary artery stenting to ostium left anterior descending artery (LAD) presented with angina on exertion NYHA class III for last 6 months. Physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
Echocardiography showed Normal LVEF.
Relevant Catheterization Findings
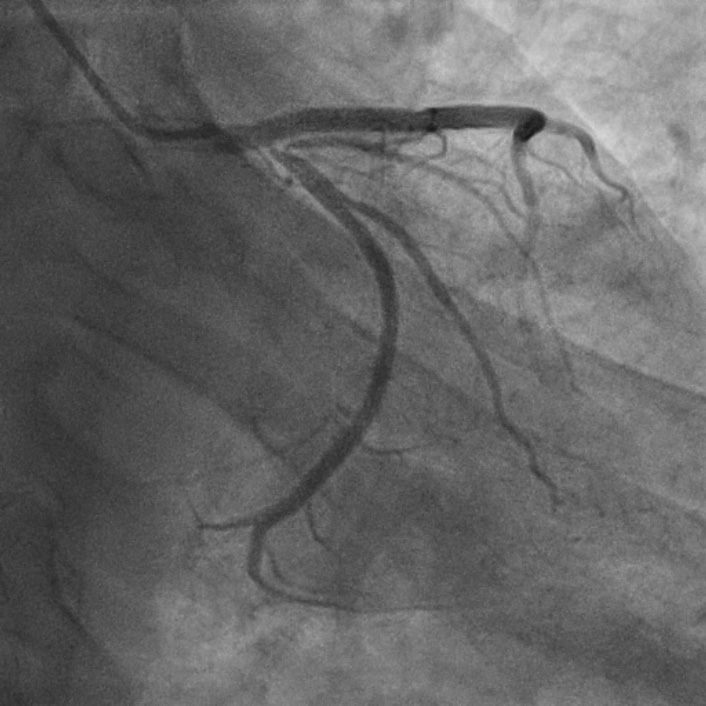
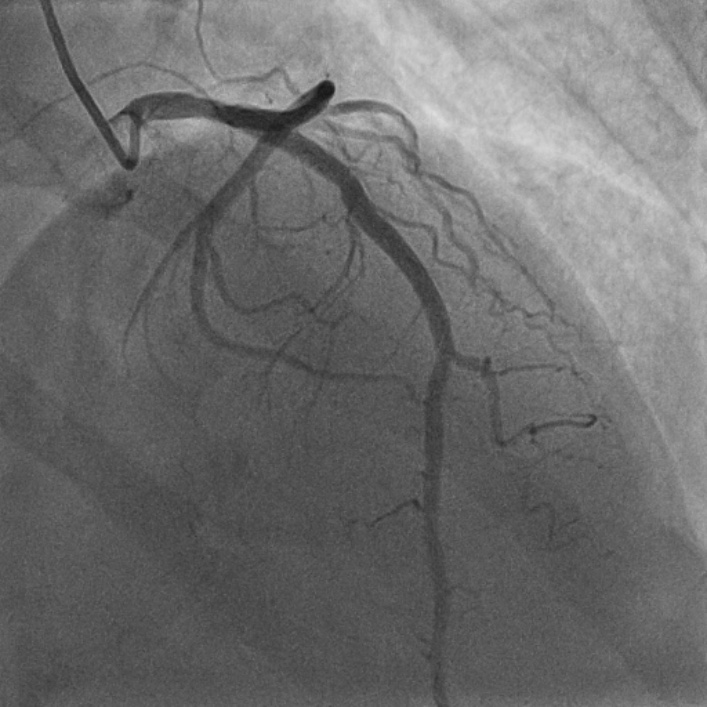
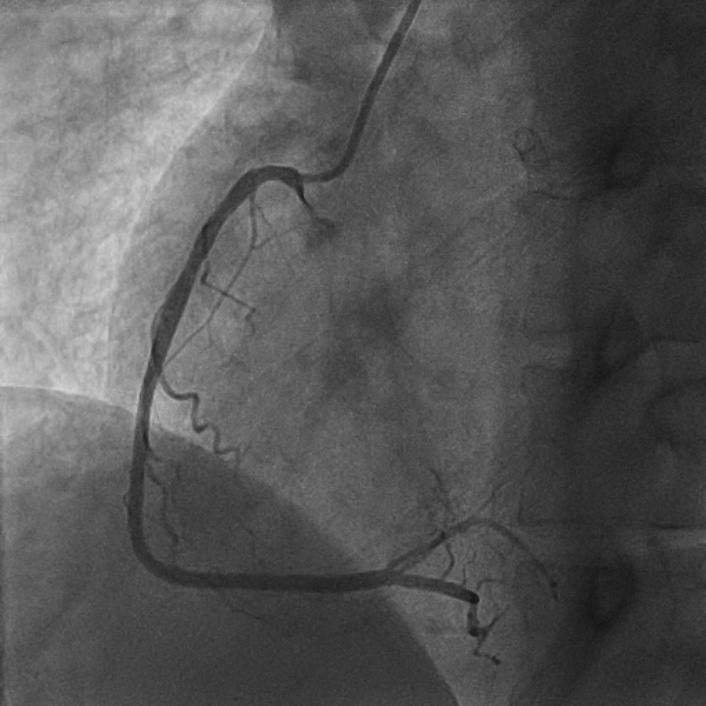
Present coronary angiogram showed left circumflex artery (LCx) ostium 90 % stenosis (Figure 1), patent stent in LAD (Figure 2) and insignificant disease in right coronary artery (Figure 3).
Interventional Management
Procedural Step
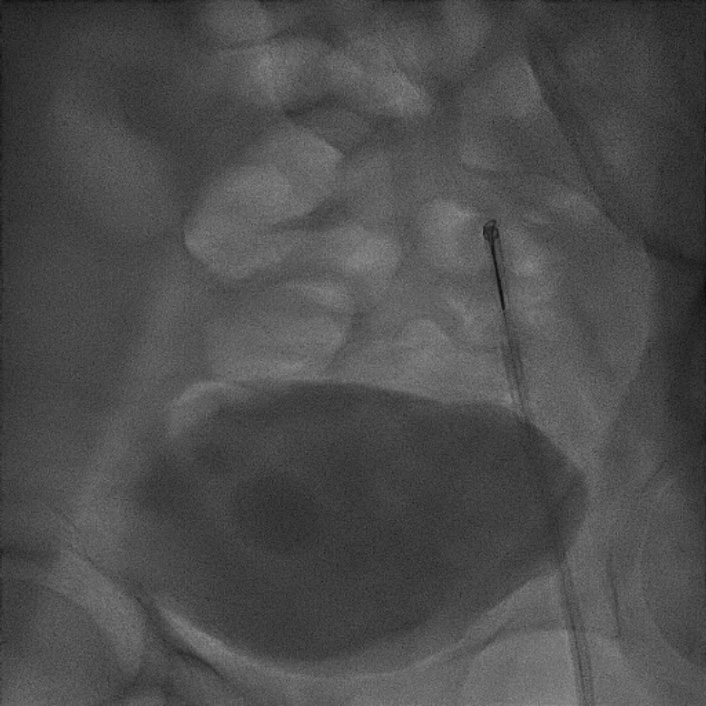
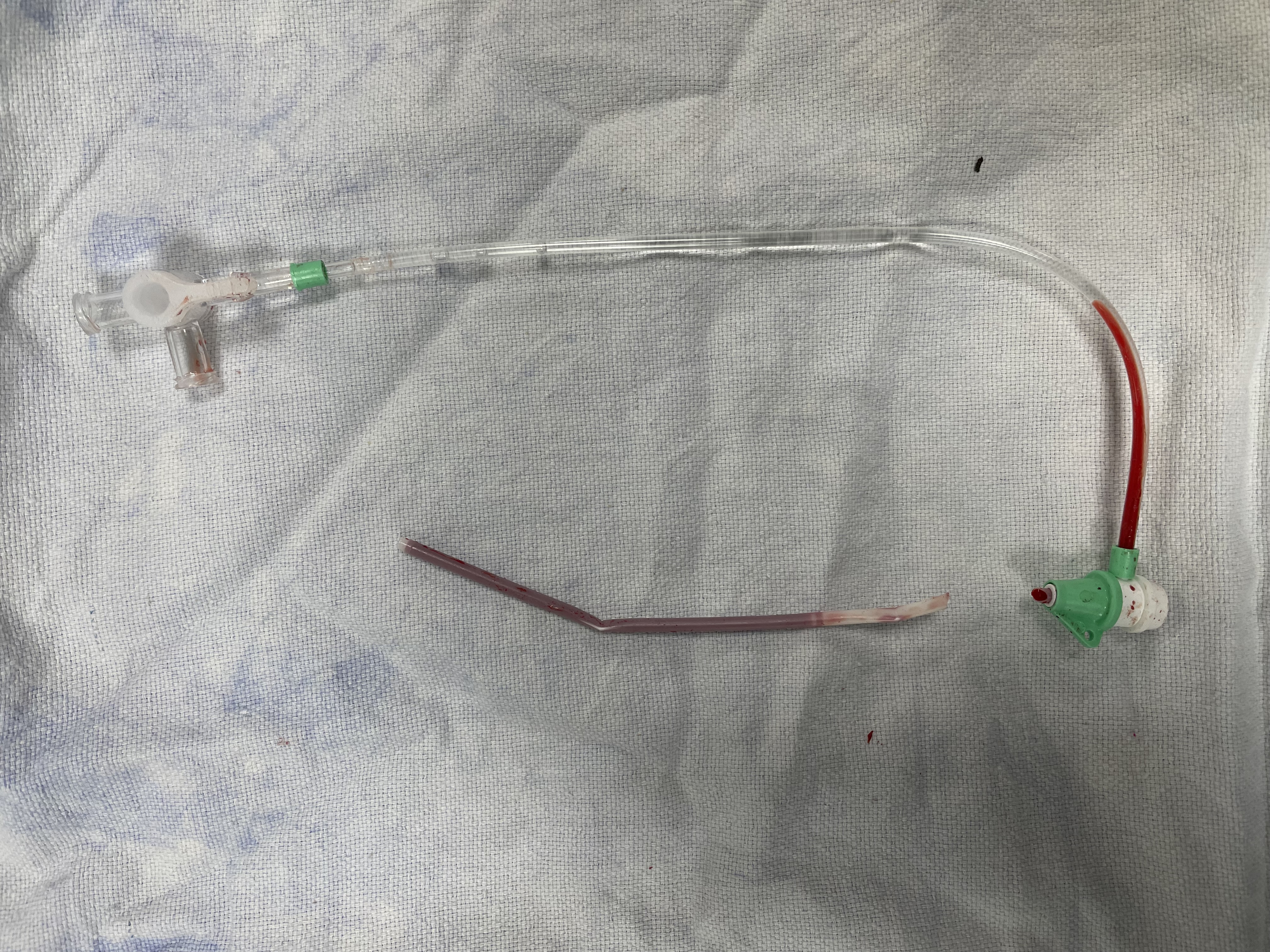
After consent patient underwent coronary artery stenting to ostium LCx using “V” technique and final kissing balloon (Figure 6). After completing the coronary stenting uneventfully, femoral angiogram was taken which showed the puncture site at the bifurcation of the common femoral artery, so perclose use was deferred. With the aim for manual compression, the femoral sheath was sutured to the skin, however, instead of cutting the suture, the sheath hub, containing the valve, was cut by the blade. Now, one end of the sheath was in the right external iliac artery and the other in the subcutaneous tissue, leading to continuous arterial bleed. Because of the active bleed, the distal end of the sheath in the subcutaneous tissue could not be visualised and no amount of manual pressure could stop the bleed. The vascular surgeon was requested to come and open up the femoral artery to manually retrieve the sheath. In the meanwhile, as the patient was bleeding profusely, the left femoral artery access was taken and after recrossing from the aortic bifurcation to the right femoral artery, the cut end of the sheath was engaged with a snare (Figure 9) and retrieved (Figure 10). Peripheral angiogram showed no damage to the femoral artery.
Case Summary
1. This was a never seen before complication of femoral angioplasty where instead of suture, the sheath hub was cut resulting in continuous arterial bleed from right femoral site and managed by snaring the cut sheath from left femoral artery route.
2. There is no surgical option in such complications as the patient might bleed to death in few minutes.
3. One should always be careful while cutting the suture tied to a sheath hub.
2. There is no surgical option in such complications as the patient might bleed to death in few minutes.
3. One should always be careful while cutting the suture tied to a sheath hub.