
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-080
The Use of Real Time IVUS-Guided PCI in Bifurcating and Ambiguous Cap of Chronic Total LAD Occlusion
By Wongwaris Aphijirawat
Presenter
Wongwaris Aphijirawat
Authors
Wongwaris Aphijirawat1
Affiliation
Queen Sirikit Naval Hospital, Thailand1,
View Study Report
TCTAP C-080
CORONARY - Chronic Total Occlusion
The Use of Real Time IVUS-Guided PCI in Bifurcating and Ambiguous Cap of Chronic Total LAD Occlusion
Wongwaris Aphijirawat1
Queen Sirikit Naval Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
AP
Relevant Clinical History and Physical Exam
Case 52 Years Old Man With a History of HT, DLP Presented With Chest Pain on Exertion for 2 Months.
Exercise Stress Test Showed Horizontal ST Depression in V3-6 at Moderate Workload.
CAG Was Performed Because Patient Still had Chest Pain Despite Maximal Medication for CAD.
PCI to LCx was done with DES x I, Staged PCI to CTO LAD was Planned for Complete Revascularization.
Exercise Stress Test Showed Horizontal ST Depression in V3-6 at Moderate Workload.
CAG Was Performed Because Patient Still had Chest Pain Despite Maximal Medication for CAD.
PCI to LCx was done with DES x I, Staged PCI to CTO LAD was Planned for Complete Revascularization.
Relevant Test Results Prior to Catheterization
CBC : WBC 8,000 Hb 14 g/dL Hct 42% platelet 300,000
HsTroponin : 8BUN 12 Cr 0.9 mg/dL GFR 82 LDL-c 124 mg/dL
HsTroponin : 8BUN 12 Cr 0.9 mg/dL GFR 82 LDL-c 124 mg/dL
Relevant Catheterization Findings
Left Main : Non-significant Stenosis.
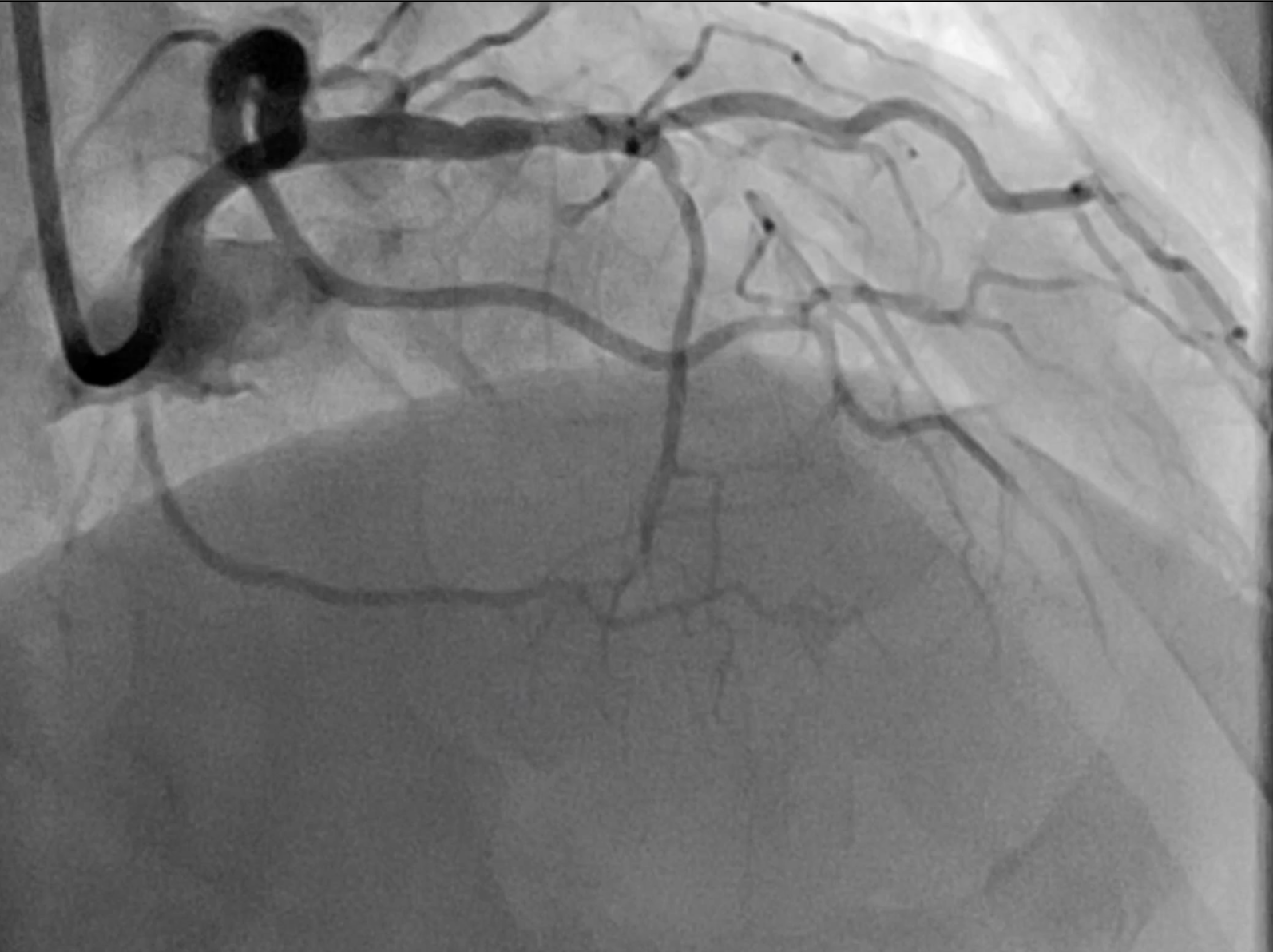
LAD : 50% Stenosis at Proximal Segment, 100% CTO at Mid LAD at Level of Bifurcation DG and Septal Branch, Ambiguous Cap, CTO Length About 15 MM and Receive Collateral Flow From Lcx and RCA.
Lcx : Patent mid Lcx Stent.
RCA : Non-significant Stenosis.


LAD : 50% Stenosis at Proximal Segment, 100% CTO at Mid LAD at Level of Bifurcation DG and Septal Branch, Ambiguous Cap, CTO Length About 15 MM and Receive Collateral Flow From Lcx and RCA.
Lcx : Patent mid Lcx Stent.
RCA : Non-significant Stenosis.
Interventional Management
Procedural Step
Strategy Was Planned, Used 7F Guiding Catheter , Antegrade Wiring First and Then Retrograde if Failed Antegrade Wiring, Dual Lumen Microcatheter.
We Placed Workhorse Wire in Septal Branch and Using the Crusade Type R Catheter, However, Runthrough, Fielder XT Wire Couldn’t Pass the Lesion Due to Wire Was Always Slipped Into DG1 and Septal Branch. So, at This Time, We Faced a Difficulty Wiring Problem From Ambiguous Cap at the Bifurcation of DG1 and Septal Branch.
Wiring Was Unsuccessful After 30 Minutes of Time.
Then We Carefully Relooked the Angiogram for the Way of Retrograde Approach but We Saw at Very Tiny Cap at Mid LAD.
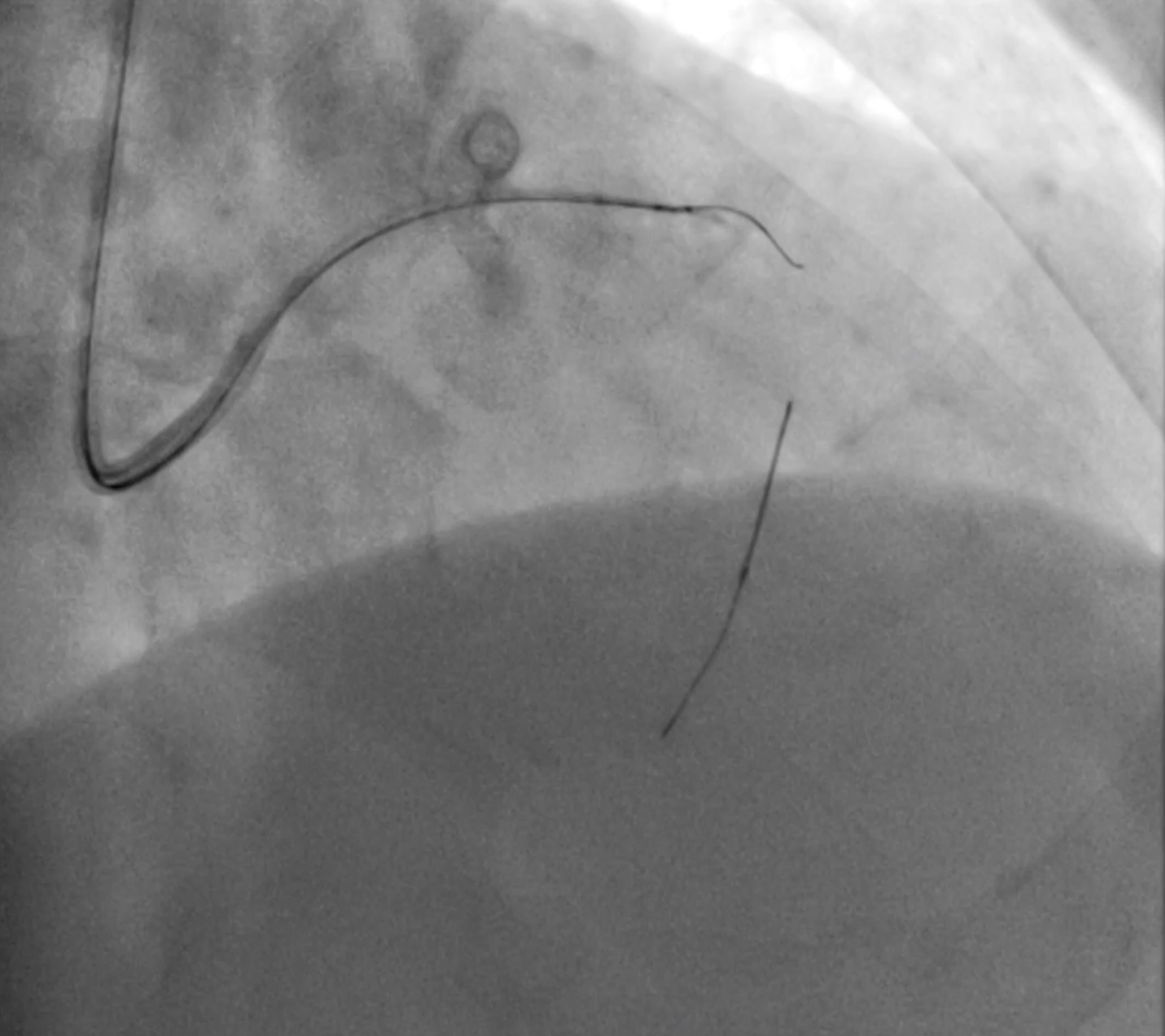
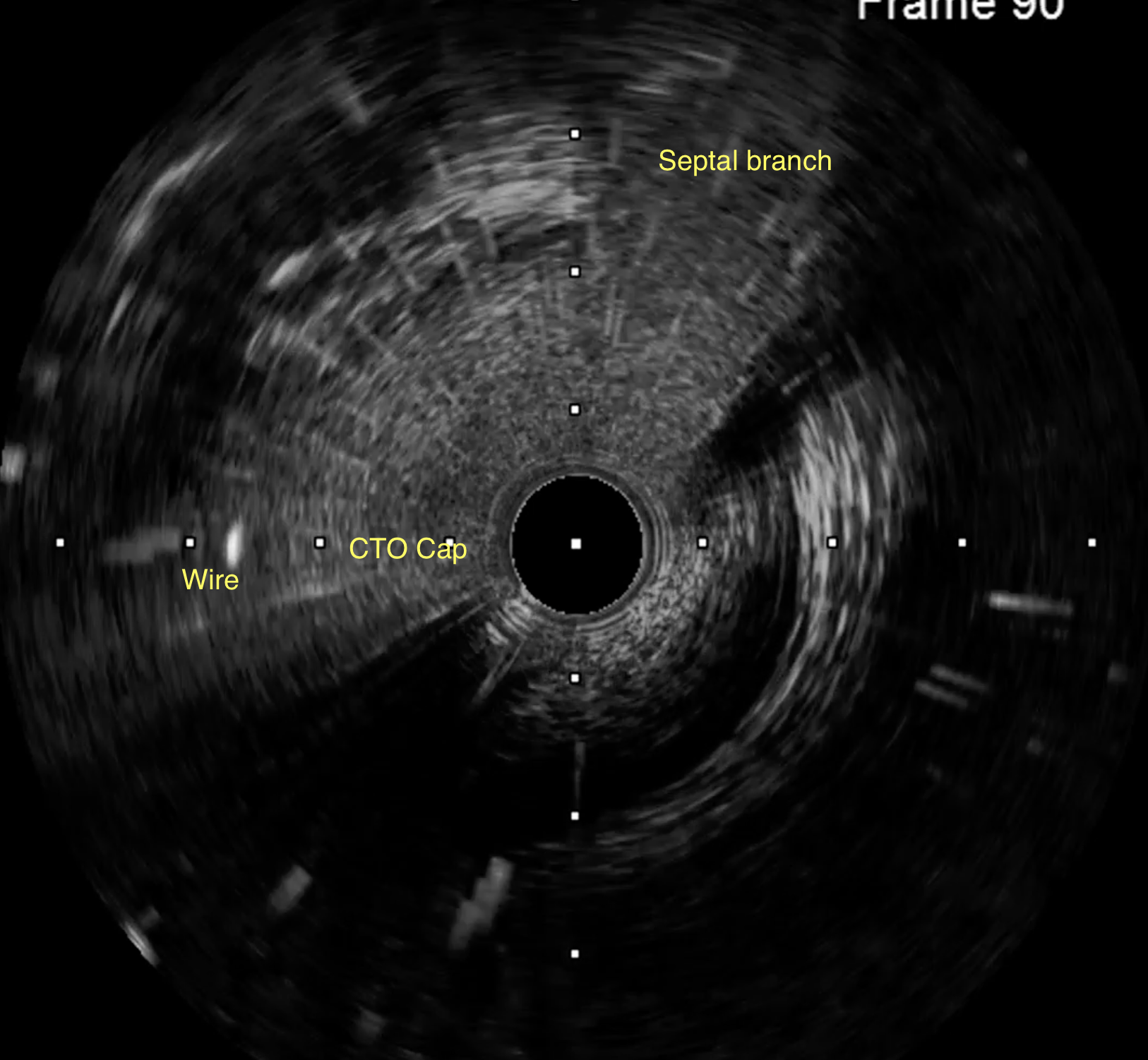
So, We Use the IVUS to Assess the Antegrade Entry Cap of The LAD.
IVUS Showed a Small Entry Cap at LAD and We Use the Real-Time IVUS-Guided Wiring by Fielder XT Wire. The Wire was Able to Entry The LAD Cap,Unfortunately, Fielder XT Couldn’t Pass the CTO Lesion. Gaia First Was Able to Cross the CTO Lesion Into Distal LAD Which Confirmed by Collateral Flow From Lcx.
The 1.5 MM Balloon Could Not Pass the Lesion at Mid LAD. We Use the Guide Extension Catheter and Leopard-Claw Technique to Pass the 1.0 X 6 MM Ikazuchi Balloon to the Lesion.
1.5 X 10 MM Ryurei Balloon, 2.0 X 15 MM Sprinter Legend Balloon Were Predilated at the Lesion, Repeated IVUS Confirmed the Wire in the True Lumen.
3.0 X 38 MM ZES Stent Was Deployed at the Lesion and 3.5 X 15 MM NC Balloon Was Postdilated in the Stent.
Final Angiogram Showed Good TIMI III Flow Without Complication.

We Placed Workhorse Wire in Septal Branch and Using the Crusade Type R Catheter, However, Runthrough, Fielder XT Wire Couldn’t Pass the Lesion Due to Wire Was Always Slipped Into DG1 and Septal Branch. So, at This Time, We Faced a Difficulty Wiring Problem From Ambiguous Cap at the Bifurcation of DG1 and Septal Branch.
Wiring Was Unsuccessful After 30 Minutes of Time.
Then We Carefully Relooked the Angiogram for the Way of Retrograde Approach but We Saw at Very Tiny Cap at Mid LAD.
So, We Use the IVUS to Assess the Antegrade Entry Cap of The LAD.
IVUS Showed a Small Entry Cap at LAD and We Use the Real-Time IVUS-Guided Wiring by Fielder XT Wire. The Wire was Able to Entry The LAD Cap,Unfortunately, Fielder XT Couldn’t Pass the CTO Lesion. Gaia First Was Able to Cross the CTO Lesion Into Distal LAD Which Confirmed by Collateral Flow From Lcx.
The 1.5 MM Balloon Could Not Pass the Lesion at Mid LAD. We Use the Guide Extension Catheter and Leopard-Claw Technique to Pass the 1.0 X 6 MM Ikazuchi Balloon to the Lesion.
1.5 X 10 MM Ryurei Balloon, 2.0 X 15 MM Sprinter Legend Balloon Were Predilated at the Lesion, Repeated IVUS Confirmed the Wire in the True Lumen.
3.0 X 38 MM ZES Stent Was Deployed at the Lesion and 3.5 X 15 MM NC Balloon Was Postdilated in the Stent.
Final Angiogram Showed Good TIMI III Flow Without Complication.
Case Summary
Carefully Examine the Angiogram Before PCI Is Important for Strategy Selection.
When the Procedure Was Not Successful as Planning, Step Backward Before Go on Further Step.
The Real-Time IVUS Guided Wiring Could Show You a Hidden Way That We Couldn’t See at the Angiogram and Make Sure You Enter the True Lumen.
When the Procedure Was Not Successful as Planning, Step Backward Before Go on Further Step.
The Real-Time IVUS Guided Wiring Could Show You a Hidden Way That We Couldn’t See at the Angiogram and Make Sure You Enter the True Lumen.