
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-070
Another Way Out!
By Chang-Yi Lin
Presenter
Chang-Yi Lin
Authors
Chang-Yi Lin1
Affiliation
Mackay Memorial Hospital, Taiwan1,
View Study Report
TCTAP C-070
CORONARY - Chronic Total Occlusion
Another Way Out!
Chang-Yi Lin1
Mackay Memorial Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
53887656
Relevant Clinical History and Physical Exam
A 57 years old male patient had underlying disease of hypertension and hyperlipidemia under medication. He is also a current cigarette smoker.He had been to our emergent department due to shortness of breath. He also had symptoms and signs of heart failure, including dyspnea on exertion and bilateral ankle edema. Physical examination revealed S3 murmur and bilateral legs edema.
Relevant Test Results Prior to Catheterization
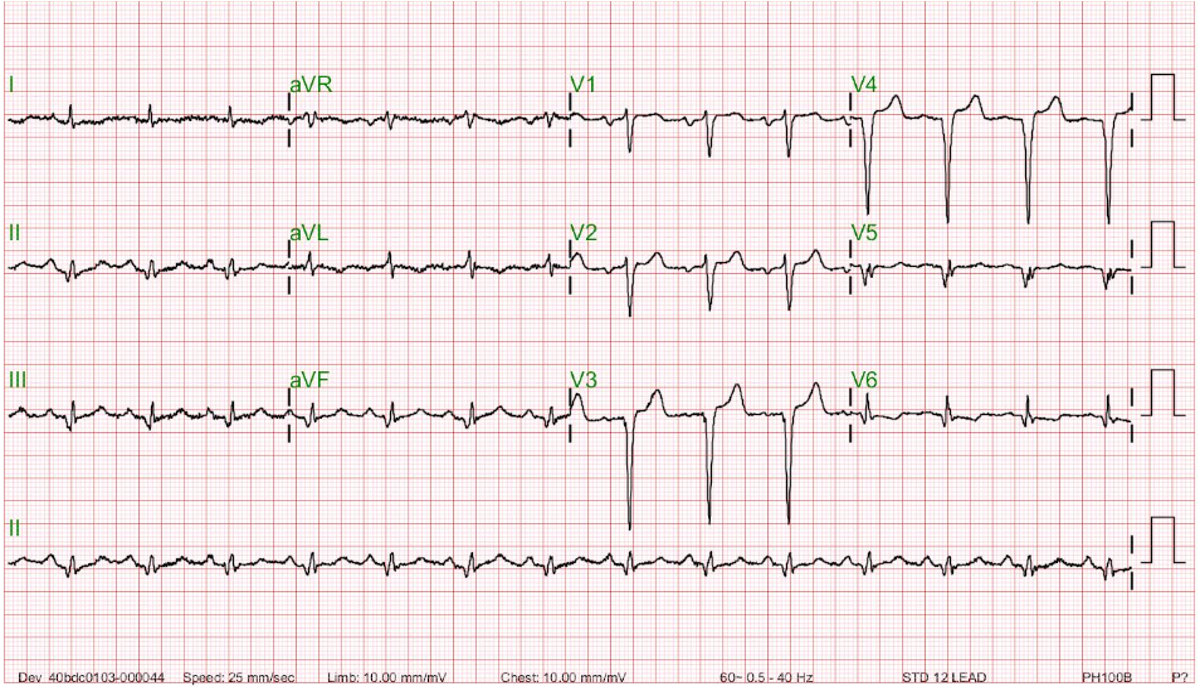
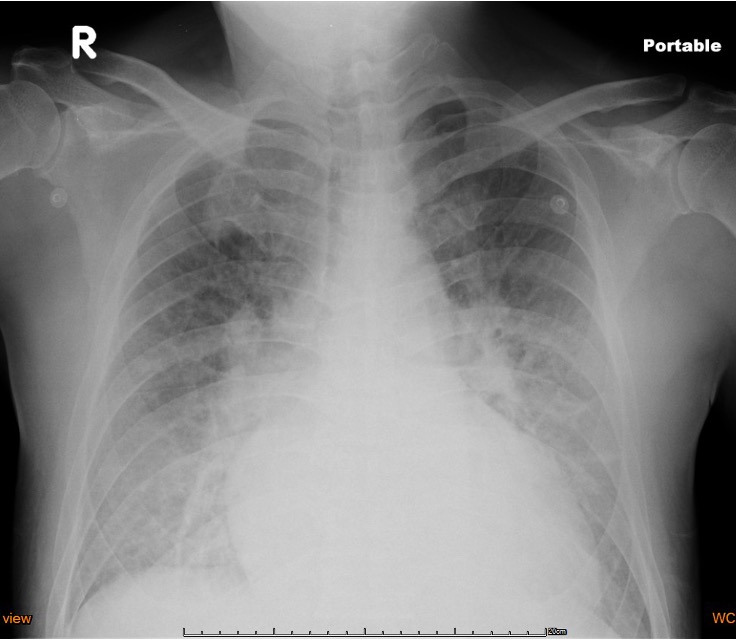
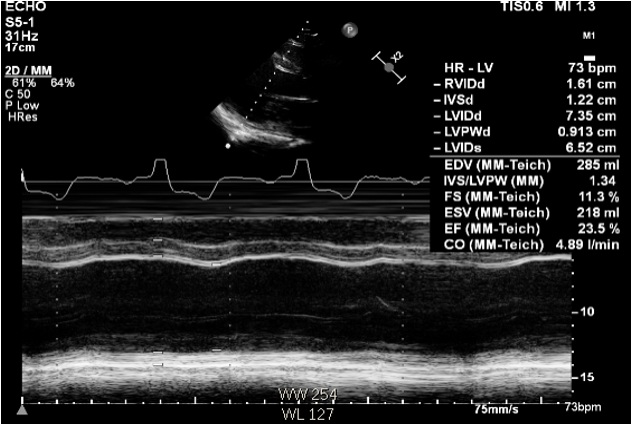
ECG: old anterior wall MI, Sinus rhythmCXR: Pulmonary edemaCK: 115, CKMB: 1.78, Troponin-I 0.033, NT-proBNP: 2470 (50-75 y/o: 900 pg/mL), Cr :1.2 (eGFR: 62.4)Heart echo: LAE, LVE, LVEF 23.5%, moderate MR
Relevant Catheterization Findings
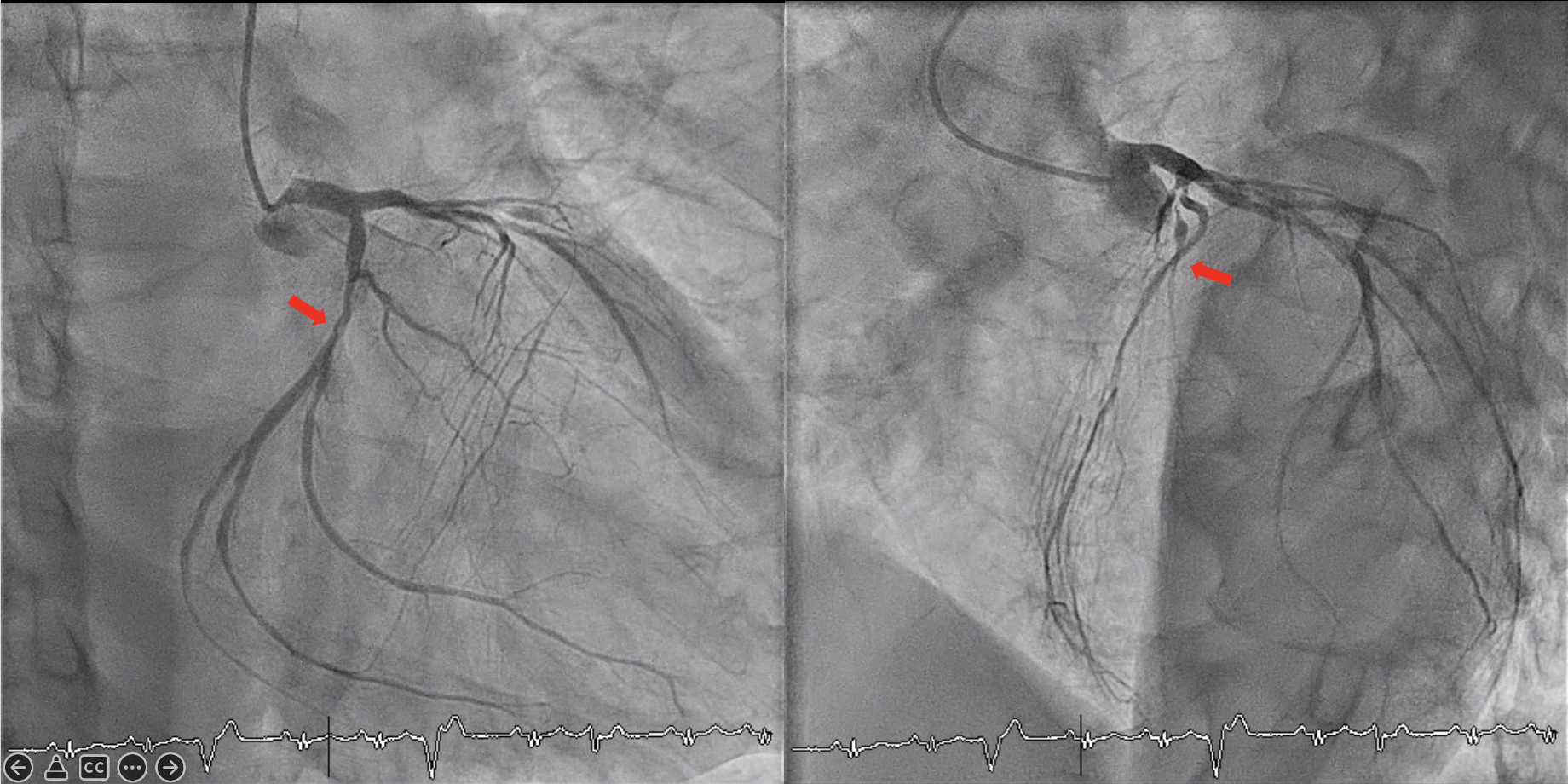
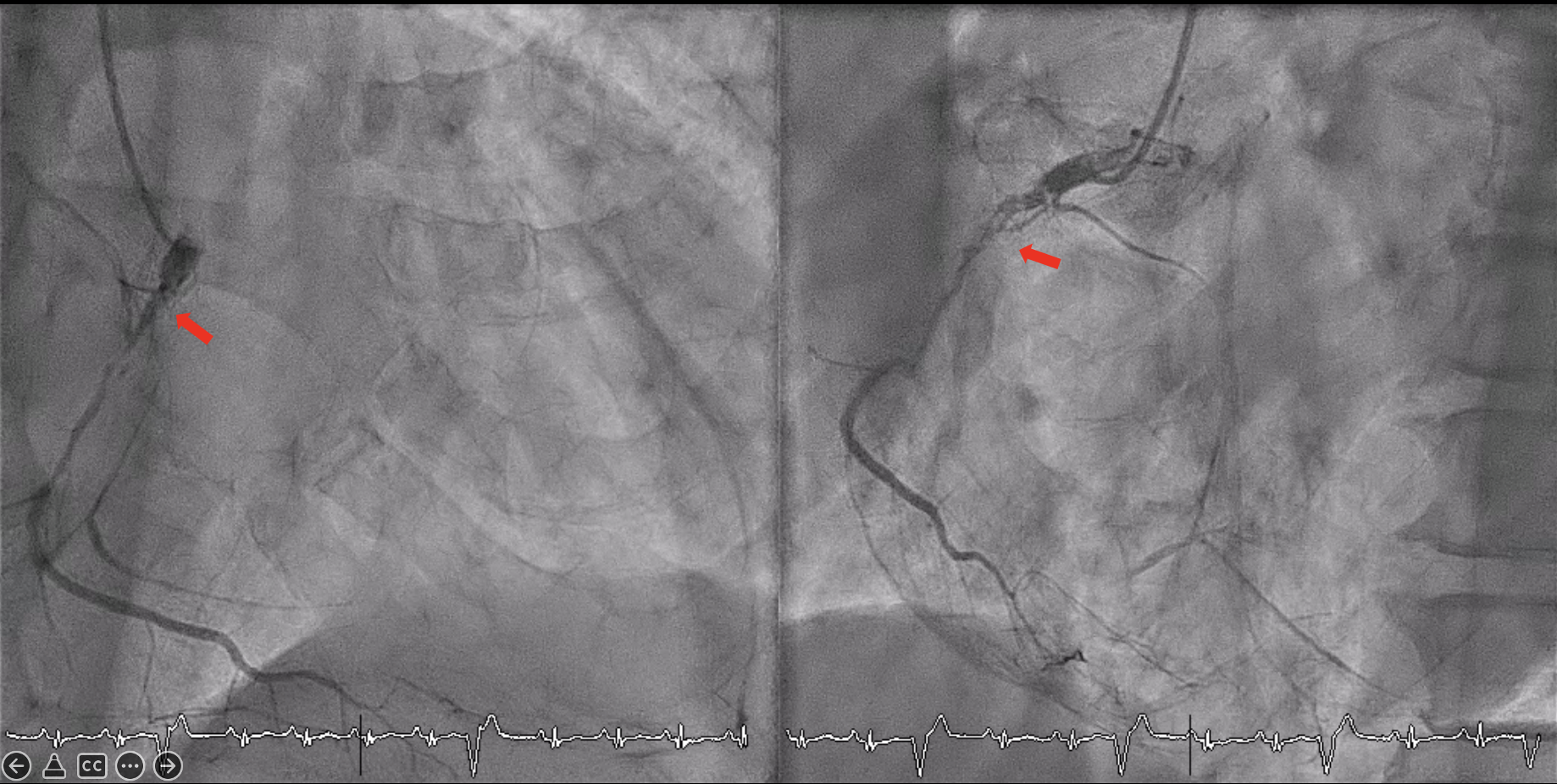
LAD-p: CTO with stumpless ostium at main trunkRCA-p: CTOLCX: 30% stenosis
Interventional Management
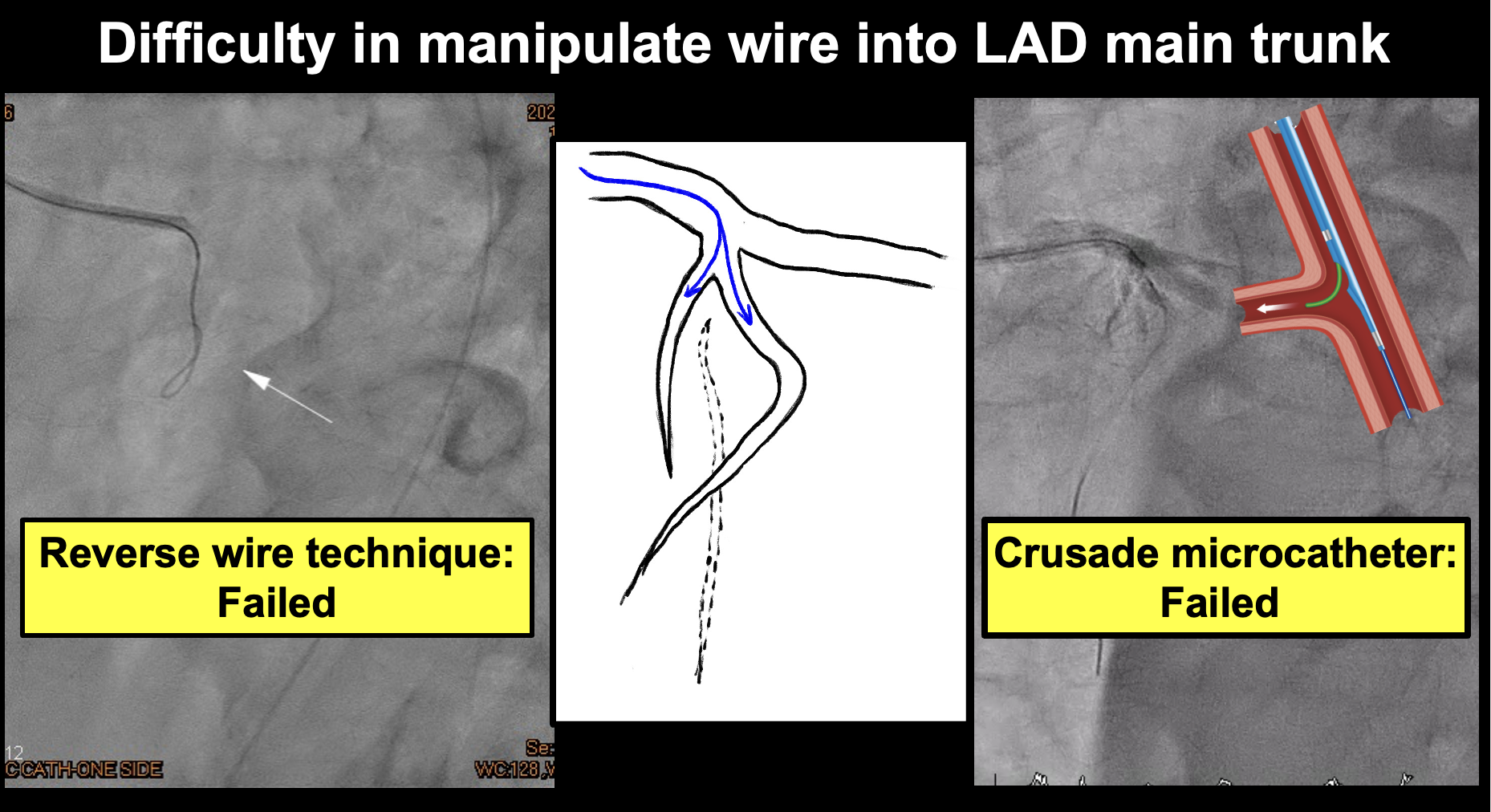
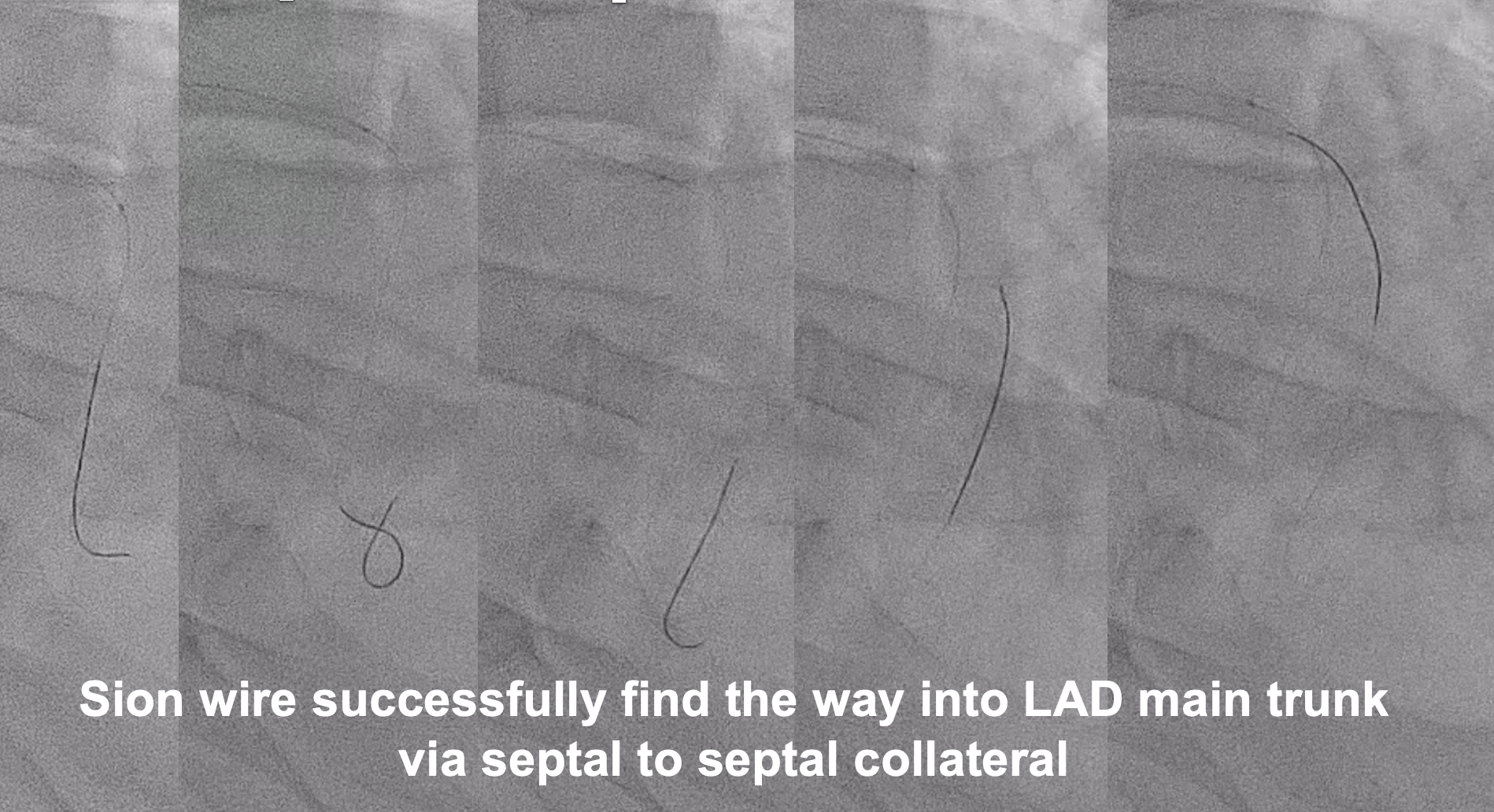
Procedural Step
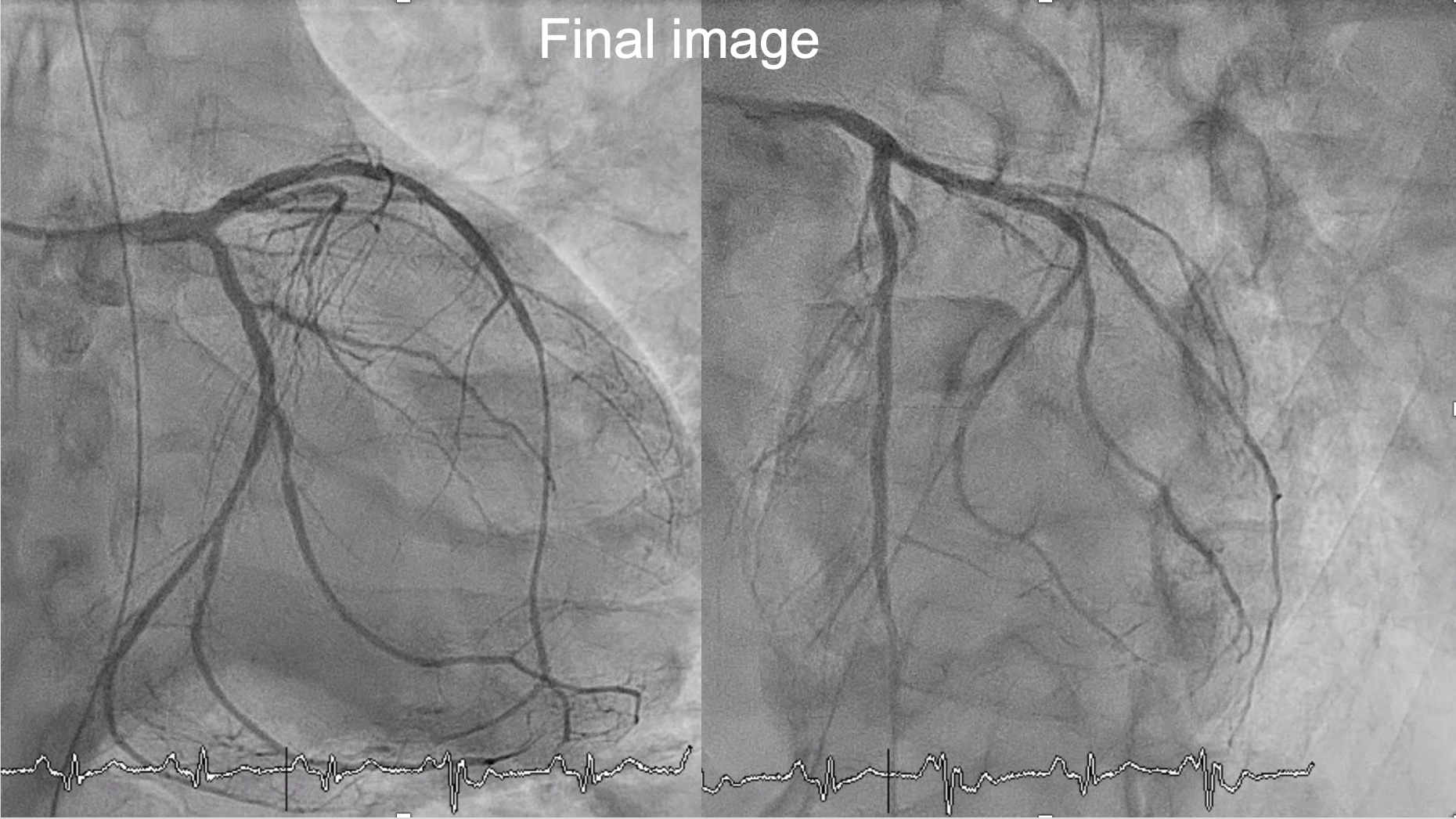
Target: p-LAD CTO. We choose antegrade approach first.There were extreme ostial narrowing at main trunk and we've tried many ways to entering the lesion, including upgrade wire from sion black, XTA to Gaia 1st, perform reversed wire technique and we even facilitated by double lumen catheter, Crusade. However, it's really difficult to wiring into main trunk of LAD. So we tried retrograde approach and find a septal to septal collateral and finally wiring Sion-blue wire back to LAD.Successful Rendezvous technique was performed in JL Guiding and we changed wire to XTA.XTA is then manipulate to distal LAD.Sequential dilatation was done and we checked IVUS to ensure that the wire was in true lumen.Two DESyne stent was deployed in p-LAD and p-LCX (2.75 x 38 mm and 2.5 x 32 mm, respectively)IVUS was checked after stenting and showed good stent expansion and apposition.Final angiography showed TIMI 3 flow.
Case Summary
1. Identify the potential risks and stop the procedure promptly.2. When fail of one strategy, stay calm, re-analysis the the lesion and always be prepared to switch between strategies. 3. Never give up any possible route, septal collateral circulation is another way for CTO retrograde approach.