
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-063
Horrible Dissection, You Need a Second Eye!
By Osama Shoeib
Presenter
Osama Shoeib
Authors
Osama Shoeib1
Affiliation
Tanta University Hospital, Egypt1,
View Study Report
TCTAP C-063
CORONARY - Bifurcation/Left Main Diseases and Intervention
Horrible Dissection, You Need a Second Eye!
Osama Shoeib1
Tanta University Hospital, Egypt1,
Clinical Information
Patient initials or Identifier Number
MA
Relevant Clinical History and Physical Exam
Male patient 55 years old, HTN not DM with typical anginal pain, His ECG showed no significant abnormalities also his ECHO showed good LV systolic function and no wall motion abnormalities. Patient was referred for coronary angiogram.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
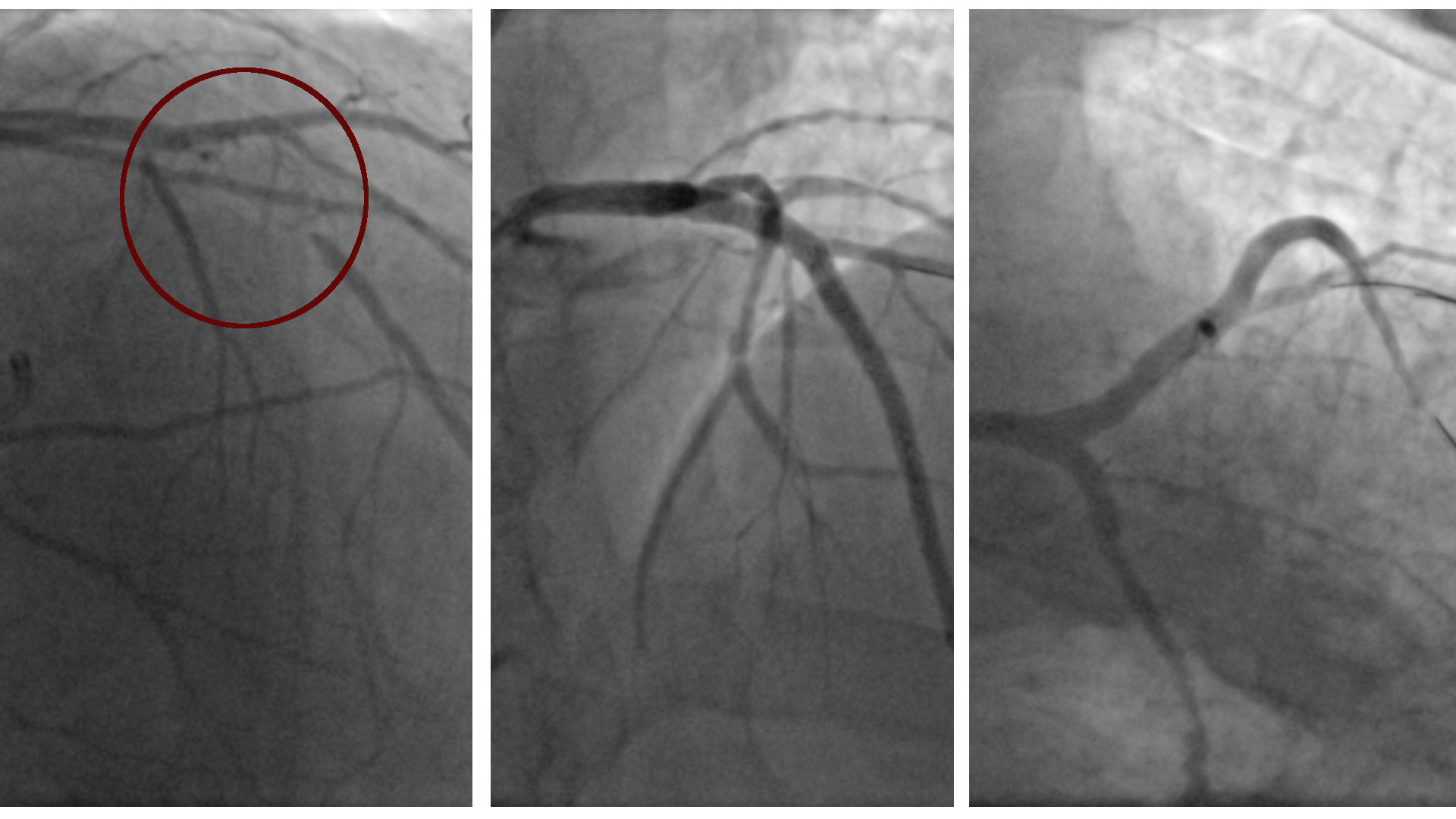
Coronary angiogram was done and showed:
•RCA: small non dominant
•CX: mid segment tight lesion
•LAD: mid segment CTO
CABG was recommended, but the patient refused!
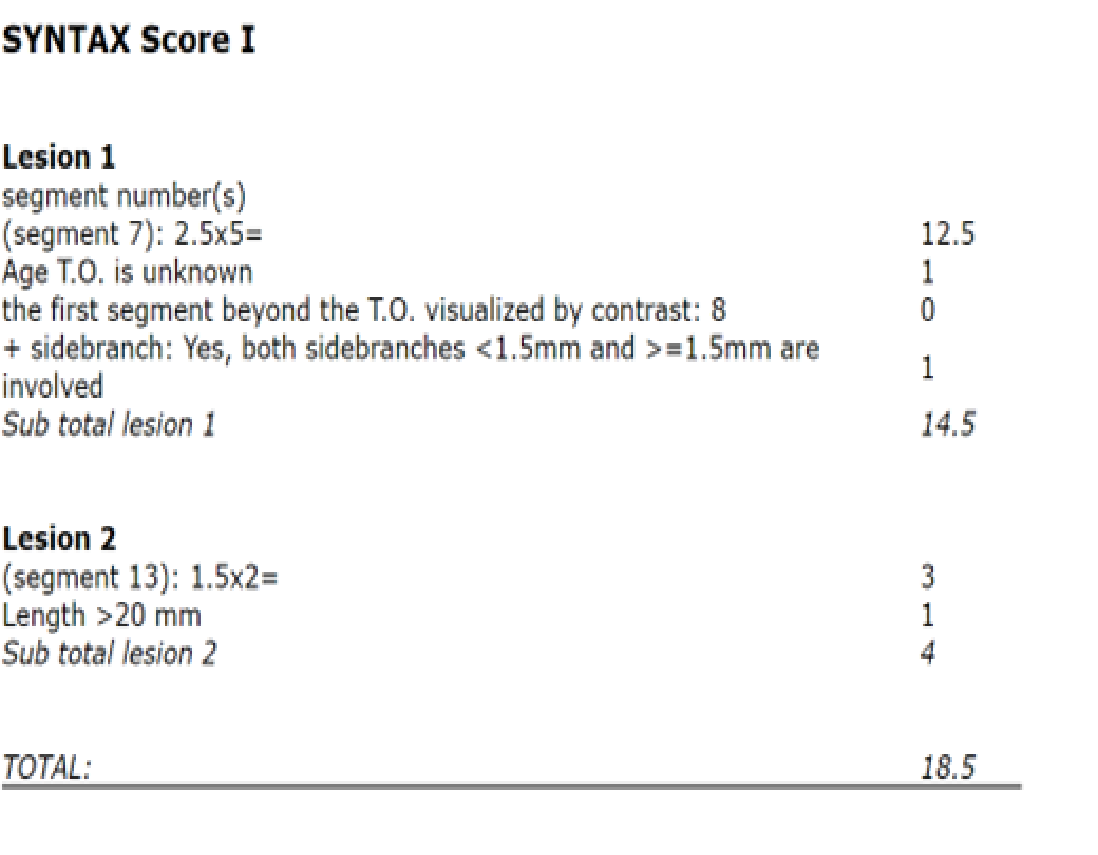
Syntax score 18.5. After a thorough discussion with the heart team and patient himself we decided to go for PCI.
Interventional Management
Procedural Step
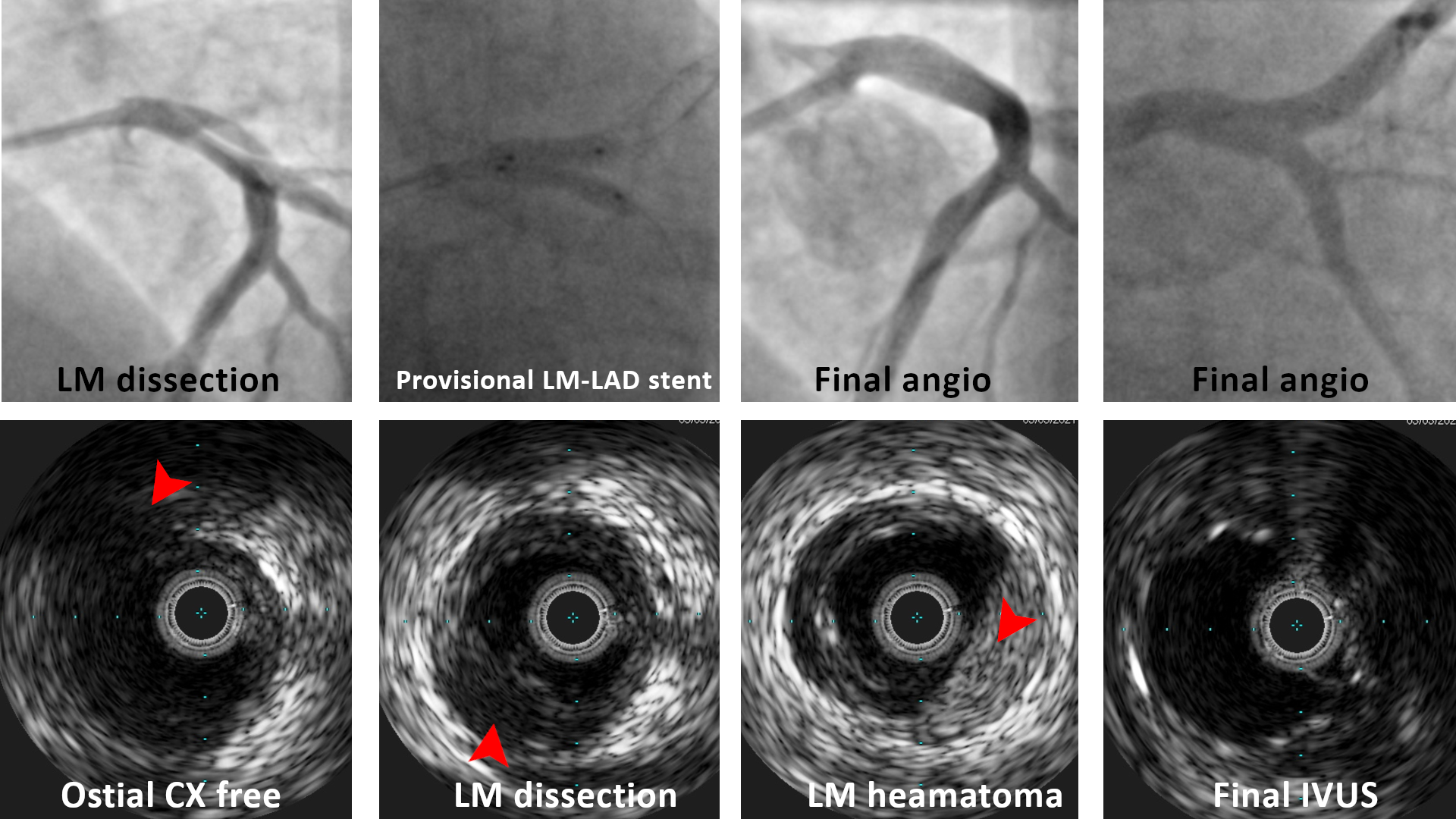
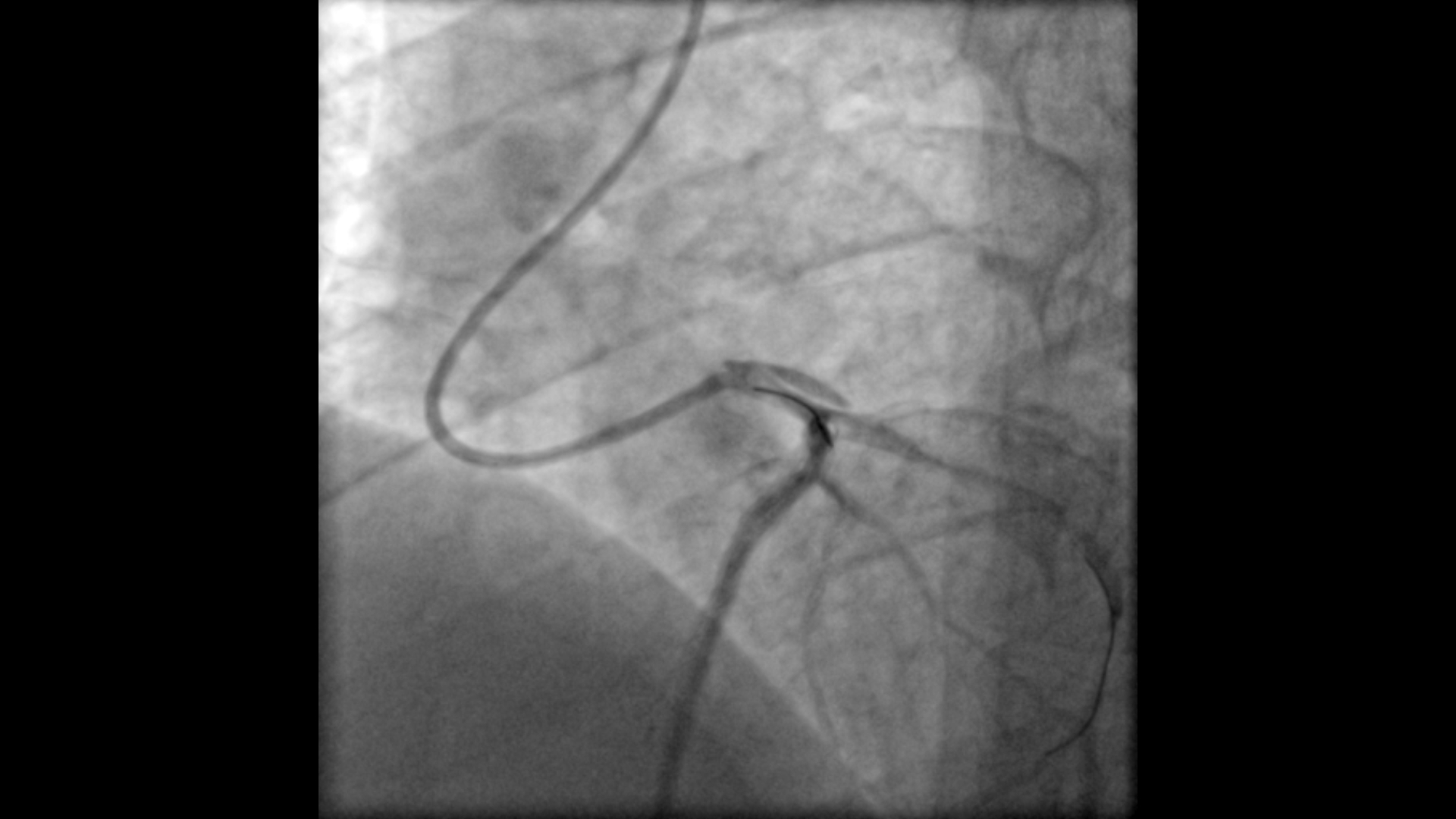
We started with the LAD CTO lesion, and we went for a bilateral radial access, with XB 3.5 6Fr to LM and A JR to RCA for retrograde injection, we adopted the antegrade wire escalation approach. The procedure went smoothly, and a GAIA II wire successfully reached distal LAD true lumen and then exchanged with a work horse wire. Two stents were deployed successfully, and the final LAD result was particularly good.Then we decided to treat the CX lesion, so another workhorse wire was advanced to distal CX, Afterwords patient developed chest pain, an angiogram showed dissection in distal LM but with sufficient flow to both LAD and CX.We were not sure if the dissection was due to the deeply engaged guiding catheter or the CX guide wire, and the doubt arises if the dissection is toward the LAD or toward the CX!So, we decided to use IVUS to understand more, and it confirms the dissection is in the LM body and the CX ostium is not affected, so we decided to stent LM-LAD to cover the dissection followed by the standard techniques of provisional stenting.Then we treated the CX lesion with another stent, after which patient developed another attack of chest pain and angiogram showed TIMI I flow in the CX and another time the IVUS come in handy and confirmed no proximal or distal edge dissection and so medical treatment in the form of IC nitrates and verapamil improved distal flow (TIMI III) and patient was discharged safely.
Case Summary
Extra backup guiding catheters are injuries so the operator should be careful regarding deep intubation and apply safety measures such as the floating wire technique if applicable to protect against deep intubation. When you suspect dissection get imaging and avoid more injections.When doing PCI with one of these guiding catheters, we recommend to always have a final caudal view to check the integrity of the LM at the end of the procedure. Rapid intervention with stenting to seal the dissection flap is a life-saving measure.