
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-100
Type III Perforation in a Vessel With Severe Calcification
By Vijin Joseph V F, Rony Mathew, Jimmy George P
Presenter
Vijin Joseph V F
Authors
Vijin Joseph V F1, Rony Mathew2, Jimmy George P1
Affiliation
Lisie Hospital, India1, Lisie Heart Institute, India2,
View Study Report
TCTAP C-100
CORONARY - Complications (Coronary)
Type III Perforation in a Vessel With Severe Calcification
Vijin Joseph V F1, Rony Mathew2, Jimmy George P1
Lisie Hospital, India1, Lisie Heart Institute, India2,
Clinical Information
Patient initials or Identifier Number
2601385
Relevant Clinical History and Physical Exam
A 87 year old female with paraparesis and a history of type 2 diabetes mellitus, systemic hypertension, peripheral vascular occlusive disease and chronic kidney disease presented with chest pain and dyspnea. she was diagnosed with acute coronary syndrome and pulmonary edema. she underwent a coronary angiogram, which showed severe calcific triple vessel disease. she was advised to undergo multivessel percutaneous transluminal coronary angioplasty. On examination her vitals were stable.
Relevant Test Results Prior to Catheterization
Her electrocardiogram showed sinus rhythm with STdepression in the anterior leads. 2D echocardiography revealed regional wallmotion abnormality with hypokinesia in the anteroseptal, apex and apical septumsegments with mild LV systolic dysfunction. Her chest x-ray showed mildpulmonary venous congestion. Her haemoglobin was 10.6 g/dL, random blood sugarwas 173 mg/dL, creatinine was 1.5 mg/dL and troponin T was 0.6 ng/ml.
Relevant Catheterization Findings
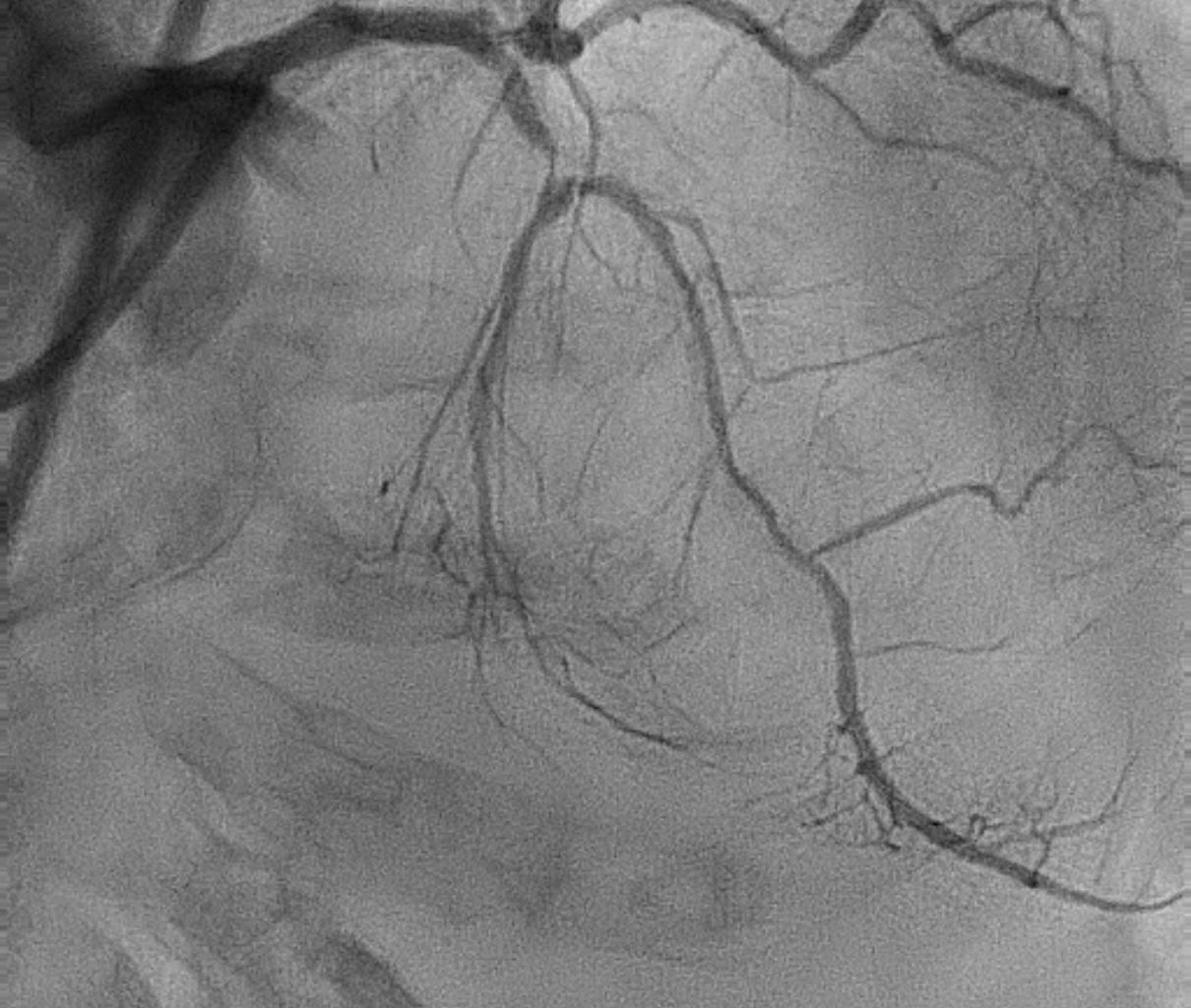
Acoronary angiogram revealed severe calcific triple vessel disease with abifurcation lesion involving the left anterior descending artery and majorseptal branch. Angiographically, there was circumferential calcium in all threevessels. She was taken up for multi vessel percutaneous transluminal coronaryangioplasty through left femoral artery. There was significant calcium withcalcific nodule in both the common iliac arteries.


Interventional Management
Procedural Step
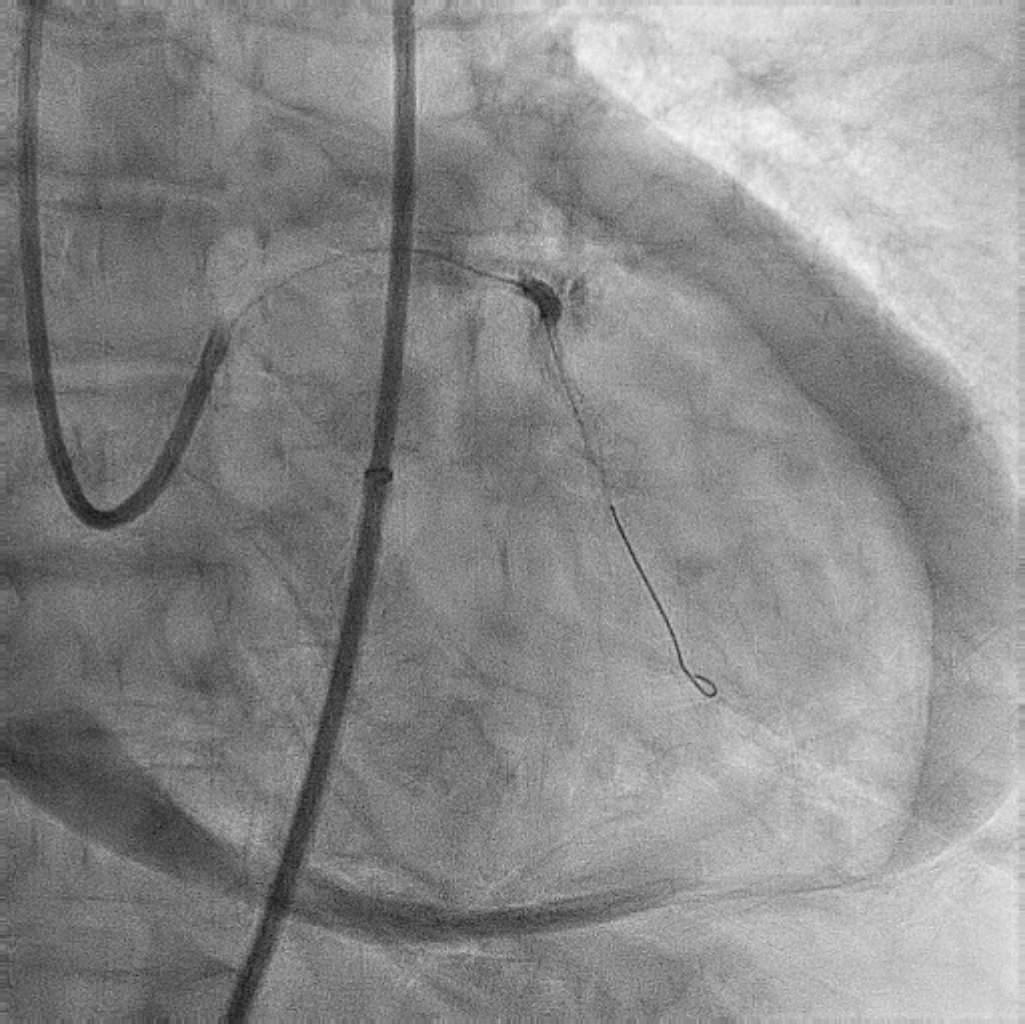
She was taken for multivessel percutaneous transluminal coronary angioplasty through the left femoral artery, where there was an 80% discrete calcified lesion in the left common iliac artery. The lesion was predilated with MUSTANG balloon (6 x40 mm) and then the 7Fr EBU 3.0 catheter was advanced. The left main coronary artery was hooked, and there was severe calcium with tight stenosis in the left anterior descending artery astride a major septal branch. There was a 90-degree angle between the septal branch and the main branch of the LAD. The crossing of the left anterior descending artery lesion with 0.014 BMW wire through this catheter failed due to the calcific nodule and the 90-degree angle. Hence we pre dilated the tightest lesion with a non compliant balloon (APOLLO 2x 15mm) at high pressure. Due to the 90 degree angle we took the CRUSADE dual lumen micro catheter through the BMW wire, which was parked in the septal branch. Through the second lumen, 0.014 Fielder XT A wire was successfully crossed over the LAD lesion. In view of severe calcium rotational atherectome was done initially with 1.25mm burr and then upsized into 1.75mm burr. Later LAD was stented with two drug eluting stents 2.5 x 48mm and 2.75 x 28mm respectively. Post stenting there was type III perforation which was managed with balloon occlusion followed by pericardiocentesis and autotransfusion. Finally, GRAFTMASTER 2.8 x 19mm used to cover the leakage with the help of guide extension catheter.


Case Summary
Managing severely calcified lesions may require adjunctive devices to complete the procedure.In calcified lesions, image guided percutaneous coronary angioplasty with the help of optical coherence tomography or intravascular ultrasonography plays an important role in detecting the plaque morphology, severity, and depth of calcium. In circumferential deep calcium, intravascular lithotripsy helps to reduce the complications, hence be prepared for the worst in calcified lesions