
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-193
A Case of Acute Decompensated Heart Failure Due to Leadless Pacemaker Induced Dyssynchrony After TAVR Which Was Dramatically Improved by Cardiac Resynchronization Therapy Pacemaker
By Euihong Ko, Shinichi Shirai, Kenji Ando
Presenter
Euihong Ko
Authors
Euihong Ko1, Shinichi Shirai1, Kenji Ando1
Affiliation
Kokura Memorial Hospital, Japan1,
View Study Report
TCTAP C-193
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
A Case of Acute Decompensated Heart Failure Due to Leadless Pacemaker Induced Dyssynchrony After TAVR Which Was Dramatically Improved by Cardiac Resynchronization Therapy Pacemaker
Euihong Ko1, Shinichi Shirai1, Kenji Ando1
Kokura Memorial Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
O.M
Relevant Clinical History and Physical Exam
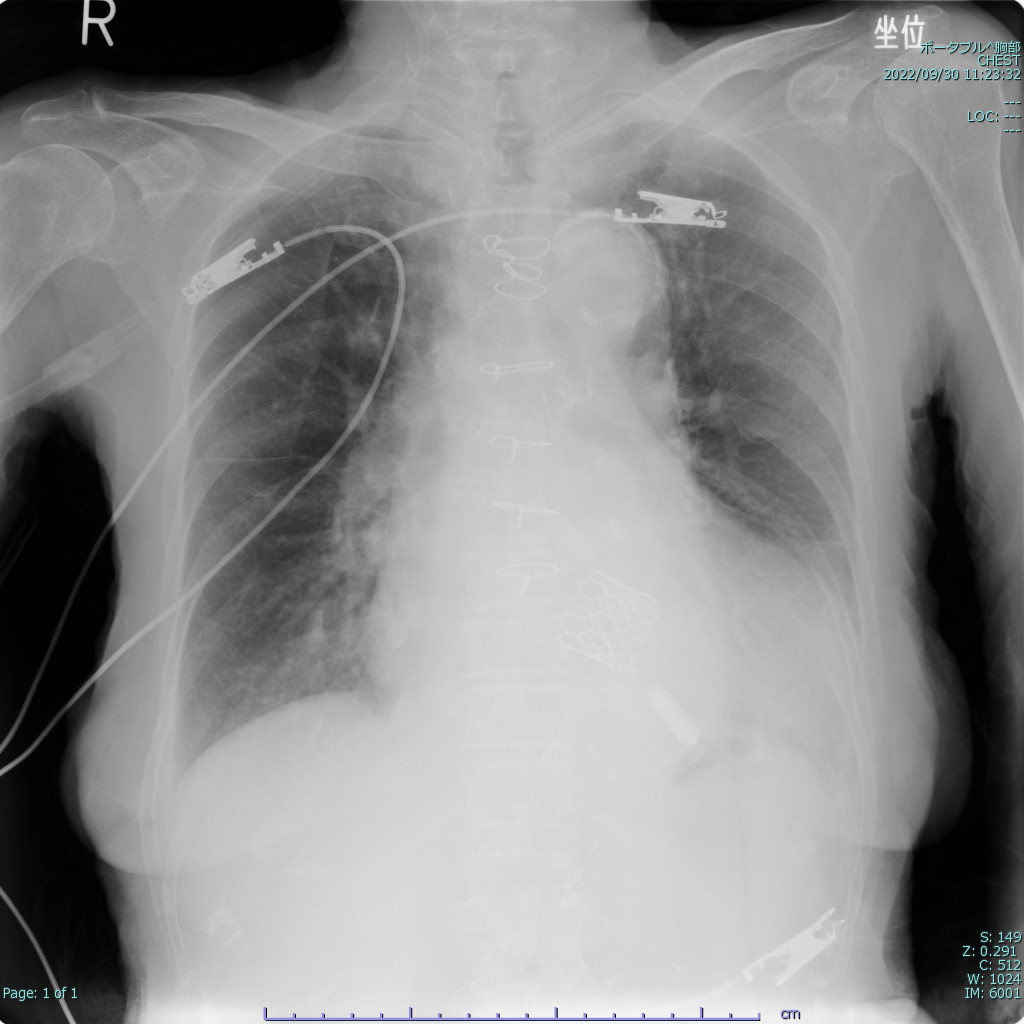
A 89-year-old woman was admitted to our institutiondue to acute decompensated heart failure (ADHF) with reduced ejection fraction(EF) with worsening dyspnea. She had history of severe aortic regurgitationwith mild aortic stenosis which had been treated with TAVR using SAPIEN 3 26mmin December 2021 and implanted leadless pacemaker due to complete atrioventricular block. Chest x-ray showed heart failure and echocardiography showed left ventricular dyssynchrony with severe mitral regurgitation.
Relevant Test Results Prior to Catheterization
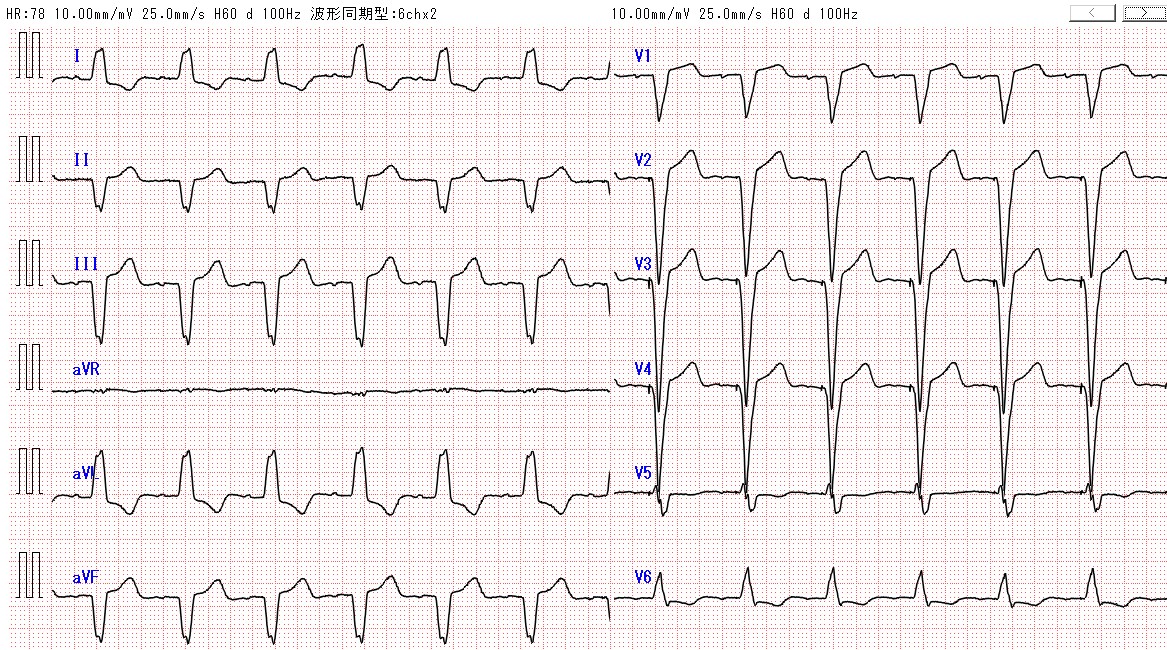
Dobutamine was started at 2.0μg/kg/minand diuretics was injected from admission. However, on the second day ofadmission, chest x-ray revealed worsening congestion requiring noninvasivepositive-pressure ventilation (NPPV), and intra-aortic balloon pump counterpulsation(IABP) to improve heart failure. The essential etiology of ADHF in this case isbecause of LV dyssynchrony caused by atrioventricular dyssynchrony and rightventricular pacing with LLPM.
Relevant Catheterization Findings
Interventional Management
Procedural Step
The essential etiology of ADHF in this case is because of LV dyssynchrony caused by atrioventricular dyssynchrony and right ventricular pacing with LLPM. Cardiac resynchronization therapy (CRT) was considered to be only effective treatment in this case, thus we implanted CRT-P on the 5th day of admission under IABP support. During the CRT-P upgrade procedure under local anesthesia, venography revealed patent left subclavian vein. To avoid additional left ventricular dyssynchrony, RV lead was screwed at the left ventricular septal subendocardium in the LBB region. The quadripolar LV lead was implanted lateral branch of coronary sinus and RA lead was implanted as usual method. The procedure was uneventful and optimal electrical parameters were obtained after one repositioning. Echocardiography was performed 4 days after CRT-P implantation demonstrating improved MR down to mild without any LV dyssynchrony. Chest x-ray also showed improved congestion and pleural effusion.
 01. LBBP 01.mp4
01. LBBP 01.mp4
04. CS lead placement.mp4
05. final.mp4
Case Summary
LLPMs represent a valuable alternative to transvenous pacemakers in different clinical scenarios, including lead malfunctions or upper-extremity venous thrombosis. We report a case with ADHF due to LV dyssynchrony caused by sustained RV pacing. PICM was successfully treated by upgrade to a biventricular pacemaker with an LV lead; stimulation of both RV and LV can reduce dyssynchrony and has been shown to improve heart failure.