
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-167
QFR Guided PCI the New Modality
By Sabapathy Diagarajan, Gurpreet Pal Singh Jugindar Singh, Mohd Ruslan Mustapa, Kengeswari Raja, Chen Tai Meng, Yew Fung Kwan, Hazleena Mohamed Hasnan, Nor Hanim Mohd Amin
Presenter
Sabapathy Diagarajan
Authors
Sabapathy Diagarajan1, Gurpreet Pal Singh Jugindar Singh2, Mohd Ruslan Mustapa3, Kengeswari Raja2, Chen Tai Meng2, Yew Fung Kwan2, Hazleena Mohamed Hasnan2, Nor Hanim Mohd Amin2
Affiliation
Hospital Pulau Pinang, Malaysia1, Hospital Raja Permaisuri Bainun, Malaysia2, Sultan Idris Shah Serdang Hospital, Malaysia3,
View Study Report
TCTAP C-167
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Physiologic Lesion Assessment
QFR Guided PCI the New Modality
Sabapathy Diagarajan1, Gurpreet Pal Singh Jugindar Singh2, Mohd Ruslan Mustapa3, Kengeswari Raja2, Chen Tai Meng2, Yew Fung Kwan2, Hazleena Mohamed Hasnan2, Nor Hanim Mohd Amin2
Hospital Pulau Pinang, Malaysia1, Hospital Raja Permaisuri Bainun, Malaysia2, Sultan Idris Shah Serdang Hospital, Malaysia3,
Clinical Information
Patient initials or Identifier Number
CSC
Relevant Clinical History and Physical Exam
He is a 65 years old gentleman non smoker admitted to district hospital had typical chest pain diagnosed as anterior myocardial infarction received thrombolytic therapy then discharged well. However since discharge he still had chest pain on exertion CCS II. He was brought in to our hospital for an angiogram. His BP 130/74 mmHg, heart rate 67 bpm other physical examination unremarkable.
Relevant Test Results Prior to Catheterization
ECG: sinus rhythm.
Echocardiogram: EF 44%, hypokinetic at anteroseptal region.
Blood investigations full blood count, renal profile, coagulation profile within normal limit.
Echocardiogram: EF 44%, hypokinetic at anteroseptal region.
Blood investigations full blood count, renal profile, coagulation profile within normal limit.
Relevant Catheterization Findings
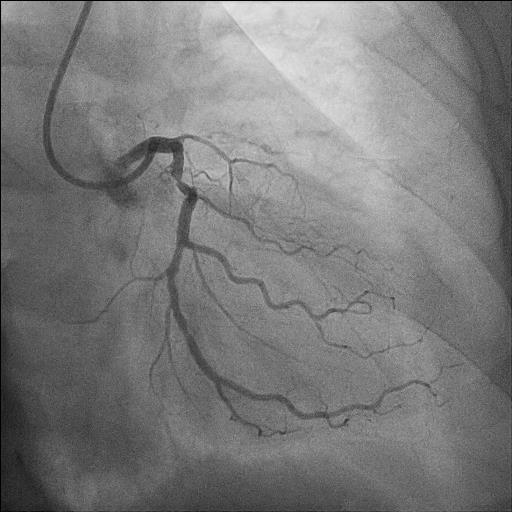
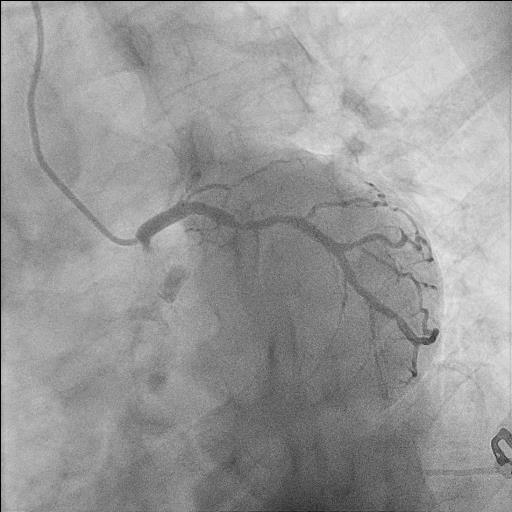
Coronary angiogram
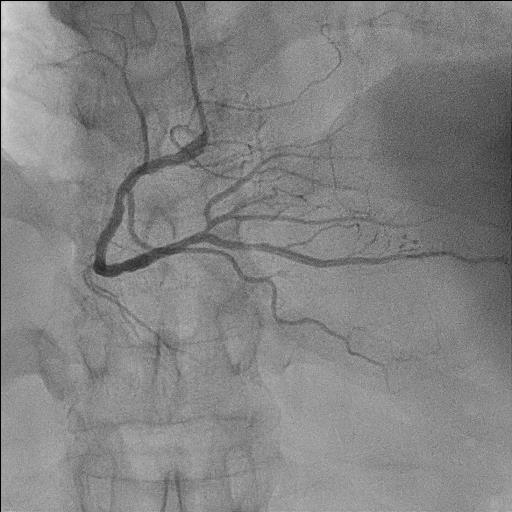
Left main: smoothLAD: Ostial LAD CTO, collaterals from RCALCx: mid LCx 70-80%RCA: Dominant, proximal 50-60%, mid 40%
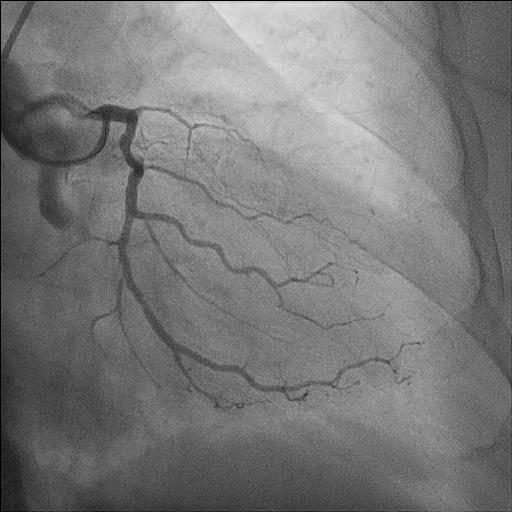
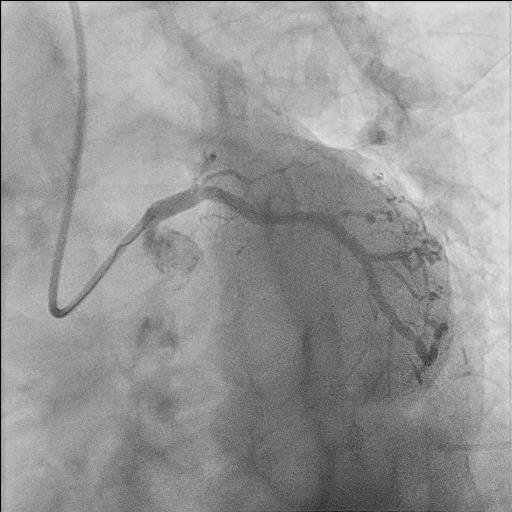
Left main: smoothLAD: Ostial LAD CTO, collaterals from RCALCx: mid LCx 70-80%RCA: Dominant, proximal 50-60%, mid 40%
Interventional Management
Procedural Step
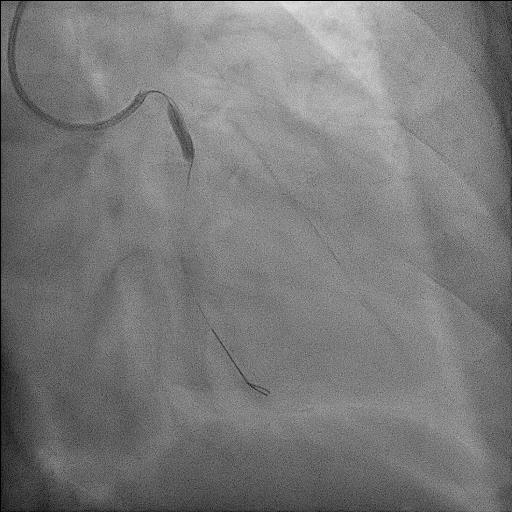
We proceeded with PCI to LCx QFR guided. Done via right radial approach 6F using guiding catheter EBU 3.5.
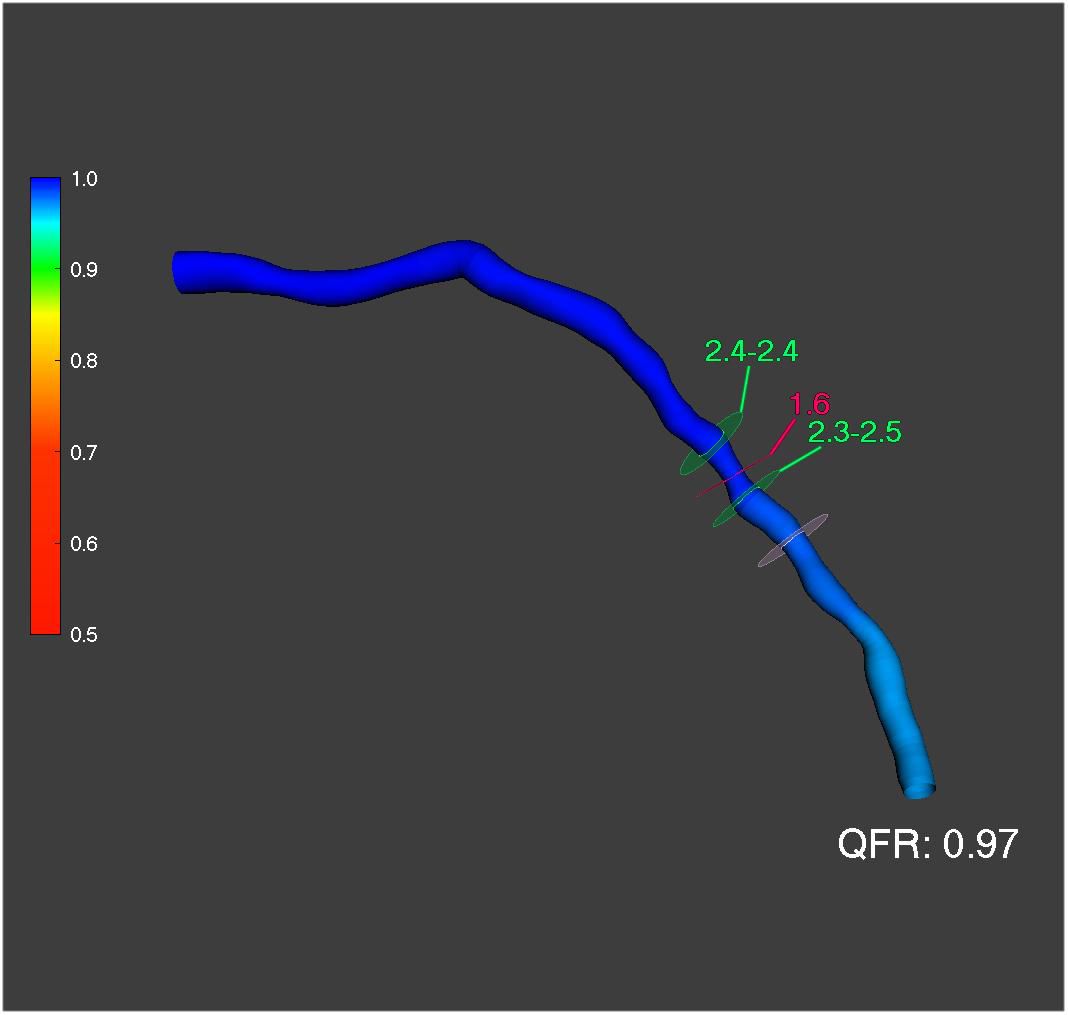
Adequate IC GTN given prior to QFR readings.QFR pre PCI 0.77.Sion blue wired into LCx.Predilated with semi compliant balloon 2.5 X 15mm @ 10 ATM, NC Scoring balloon 3.0 mm X 20mm @ 16 ATM.QFR post predilatation 0.93.Balloon angioplasty done at LCx with drug coated balloon(DCB) 3.0 X 20mm @ 7 ATM for 60 seconds.QFR post DCB 0.97.
Successful PCI to LCx with TIMI 3 flow seen. No dissection/perforation seen. No immediate complications seen.
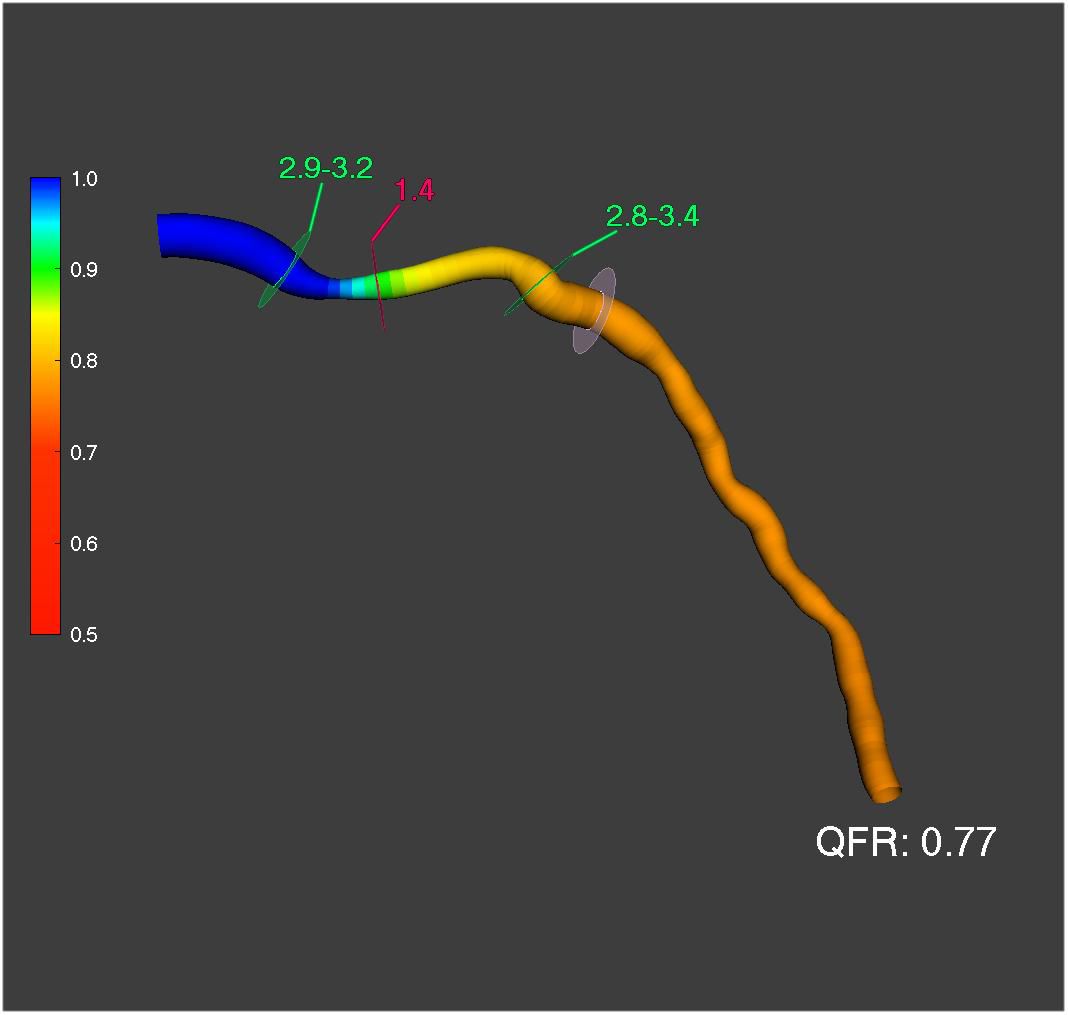
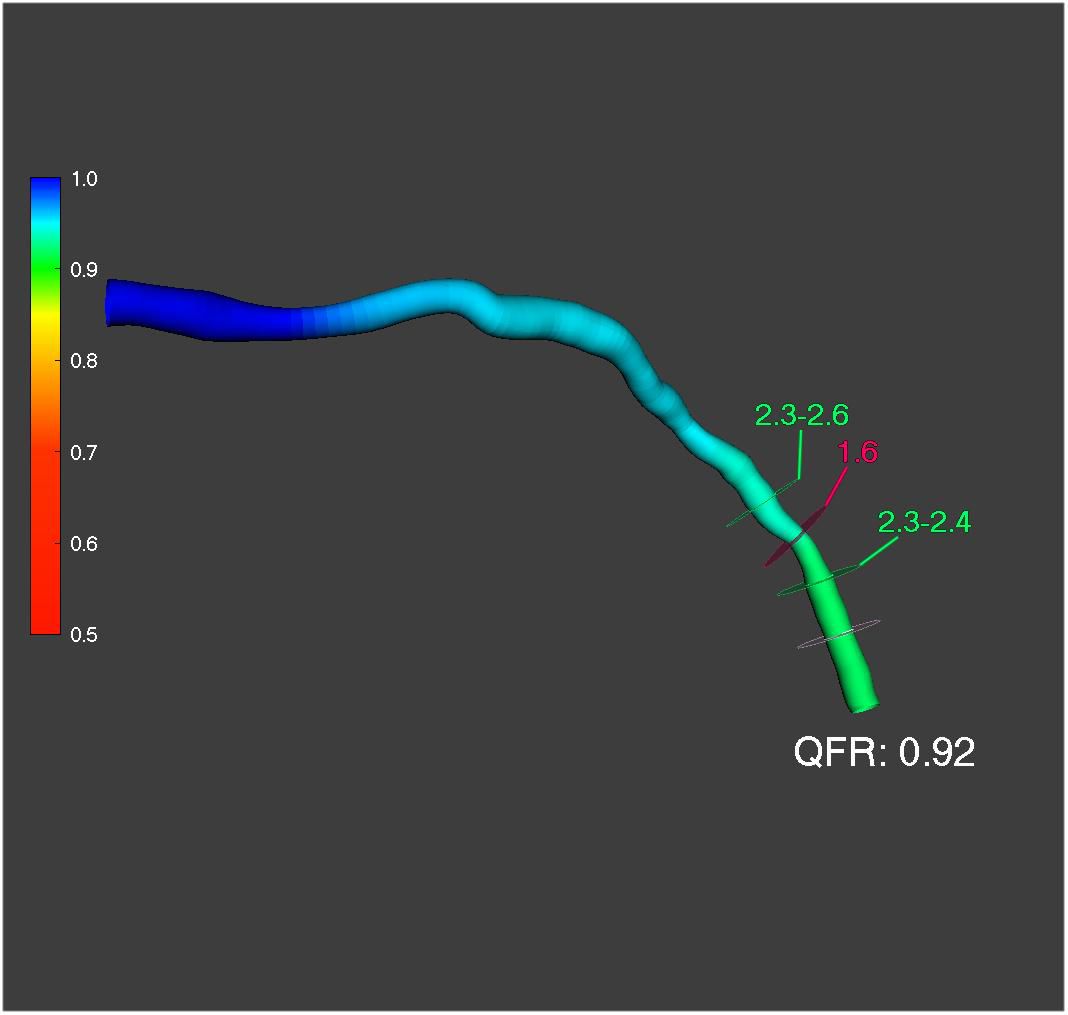
Adequate IC GTN given prior to QFR readings.QFR pre PCI 0.77.Sion blue wired into LCx.Predilated with semi compliant balloon 2.5 X 15mm @ 10 ATM, NC Scoring balloon 3.0 mm X 20mm @ 16 ATM.QFR post predilatation 0.93.Balloon angioplasty done at LCx with drug coated balloon(DCB) 3.0 X 20mm @ 7 ATM for 60 seconds.QFR post DCB 0.97.
Successful PCI to LCx with TIMI 3 flow seen. No dissection/perforation seen. No immediate complications seen.
Case Summary
Non invasive physiological ie QFR guided PCI has been new modality and widely used in current era. He is currently asymptomatic and planning for functional assessment keep in view to proceed stage PCI to CTO LAD later.