
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-197
Difficult Transcatheter Aortic Valve Implantation in a Bicuspid Aortic Stenosis With Eccentric Calcification and a Horizontal Ascending Aorta
By Debdatta Bhattacharyya, Manik Chopra, Ayan Kar, Snehil Goswami
Presenter
Snehil Goswami
Authors
Debdatta Bhattacharyya1, Manik Chopra2, Ayan Kar2, Snehil Goswami3
Affiliation
RN Tagore Hospital, India1, NH-Rabindranath Tagore International Institute of Cardiac Sciences, India2, NH MMI Hospital, India3,
View Study Report
TCTAP C-197
STRUCTURAL HEART DISEASE - Valvular Intervention: Aortic
Difficult Transcatheter Aortic Valve Implantation in a Bicuspid Aortic Stenosis With Eccentric Calcification and a Horizontal Ascending Aorta
Debdatta Bhattacharyya1, Manik Chopra2, Ayan Kar2, Snehil Goswami3
RN Tagore Hospital, India1, NH-Rabindranath Tagore International Institute of Cardiac Sciences, India2, NH MMI Hospital, India3,
Clinical Information
Patient initials or Identifier Number
MS
Relevant Clinical History and Physical Exam
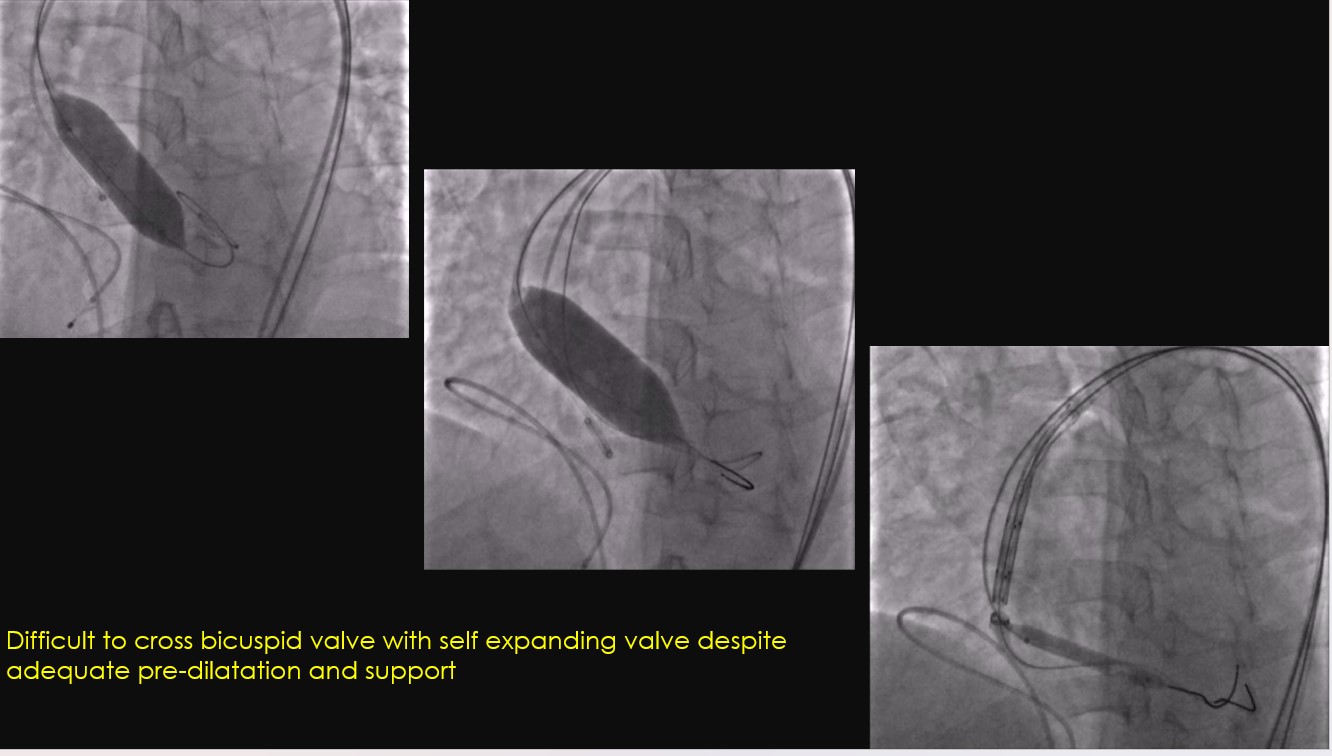
73-year diabetic and hypertensive with symptomatic severe aortic stenosis in a case of bicuspid aortic valve attempted with an Indian self expanding TAVR valve at a different hospital, but the valve could not be negotiated across the aortic valve referred to our center for a second attempt.
Relevant Test Results Prior to Catheterization
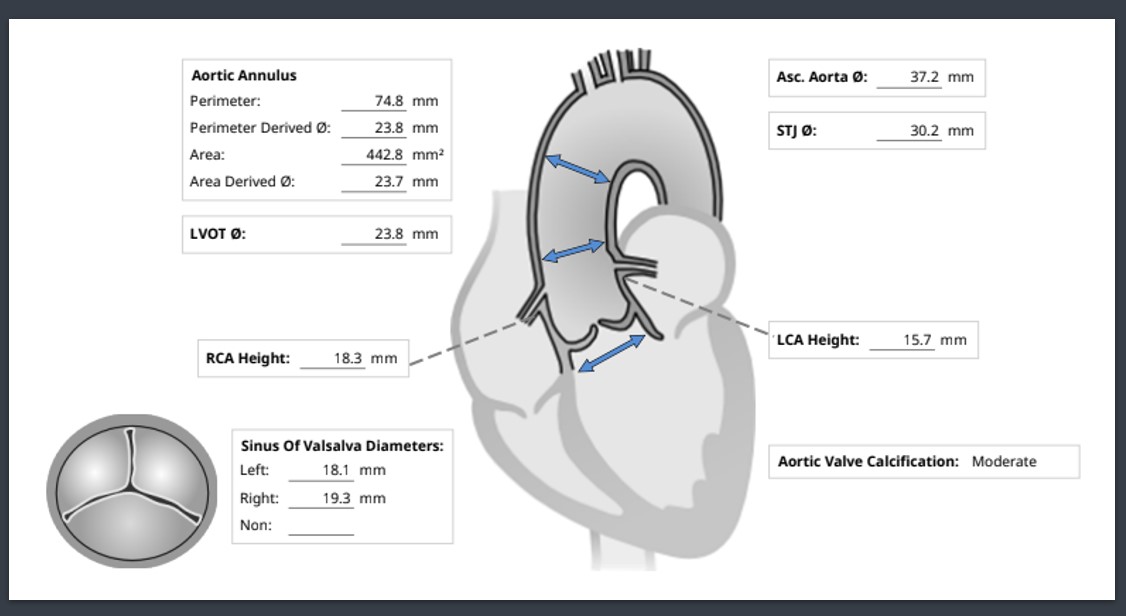
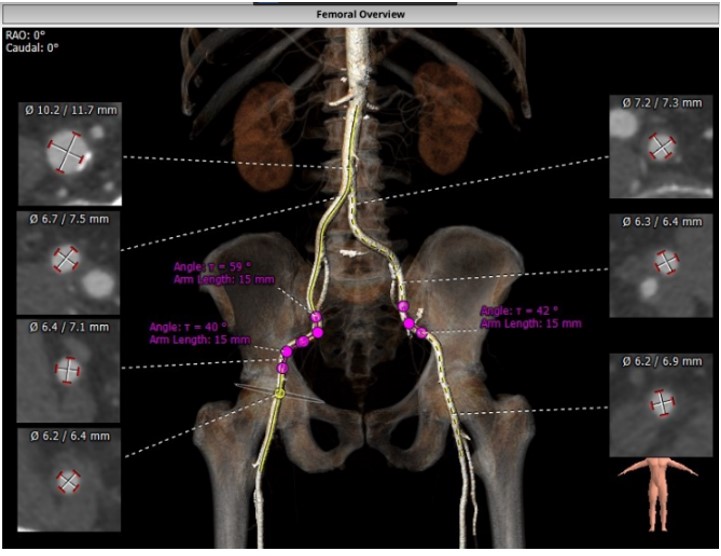
Hemoglobin 12.1, creatinine 0.68Echo concentric LVH, LV peak gradient 61 mm of Hg and mean gradient 36mm of Hg 3mension analysis of the aortic valve was done which showed an area-derived and a perimeter-derived aortic valve annulus of 23.7 mm and 23.8 mm respectively.The Ascending aorta measured 37.2 mm and coronary heights were adequate.peripheral common femoral access sites bilaterally measured more than 6 mm
Relevant Catheterization Findings
Pre TAVI:AO: 118/65/82 mm of Hg
Pre-TAVI peak gradient was 61 mm of Hg
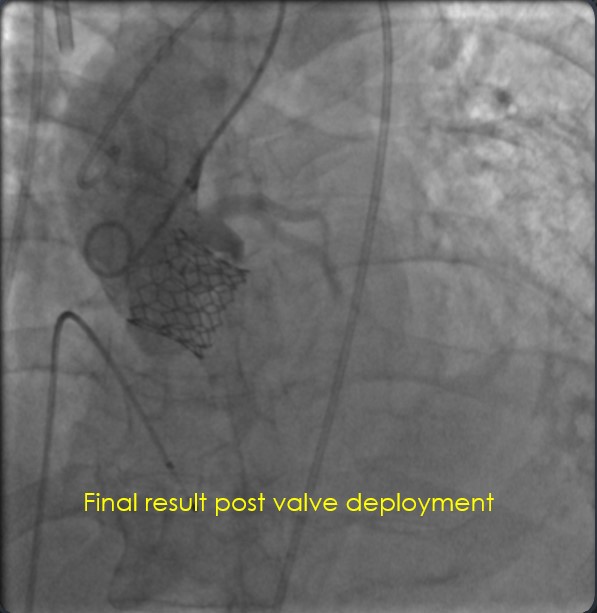
Post TAVI peak gradient 5mm of Hg
no significant AR at the end of procedure
Interventional Management
Procedural Step
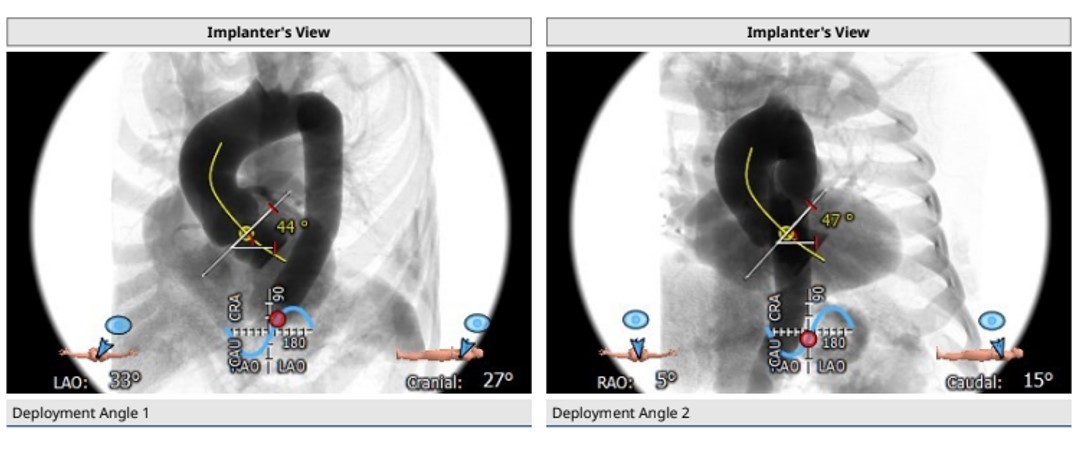
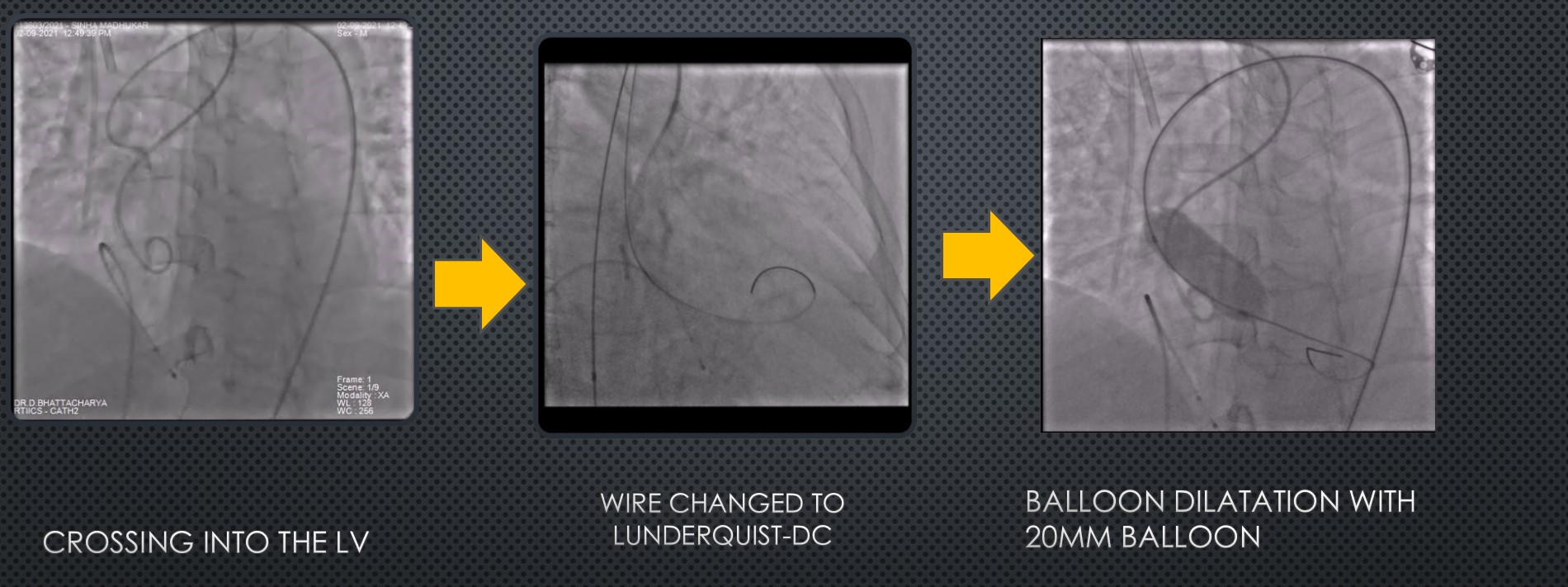
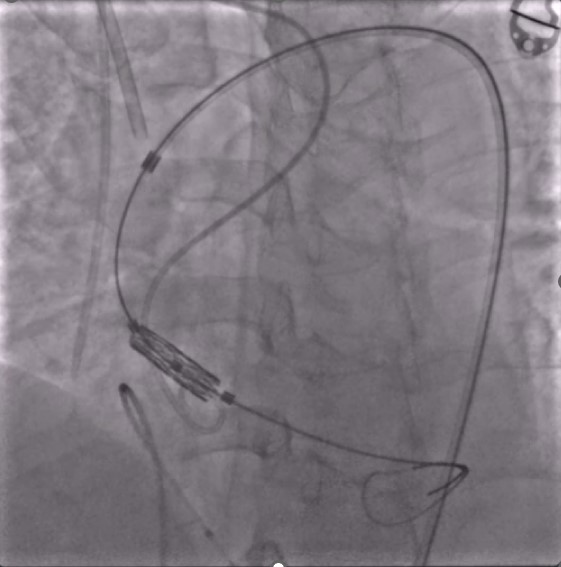
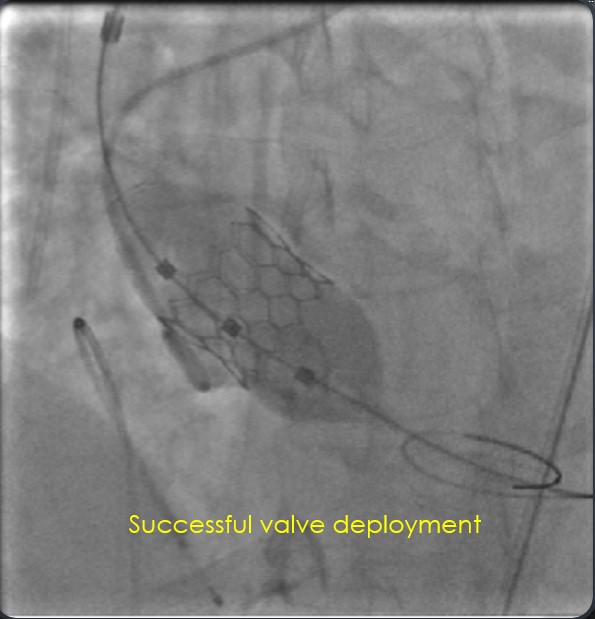
Right common femoral access was obtained under fluoroscopic and contralateral femoral dye injection.A 14 Fr Python sheath was inserted over an Amplatz super stiff wire parked in the ascending aorta. The valve was crossed with a 6F AL1 and straight-tip Terumo guide wire. The Terumo was exchanged for a Lunderquist double curve super stiff wire.the aortic valve was predilated with a 20x 40mm Mammoth OTW balloon under rapid-pacing support. Following which a 24.5 mm Myval (balloon expandable) valve was taken up to the ascending aorta. Given the horizontal nature of the ascending aorta, it was difficult to negotiate the valve and required deep flexion of the navigator balloon catheter to achieve coaxiality and negotiate the bicuspid valve with eccentric calcium . Following this and sustained traction, the valve finally jumped across the calcific hump of the aortic valve.It was deployed successfully under rapid-pacing support@ 180bpm and the final result was excellent. Common right femoral access was secured with a double ProGlide and temporary pacer was withdrawn on table .
Case Summary
Bicuspid aortic valve with eccentric calcification always presents a challenge for transcatheter Aortic valve implantation.It requires meticulous study of the pre-procedural CT imaging and planning for successful results.Bicuspid valve anatomy is peculiar for eccentrically placed calcium and difficult valve deployment across the eccentrically opening diseased aortic valve.The smaller profile of balloon expandable Myval (compared to the Indian self-expanding TAVR valve) along with the deep flexion on the navigator catheter helped in this case to negotiate the horizontal ascending aorta and eccentric calcium on the bicuspid aortic valve.