
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-018
Wrong Way. Always look Right and Left Before Crossing
By Mohamed Abed Bouraghda, Mohamed Amine Bouzid, Kamal Mouchene, Nazim Megherbi, Wathik Takdemt, Mohamed Chettibi, Mohamed Tahar Chafik Bouafia
Presenter
Mohamed Abed Bouraghda
Authors
Mohamed Abed Bouraghda1, Mohamed Amine Bouzid2, Kamal Mouchene1, Nazim Megherbi3, Wathik Takdemt1, Mohamed Chettibi1, Mohamed Tahar Chafik Bouafia1
Affiliation
CHU Frantz Fanon, Blida, Algeria1, Benimessous University Hospital, Algeria2, King AbdulAziz Specialist Hospital, Saudi Arabia3,
View Study Report
TCTAP C-018
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Wrong Way. Always look Right and Left Before Crossing
Mohamed Abed Bouraghda1, Mohamed Amine Bouzid2, Kamal Mouchene1, Nazim Megherbi3, Wathik Takdemt1, Mohamed Chettibi1, Mohamed Tahar Chafik Bouafia1
CHU Frantz Fanon, Blida, Algeria1, Benimessous University Hospital, Algeria2, King AbdulAziz Specialist Hospital, Saudi Arabia3,
Clinical Information
Patient initials or Identifier Number
M-B
Relevant Clinical History and Physical Exam
The patient was 52 years old, he presented for NSTEMI 7 hours after the onset of chest pain, the patient was hemodynamically stable ; SBP was 143 mmhg and DBP was 84 mmhg with abnormal biological parameters ;Troponines was in increasing cinetic , The patient was admitted in intensive care unit and coronary angiography was planned
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
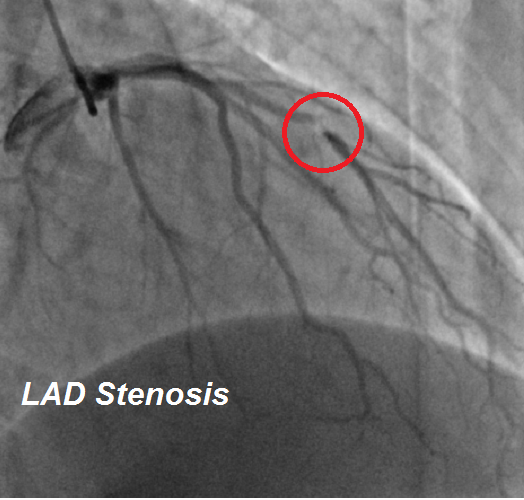
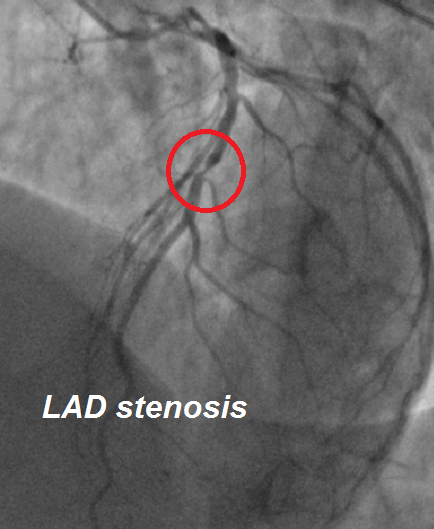
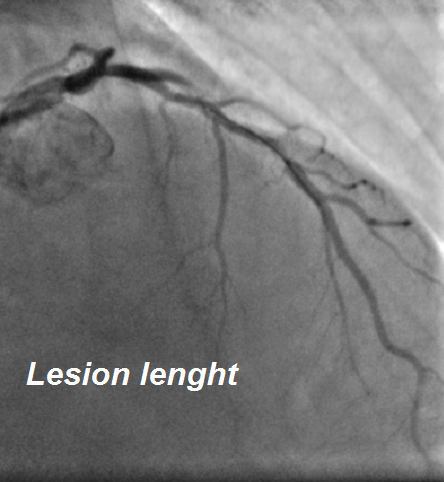
Coronary angiography was performed 10 hours after symptomes onset. The angiography showed a short and tight stenosis on the middle part of the LAD. The rest of the coronary arteries were free of significant lesions. The culprit lesion was considered a simple lesion and we decided to opt for direct stenting
Interventional Management
Procedural Step
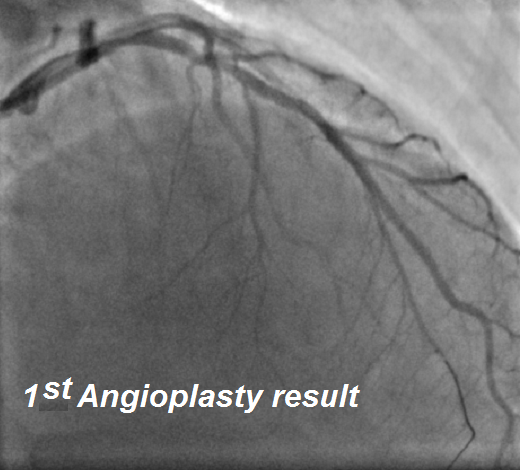
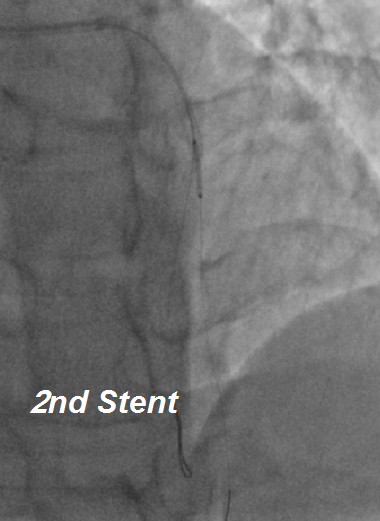
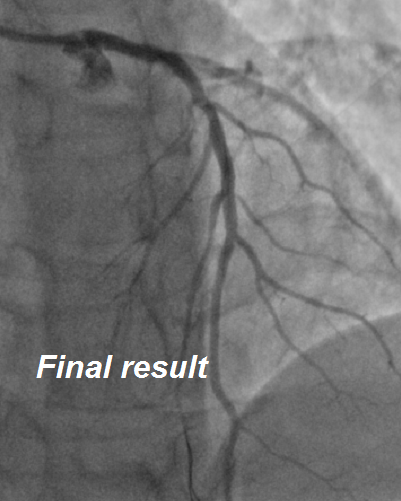
A floppg wire was advanced and placed distal to the stenosis on a cranial view, we took a third generation stent deployed at nominal pressure and completed the angioplasty with an angiographic control in the same view, the result was deemed satisfactory and we would have stopped there if the patient was not still complaining of chest pain. Checking the angioplasty in other views, it soon became apparent that the wire was on a large septal branch, completely superimposed on the LAD. We converted the procedure to a two-stent culottetechnique with a second stent on the LAD to complete the procedure with a good final result
Case Summary
In interventional cardiology, it would be wiser to consider that there is no "slam-dunk" angioplasy. An angioplasty failure can be caused by an error as simple as incorrect positioning of a wire in a parallel branch, an error easily avoidable by multiplying the views before and during the angioplasty.