
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-052
A Nightmare of Main Branch Ostium In-Stent Total Occlusion Intervnetion and Plaque Shift to Left Main Lesion: A Dilemma of Rescue Order
By Meitzu Wang, Wei-Chun Huang, Cheng-Chung Hung, Chin-Chang Cheng
Presenter
Meitzu Wang
Authors
Meitzu Wang1, Wei-Chun Huang1, Cheng-Chung Hung1, Chin-Chang Cheng1
Affiliation
Kaohsiung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-052
CORONARY - Bifurcation/Left Main Diseases and Intervention
A Nightmare of Main Branch Ostium In-Stent Total Occlusion Intervnetion and Plaque Shift to Left Main Lesion: A Dilemma of Rescue Order
Meitzu Wang1, Wei-Chun Huang1, Cheng-Chung Hung1, Chin-Chang Cheng1
Kaohsiung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Yo U C
Relevant Clinical History and Physical Exam
The 60-year-old male had coronary artery disease and underwent coronary stenting. He had angina in Canadian Cardiovascular Society angina grade 2. There were previous coronary stents deployed in segment 1, segement 6-7 and segement 11 from ostium.
Relevant Test Results Prior to Catheterization
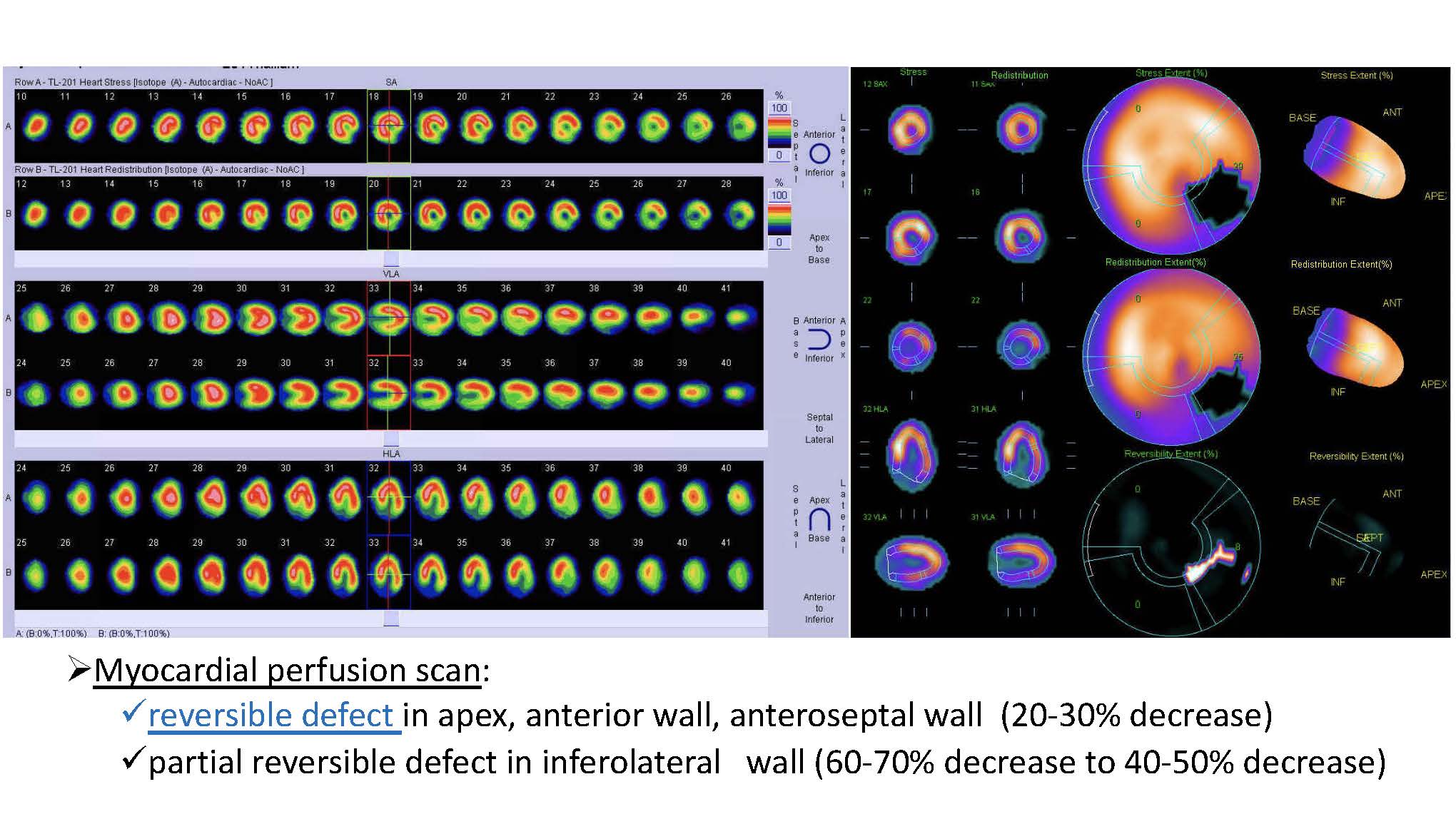
※Myocardial perfusion scan: reversible defect in apex, anterior wall, anteroseptal wall (20-30% decrease); partial reversible defect in inferolateral wall (60-70% decrease to 40-50% decrease). ※Estimated left ventricular ejectional fraction 56%
Relevant Catheterization Findings
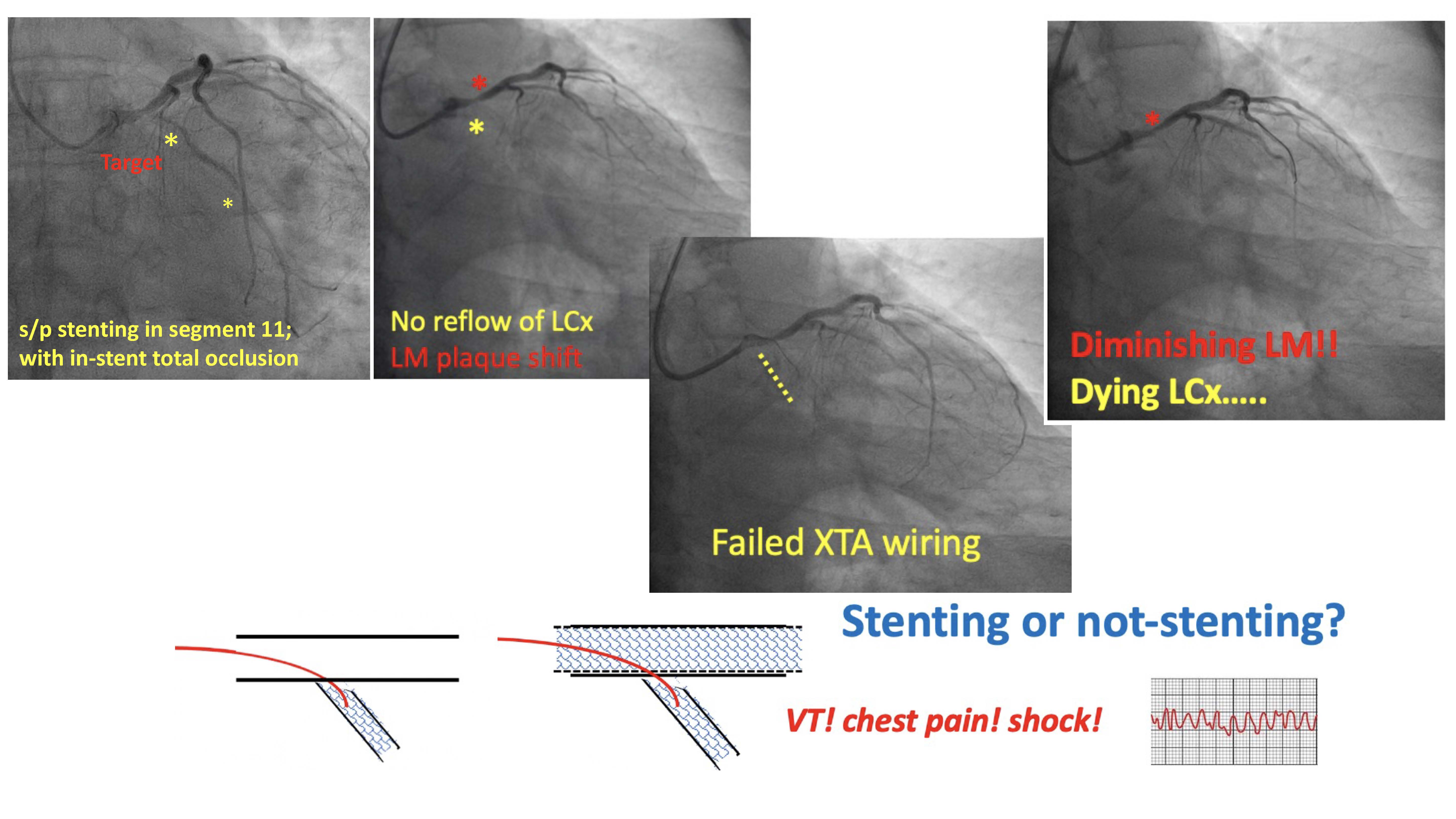
※LCx: -O:near total occlusion -P to -D:total occlusion -M:total occlusion
Interventional Management
Procedural Step
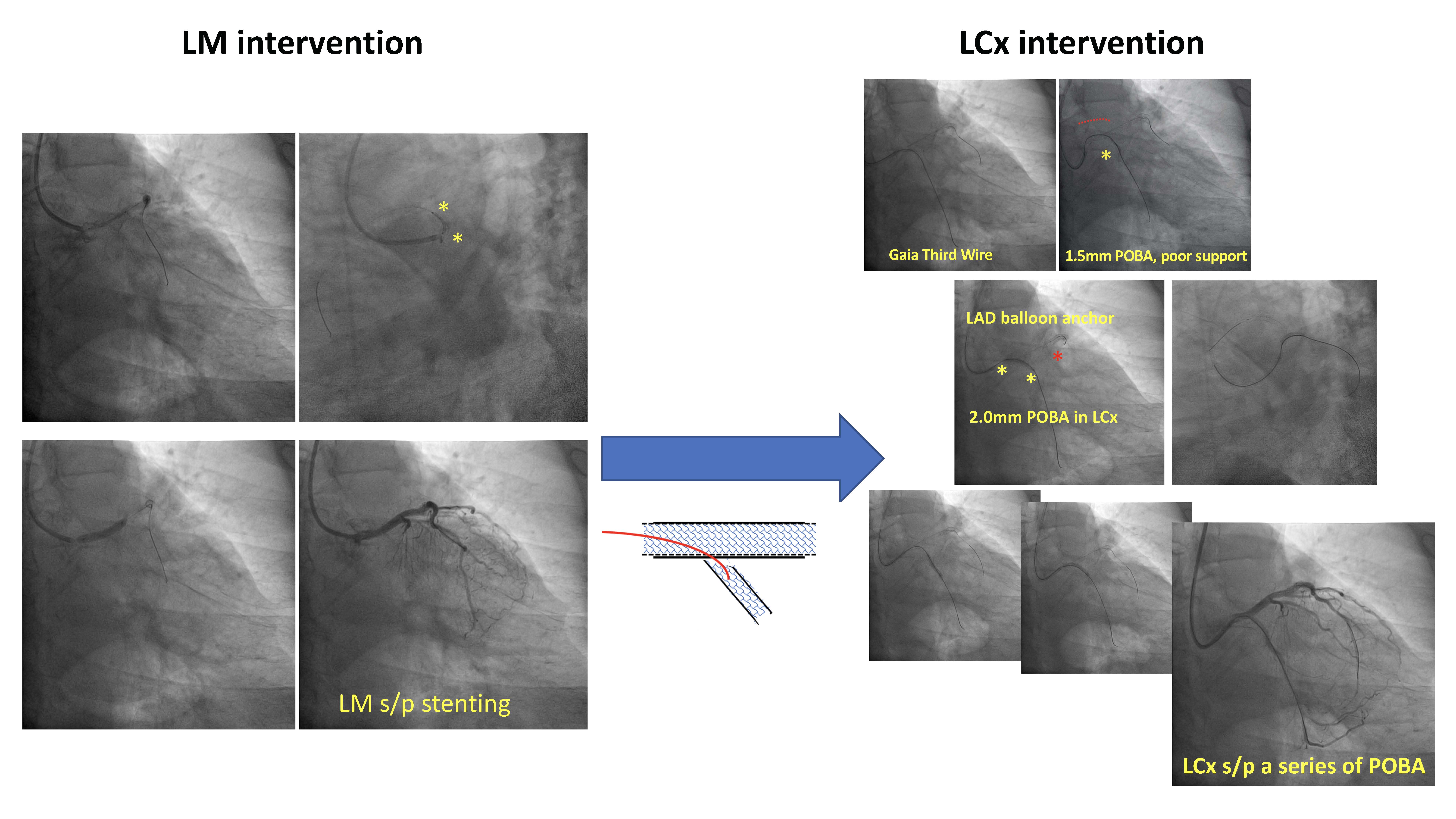
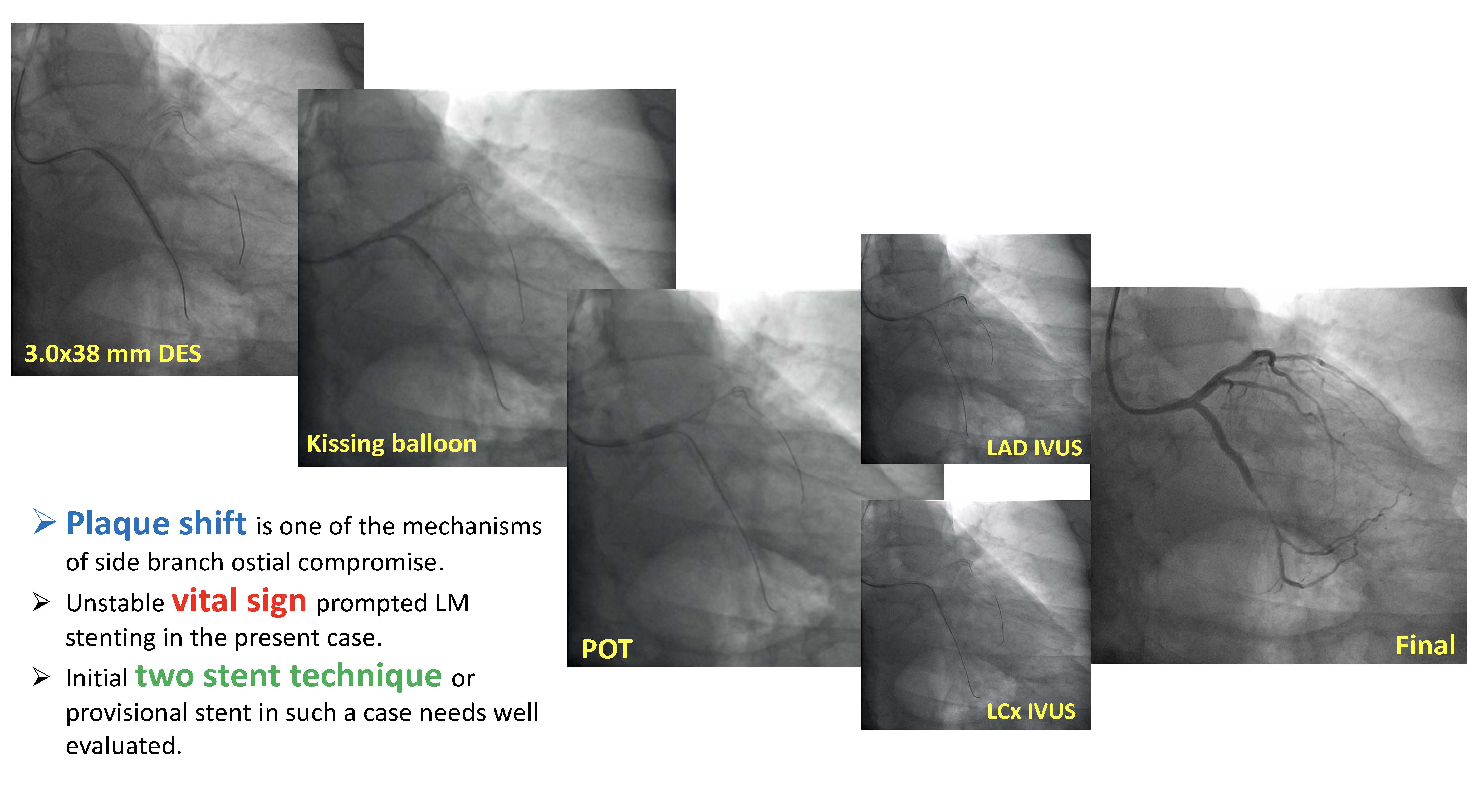
The patient unerwent percutanoues coronary intervention for in-stent ostium total occlusion lesion of left circumflex (LCx). However, during wiring attempin LCx, there was no reflow phenomenon of LCx and then plaque shifted to left main(LM). Patients complained of chest pain, and non-sustained VT attacked with associated hypotension. Vasoactive agent was prescribed, and after hemodynamic stabilzed, LM balloon dilation was done immediately. However, there was critical stenosis and failed to recanalized LM vessel. One drug-eluting stent (DES) with 3.0mm indiameter and 38mm in length was deployed in LM segment 5. LCx intervention was done under micricatheter support and Gaia Third 0.014" 190cm Guidewirepassed the chronic total occlusion cap. Balloon inflation and one DES stenting in LCx segment 11-13 with Culotte two stent technique were done. Moreover, kissing balloon technique abd POT were done after stenting. Final result was chescked by IVUS, and the result was optimal.
Case Summary
This is a LM bifurcation lesion, and intervention of LCx ostium complicated with plaque LM shift. The dilemma was that once LM was stented, the intervention to LCx CTO was more difficult. However, stable hemodynamic should be put on the first place. Intra-coronary image evaluation for optimal result was also important in complex PCI.