
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-174
Complex PCI in Chronic Kidney Disease – Made Possible With a Strategy
By Jesslyn Natalie Hariyanto, Sunanto Ng
Presenter
Jesslyn Natalie Hariyanto
Authors
Jesslyn Natalie Hariyanto1, Sunanto Ng1
Affiliation
Universitas Pelita Harapan, Indonesia1,
View Study Report
TCTAP C-174
OTHERS - Renal Insufficiency and Contrast Nephropathy
Complex PCI in Chronic Kidney Disease – Made Possible With a Strategy
Jesslyn Natalie Hariyanto1, Sunanto Ng1
Universitas Pelita Harapan, Indonesia1,
Clinical Information
Patient initials or Identifier Number
SHLV169069
Relevant Clinical History and Physical Exam
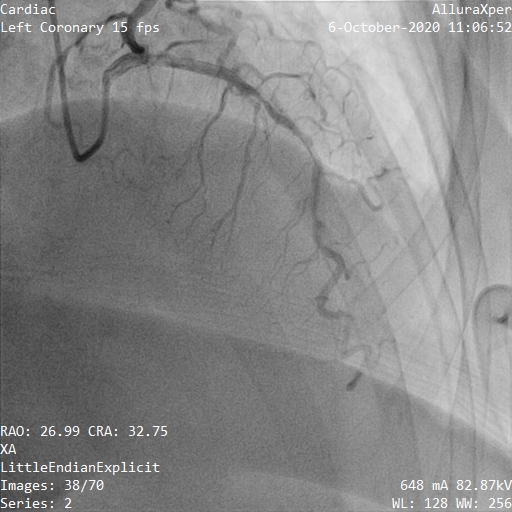
A 61 year old diabetic (controlled), hypertensive, female with hyperthyroidism (controlled) and stage IV CKD presented with CCS 3 angina and dyspnea on exertion. Her cardiopulmonary examination was normal. 2 years prior, angiography revealed diffuse three-vessel CAD with mid LAD calcification. She refused CABG and was managed with medical therapy. However, her angina persisted. We elected to proceed with PCI with special considerations for her reduced renal function.
Relevant Test Results Prior to Catheterization
Her 12-lead ECG showed normal sinus rhythm with no Q waves and no ST segment and T wave changes. Echocardiography showed an LVEF of 62% without regional wall motion abnormalities.
Relevant Catheterization Findings
Interventional Management
Procedural Step
Intravenous prehydration was administered for 2 days prior to procedure. Baseline renal function was obtained. PCI was planned to the RCA and LAD with an IVUS-guided minimal contrast approach and orbital atherectomy.
Diffuse lesions throughout the RCA were predilated with Sapphire 2.0/15. IVUS showed diffuse lesion with moderate calcification, MLA of 2.35 mm2. Lesion preparation was done with Wolverine 3.0/15 (Boston Scientific, USA) stented with Orsiro 3.0/40 and Orsiro 3.5/40 (Biotronik, Germany) and postdilated with NC Pantera Leo 3.25/15 (Biotronik, Germany) and NC Sprinter 3.75/21 (OrbusNeich, Hong Kong). IVUS (Boston Scientific, USA) showed good stent expansion and overlap without malapposition, MSA 7.58 mm2.
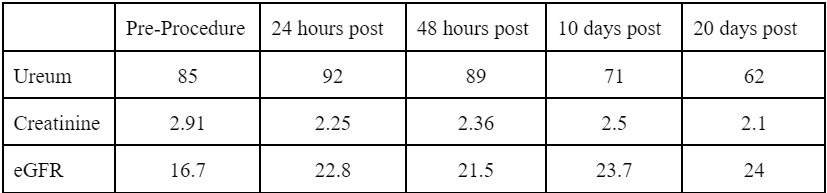
The procedure was completed without complications. A total of 23 ml of Iomeron contrast (Bracco Imaging, Italy) was used. Ureum and creatinine remained consistent and eGFR was preserved. She was well at discharge without symptoms.

Diffuse lesions throughout the RCA were predilated with Sapphire 2.0/15. IVUS showed diffuse lesion with moderate calcification, MLA of 2.35 mm2. Lesion preparation was done with Wolverine 3.0/15 (Boston Scientific, USA) stented with Orsiro 3.0/40 and Orsiro 3.5/40 (Biotronik, Germany) and postdilated with NC Pantera Leo 3.25/15 (Biotronik, Germany) and NC Sprinter 3.75/21 (OrbusNeich, Hong Kong). IVUS (Boston Scientific, USA) showed good stent expansion and overlap without malapposition, MSA 7.58 mm2.
IVUS to the LAD revealed extensive calcification with napkin ring at the mid LAD, MLA of 2.16 mm2. 4 low speed runs of the Diamondback® (Cardiovascular Systems Inc, USA) OAS were delivered to the mid LAD, followed by NC Scoreflex 2.75/20 (OrbusNeich, Hong Kong), stented with Orsiro 2.75/40 and postdilated with Pantera Leo 3.25/15. IVUS showed good stent expansion without edge dissection and malapposition, MSA 8.62 mm2.
The procedure was completed without complications. A total of 23 ml of Iomeron contrast (Bracco Imaging, Italy) was used. Ureum and creatinine remained consistent and eGFR was preserved. She was well at discharge without symptoms.
Case Summary
The two largest predictors of contrast-induced nephropathy are baseline creatinine and volume of contrast used. In the interest of not tipping over her borderline renal function, a revascularization strategy is possible by opting for a minimal contrast approach supported by short injections, intravascular imaging and preparation of adjunctive calcium modification devices where necessary.