
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-076
A Case of Successful PCI of RCA Chronic Total Occlusion (CTO) With AnteOwl WR™ IVUS-Guided Parallel Wiring Technique for Recanalization From a Large False Lumen
By Yukihiro Yamaguchi, Toshiya Muramatsu, Reiko Tsukahara, Masatsugu Nakano, Hideyuki Takimura, Satoru Nishio, Yukako Takimura, Mami Kawano, Emi Tajima, Ippei Tsuzuki, Rintaro Taniguchi
Presenter
Yukihiro Yamaguchi
Authors
Yukihiro Yamaguchi1, Toshiya Muramatsu2, Reiko Tsukahara3, Masatsugu Nakano3, Hideyuki Takimura3, Satoru Nishio3, Yukako Takimura3, Mami Kawano3, Emi Tajima3, Ippei Tsuzuki3, Rintaro Taniguchi3
Affiliation
International University of Health and Welfare, Japan1, Tokyo Heart Center, Japan2, Tokyo General Hospital, Japan3,
View Study Report
TCTAP C-076
CORONARY - Chronic Total Occlusion
A Case of Successful PCI of RCA Chronic Total Occlusion (CTO) With AnteOwl WR™ IVUS-Guided Parallel Wiring Technique for Recanalization From a Large False Lumen
Yukihiro Yamaguchi1, Toshiya Muramatsu2, Reiko Tsukahara3, Masatsugu Nakano3, Hideyuki Takimura3, Satoru Nishio3, Yukako Takimura3, Mami Kawano3, Emi Tajima3, Ippei Tsuzuki3, Rintaro Taniguchi3
International University of Health and Welfare, Japan1, Tokyo Heart Center, Japan2, Tokyo General Hospital, Japan3,
Clinical Information
Patient initials or Identifier Number
NS 258456
Relevant Clinical History and Physical Exam
The patient was a male in his 50s and his diagnosis was SMI (Silent Myocardial Ischemia). CAG showed CTO at #3-4 AV in a previous hospital, but PCI was failure. Then he was referred to our hospital. LVEF was 58% (UCG) and eGFR was 74 (ml/min/1.73m2).
Relevant Test Results Prior to Catheterization
Cardiac CT showed that the entry site of CTO was tapered and there was no severe calcification. The lesion was so tortuous and there was RV branch just before the lesion. The predicted occlusion length was 40 mm (J-CTO score 3).
Relevant Catheterization Findings
The initial angiography showed the CTO at RCA distal seg. 3 occluded from RV branch. The collateral channel was absent from LCA and that of from RV branch to seg. 4 was very poor, therefore, the retrograde approach was not an option. We would like to show the bail-out procedures.
Interventional Management
Procedural Step
We tried to cross the lesion with FINE CROSS GT and XT-R from the antegrade, but the tip of the wire strayed into the myocardium through the false lumen, causing leakage of contrast medium into it. In addition, a large dissection was found in RCA. It was a perforation within the CTO and did not lead to cardiac tamponade. Then, a parallel wiring technique was attempted under AnteOwl WR™ intravascular ultrasound (AO-IVUS) guidance. AnteOwl WR™ is a new IVUS specifically developed in Japan for CTO-PCI. Tip-to-sensor position is as short as 8mm and the shaft is reduced in diameter to 3.1Fr, allowing simultaneous use of IVUS and 2 micro catheters or micro catheter and 0.014 guidewire within a 7Fr guide catheter.
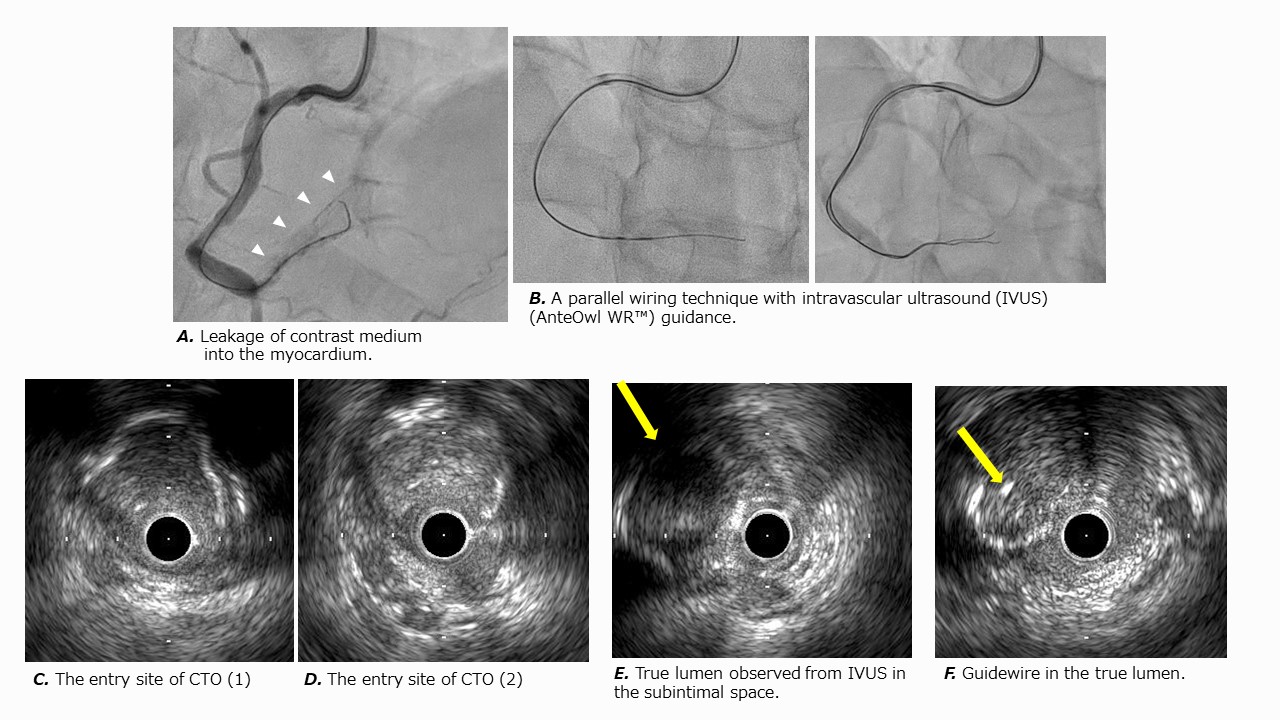
Case Summary
We performed a successful PCI of RCA chronic total occlusion (CTO) with AO-IVUS-guided parallel wiring technique for recanalization from a large false lumen. AnteOwl WR™ is ideal for IVUS-guided PCI because of its short tip-to-sensor distance, small shaft diameter, and good passability.