
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-057
The Last Hope
By Swee En Goay, Hafidz Abd Hadi, Mugilan Sundarajoo
Presenter
Swee En Goay
Authors
Swee En Goay1, Hafidz Abd Hadi1, Mugilan Sundarajoo2
Affiliation
National Heart Institute, Malaysia1, National Heart Institute Ijn, Malaysia2,
View Study Report
TCTAP C-057
CORONARY - Bifurcation/Left Main Diseases and Intervention
The Last Hope
Swee En Goay1, Hafidz Abd Hadi1, Mugilan Sundarajoo2
National Heart Institute, Malaysia1, National Heart Institute Ijn, Malaysia2,
Clinical Information
Patient initials or Identifier Number
AB
Relevant Clinical History and Physical Exam
A 50 year-old ex-army man presented with worsening chest pain with reduced effort tolerance for 1 week. He has Diabetes, Hypertension and had CABG with 4 grafts in 2011 after a myocardial infarction. His heart rate was 105 bpm and blood pressure of 110/70mmHg. Clinical examination is unremarkable.
Relevant Test Results Prior to Catheterization
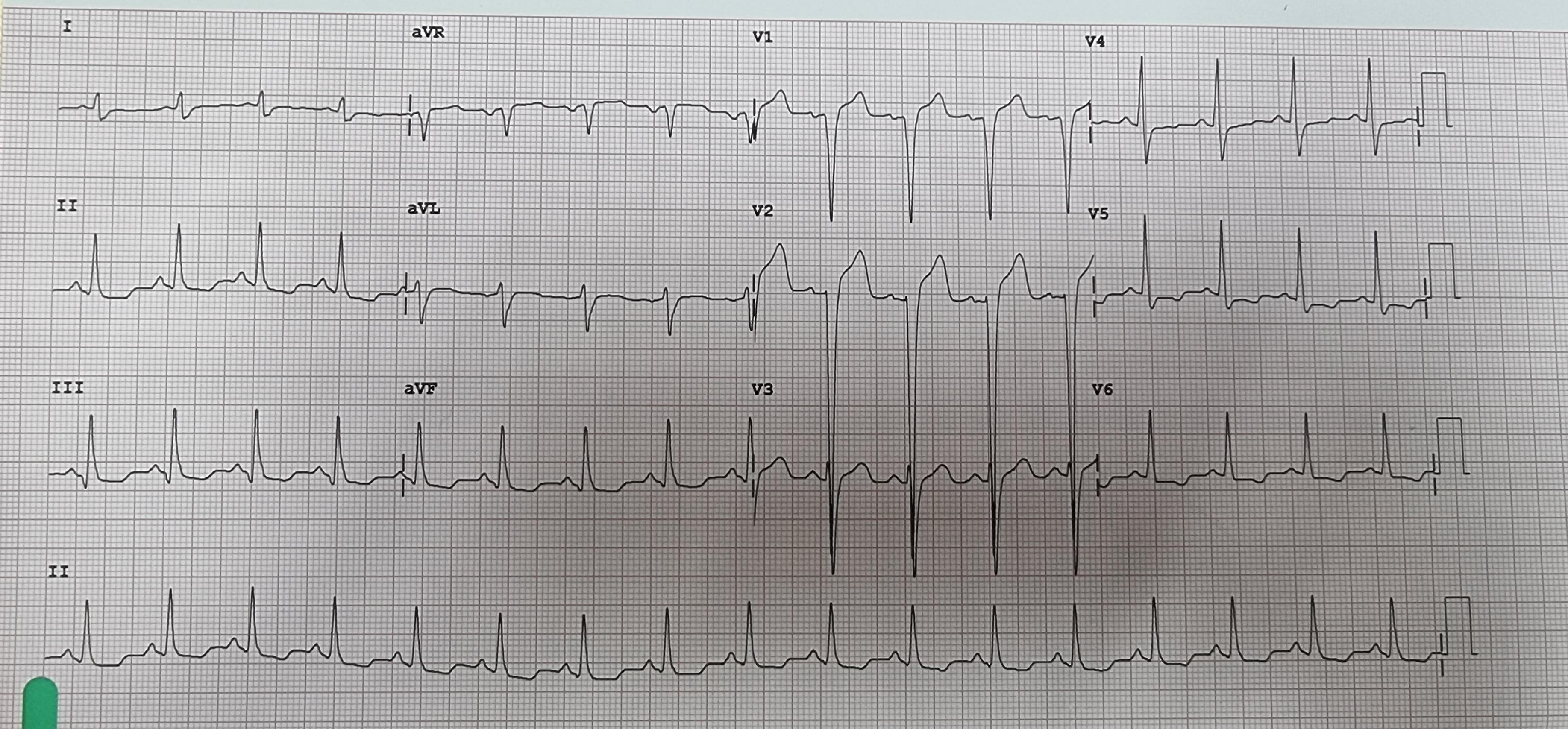
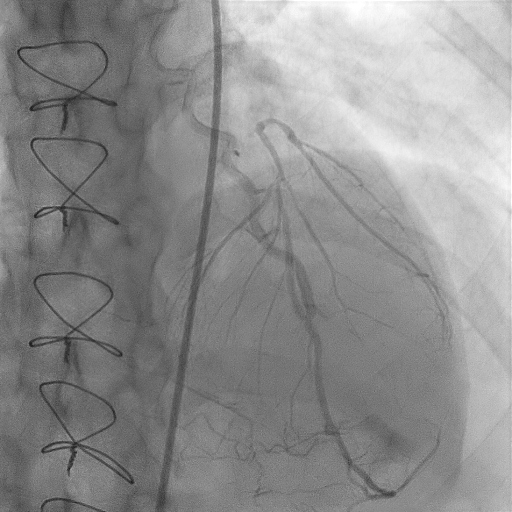
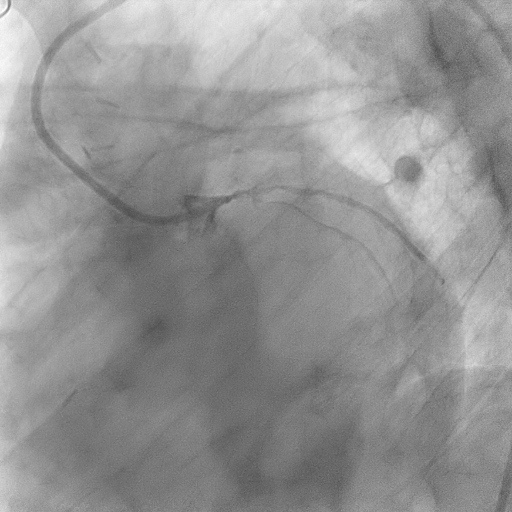
Relevant Catheterization Findings
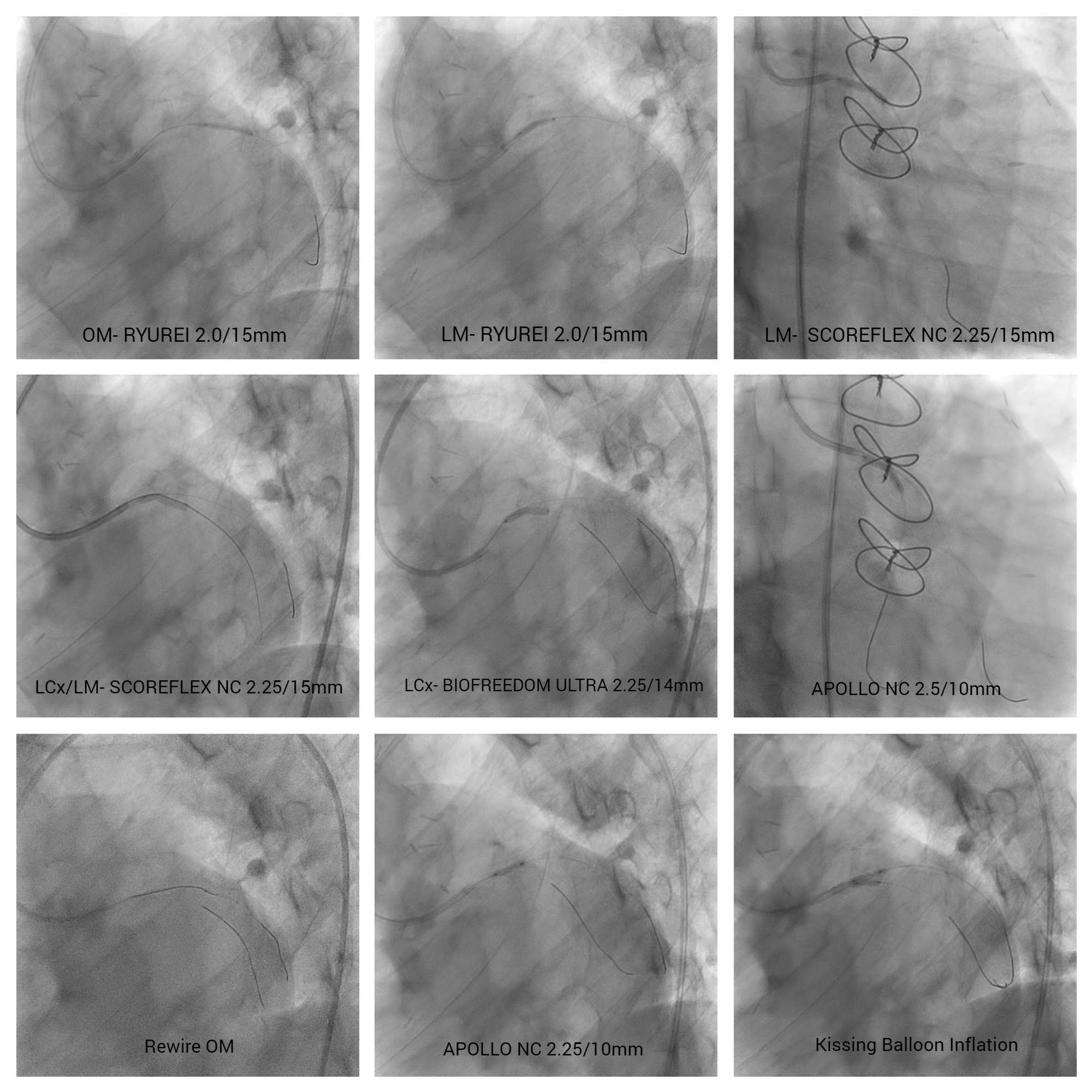
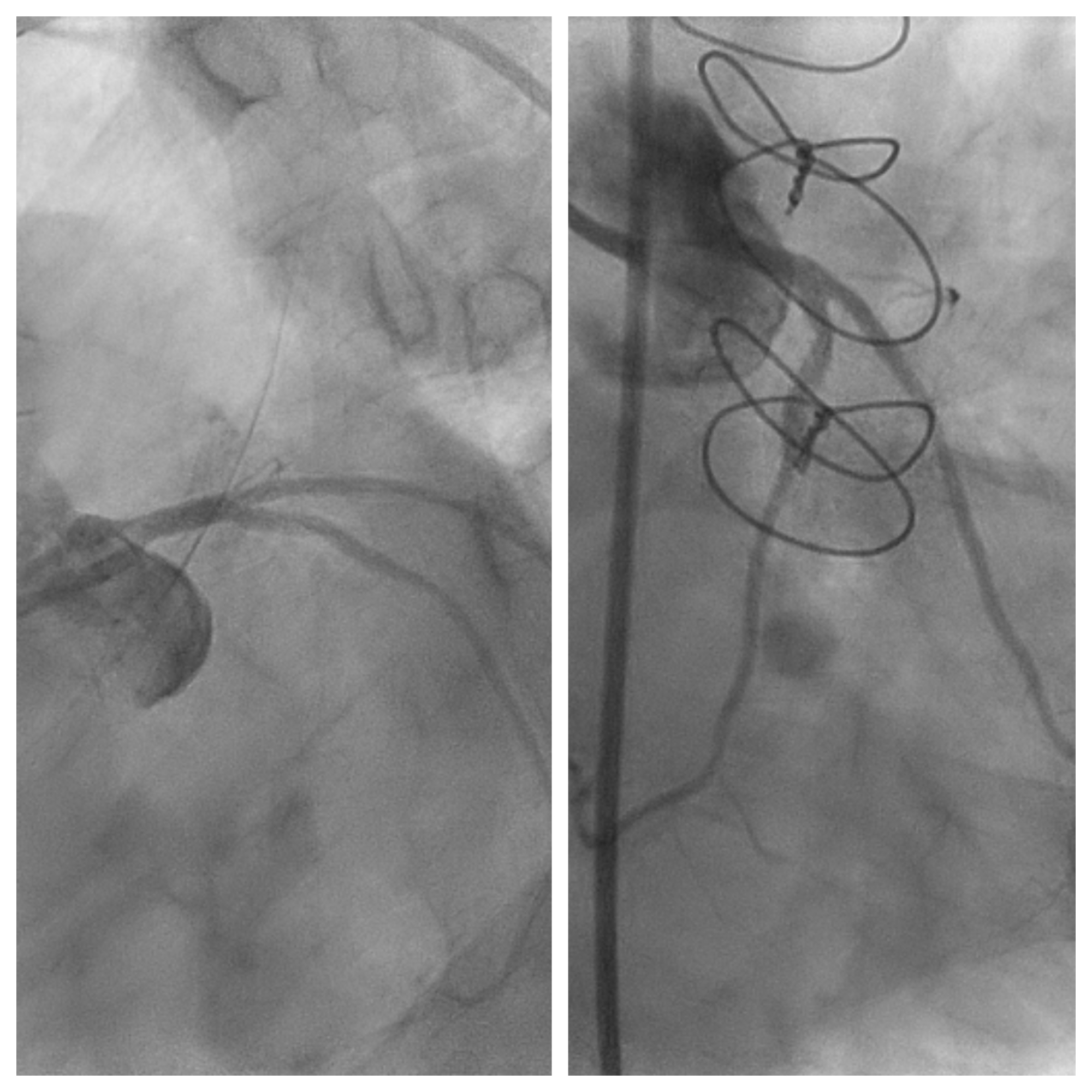
Coronary angiogram showed severely diseased Left main (LM) with chronic total occlusion Left anterior descending (LAD) and severe stenosis at the ostial & proximal segments of an angulated Left circumflex (LCx) with calcification & also the ostium of the Obtuse marginal (OM) (Medina 1,1,1). Right coronary artery (RCA) had chronic total occlusion from proximal with side branch collaterals. Graft study revealed only a patent LIMA-LAD graft.
Interventional Management
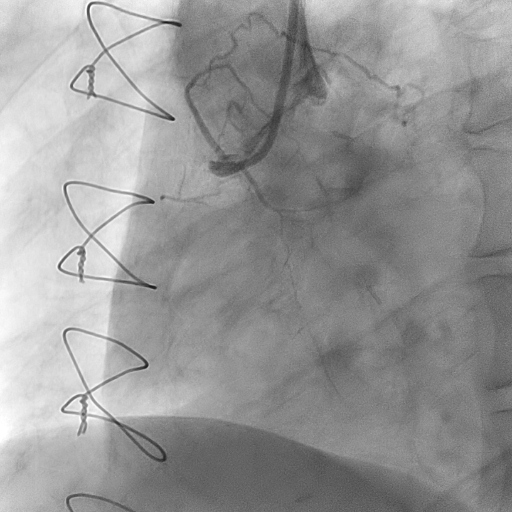
Procedural Step
Percutaneous Intervention to LM/LCx & OM using an EBU 3.5/6Fr guiding catheter via Right femoral with 6Fr sheath. We first predilated the proximal &Ostial OM till the LM (MB)with RYUREI 2.0/15mm up to 14atm then with SCOREFLEX NC 2.25/15mm up to 14atmafter crossing it with Run through floppy workhorse wire. This was done to facilitate the wiring of both OM (MB) & the angulated LCx (SB). By using FIELDER XT, we were able to cross the ostial LCx lesion and predilated it with SCOREFLEX NC 2.25/15mm up to LM with 20atm. FIELDER XT was exchanged to SION BLUE then to Grandslam for better support using the FINECROSS microcatheter. Further predilation with SCOREFLEX NC 2.25/15mm up to 22atm again before stented LM-LCx with BIOFREEDOM ULTRA 2.25/14mm followed by postdilation with APOLLO NC 2.5/10mm up to 22atm.

Case Summary
Coronary bifurcation stenting remains a complex procedure with high risk of stent thrombosis and restenosis even with contemporary techniques. Culotte stenting technique was used in this patient with similar vessel size of OM & LCx. His calcified vessels and angulated LCx was a challenge to us in wiring and deploying the stent, however we were able to do so with adequate vessel preparation and different coronary guide wires. Vessel diameter between the branches and the concept of plaque shift and carina shift is important in determining the strategy in bifurcation stenting, also the training experience of the operator.