
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-157
Case Report: Endovascular Thrombectomy in Woman With Deep Vein Thrombosis
By Chung-Ying Lu, Jen-Kuang Lee
Presenter
Chung-Ying Lu
Authors
Chung-Ying Lu1, Jen-Kuang Lee1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-157
ENDOVASCULAR - Peripheral Vascular Disease and Intervention
Case Report: Endovascular Thrombectomy in Woman With Deep Vein Thrombosis
Chung-Ying Lu1, Jen-Kuang Lee1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
64-year-old female
Relevant Clinical History and Physical Exam
She suffered from progressive dyspnea and intermittent fever; she visited emergency depart and disclosed severe anemia and leukocytosis with blast; acute myeloid leukemia was suspected, and she was admitted. Cytoreduction therapy was initiated and survey for leukemia was conducting, but leg edema developed during admission. Grade 4 pitting edema of right leg was noted; symptom extended from sole to thigh.

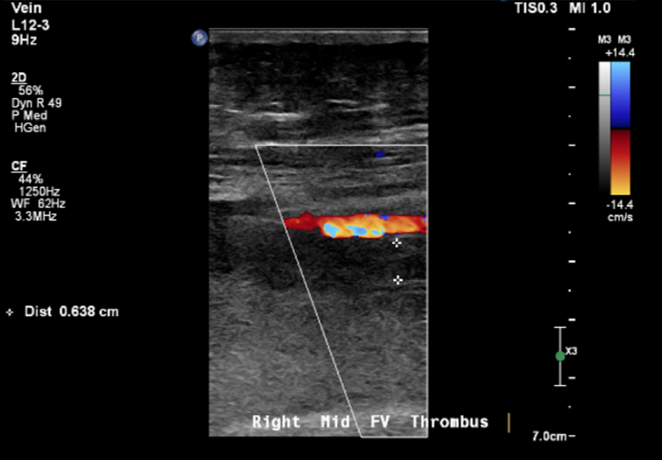
Relevant Test Results Prior to Catheterization
Vascular ultrasound showed thrombosis over greater saphenous vein, common femoral vein and popliteal vein. Lower extremities CT scan showed diffuse thrombosis from popliteal vein to right iliac vein.


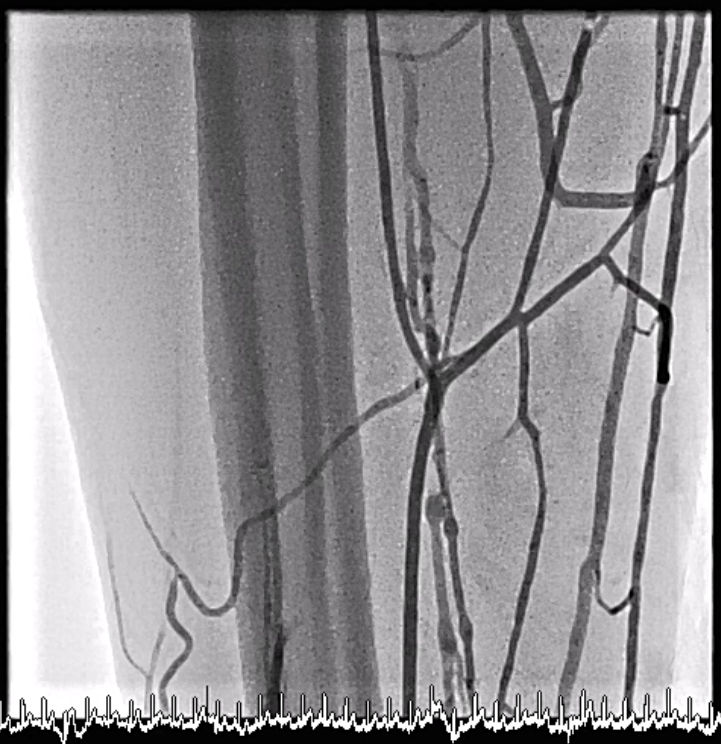
Relevant Catheterization Findings
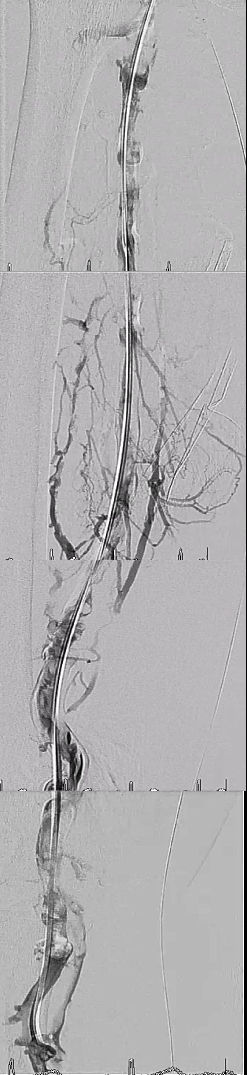
Antegrade venogram was performed via right foot IV catheter and showed occlusion of great saphenous vein and below knee veins, with prominent collateral veins. Retrograde venogram via left femoral vein approach showed suspect right external iliac vein thrombosis with occlusion.


Interventional Management
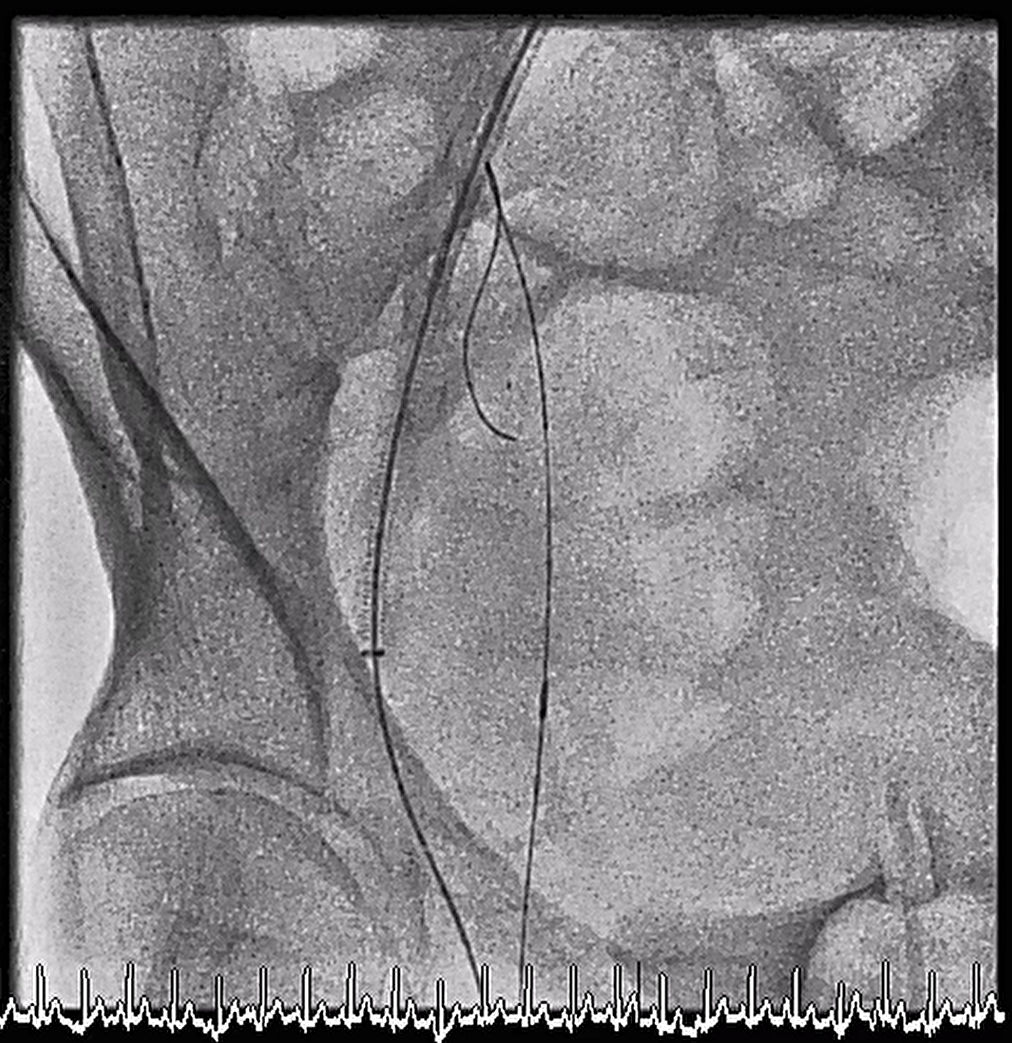
Procedural Step
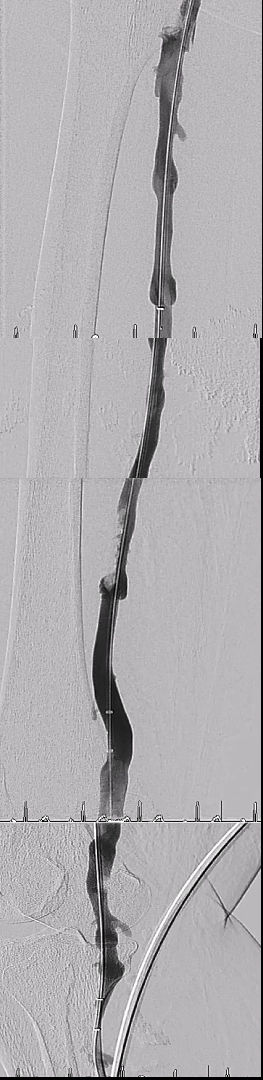
We tried retrograde approach from left femoral vein with long sheath cross over to right common iliac vein, but failed to wire cross common femoral vein even with microcatheter support. We then shifted to antegrade approach from right foot IV catheter and wired to greater saphenous vein successfully and wired back to right external iliac vein. We retrieved the antegrade wire with Snare at common iliac vein and performed externalization for wire fixation. With the antegrade wire guidance, we successfully wired to popliteal vein through common femoral vein; retrograde venogram showed diffuse thrombus with near total occlusion all along femoral vein. We then performed aspiration thrombectomy from popliteal vein to external iliac vein with AngioJet, and thrombus burden decreased a lot; some residual thrombus still noted at femoral vein and iliac vein, and acute on chronic thrombotic event was suspected. Due to residual chronic thrombus with stenosis, we placed two self-expanding bare metal stents from common femoral vein to external iliac vein with good final flow.
Case Summary
In this case, without antegrade wire guidance we cannot found the route of common femoral vein. Switching antegrade or retrograde approach is essential when difficult finding the route, and antegrade venous approach at distal peripheral limbs showed good accessibility and easy for hemostasis. AngioJet thrombectomy showed an optimal result of eliminating thrombosis at femoral vein.