
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-025
Coronary Wire TPM in Rescue PCI
By Suhashni Gnaneswaran, Seong Kooi Khaw, Houng Bang Liew
Presenter
Suhashni Gnaneswaran
Authors
Suhashni Gnaneswaran1, Seong Kooi Khaw1, Houng Bang Liew2
Affiliation
Hospital Queen Elizabeth II, Malaysia1, Queen Elizabeth II Hospital, Malaysia2,
View Study Report
TCTAP C-025
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Coronary Wire TPM in Rescue PCI
Suhashni Gnaneswaran1, Seong Kooi Khaw1, Houng Bang Liew2
Hospital Queen Elizabeth II, Malaysia1, Queen Elizabeth II Hospital, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Mr IH
Relevant Clinical History and Physical Exam
Mr IH is a 66 years old fit gentleman with no known medical illness.
He is a chronic smoker.
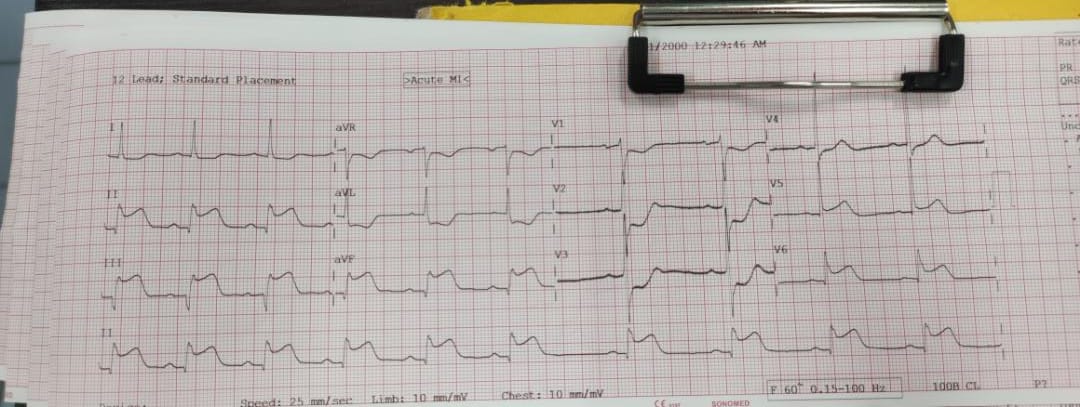
He presented to a district hospital with Inferior STEMI.He was given lytic therapy. However post lytic noted to have persistent ST elevation at the inferior leads and ongoing chest pain.
Heart Rate 66bpm Blood Pressure 111/90.
Cardiovascular examination was unremarkable and lungs were clear.
He was subsequently transferred to our centre for rescue PCI.
Relevant Test Results Prior to Catheterization
ECG was noted ST elevation at infero-lateral leads with reciprocal changes at 1 and aVL.
Relevant Catheterization Findings
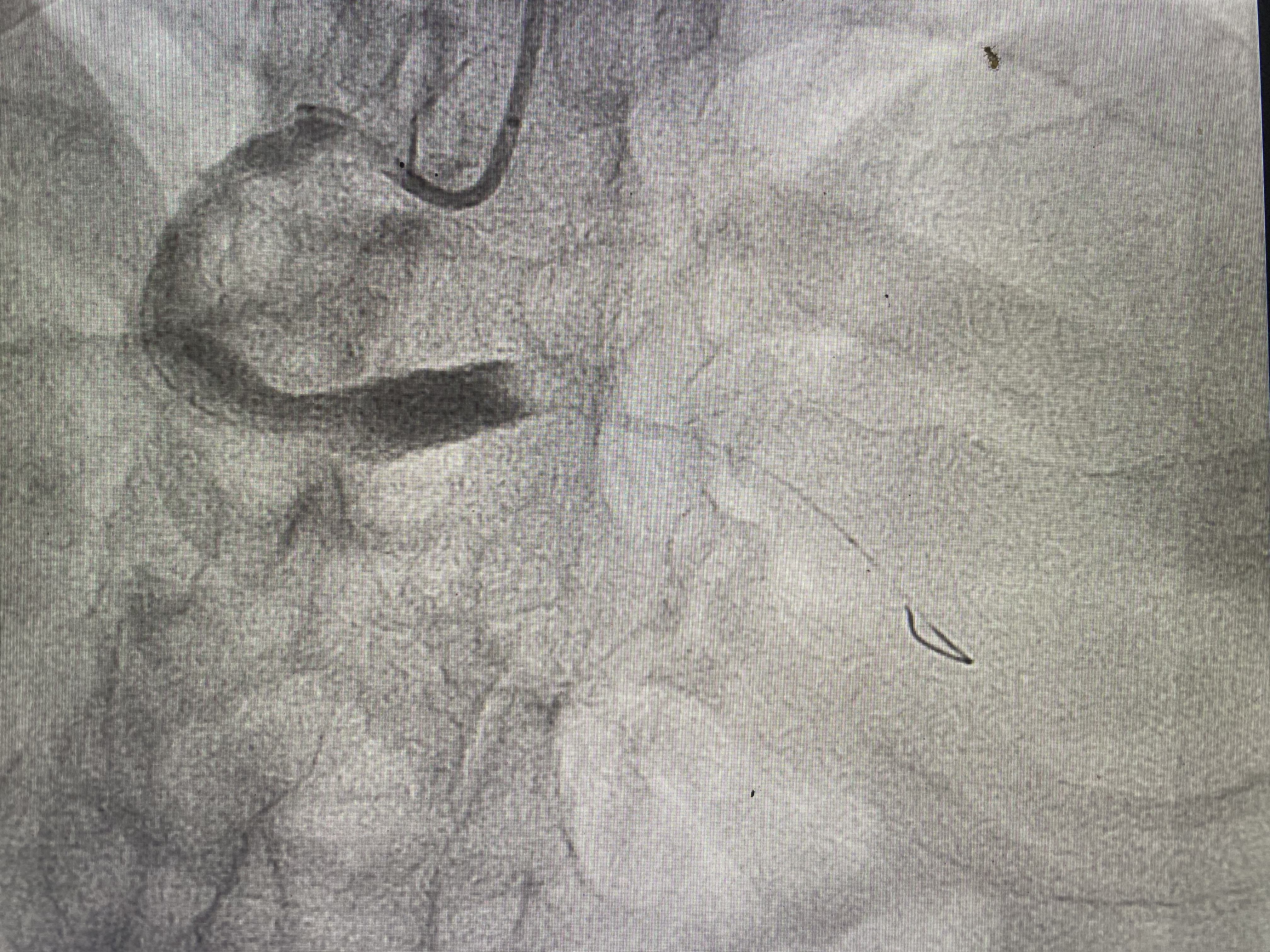
The angiogram revealed single vessel disease and the RCA was the infarct related artery.RCA was large and dominant with distal occlusion.Post PCI results revealed TIMI 3 flow.


Interventional Management
Procedural Step
RCA was engaged with a JR4 guiding catheter and a BMW wire was passed to the RCA. A semi-compliant 3.0x15 mm balloon was dottered through the RCA. Post dottering, TIMI 1-2 flow was established. However a large thrombus was noted at the distal RCA.Hence, decision was made for mechanical thrombectomy with angiojet system.After the first run of angiojet, patient became bradycardic, HR drop to 30-40, cardiac monitor showed complete heart block.


Patient was asymptomatic.
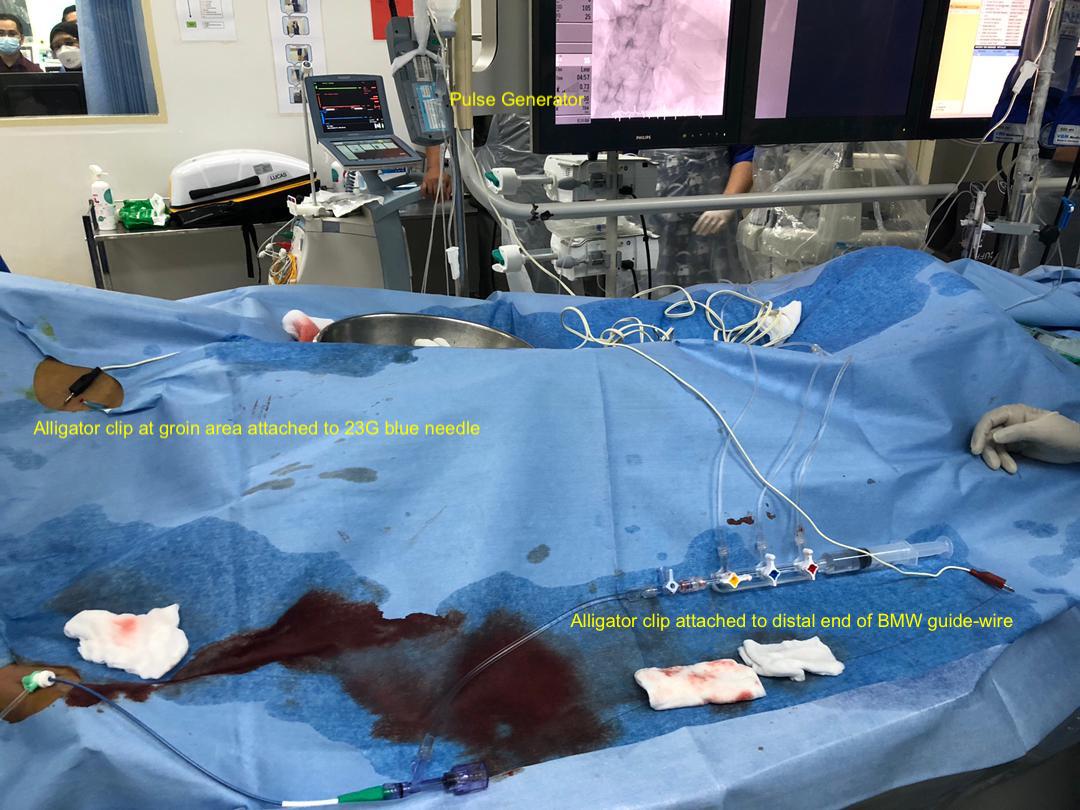
We immediately proceeded with temporary pacing via coronary guide-wire.
A 23-gauge needle was inserted at the subcutaneous tissue of patient's right groin with one of the sterile alligator clips attached to it.
A scalpel was used to scrape the distal end of the BMW guide wire to expose the metal of the guide-wire and the remaining alligator clip is attached to it. The electrodes were then attached to a pulse generator with output 5mV and rate 60bpm.Cardiac monitor revealed paced rhythm.
We then proceeded with another two runs of angiojet and subsequently TIMI-3 flow was established.
Patient remained chest pain free and blood pressure and heart rate was maintained post procedure.
Patient was admitted to the coronary care unit for five days and was started on anticoagulation and DAPT.
He was discharged well with DAPT regime for one year and an exercise stress test was successfully performed at 6 months follow up.
Case Summary
In a case where conduction block develops during PCI, temporary guide wire pacing is reliable and easily performed and should be considered as an alternative to theseparate placement of a transvenous temporary pacemaker.It is cost friendly and avoids additional venous puncture under hemodynamically unstable conditions and also avoids an insertion of a transvenous pacing which can lead to potentially severe complications.