
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-036
Combined Use of Rotational Atherectomy and Intra-Vascular Shockwave Lithotripsy in Heavily Calcified Lesion
By Wai Lun Mak, Yue Hong Cheng, Chi Wing Wong
Presenter
Wai Lun Mak
Authors
Wai Lun Mak1, Yue Hong Cheng1, Chi Wing Wong1
Affiliation
Pok Oi Hospital, Hong Kong, China1,
View Study Report
TCTAP C-036
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Combined Use of Rotational Atherectomy and Intra-Vascular Shockwave Lithotripsy in Heavily Calcified Lesion
Wai Lun Mak1, Yue Hong Cheng1, Chi Wing Wong1
Pok Oi Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
YKC
Relevant Clinical History and Physical Exam
75 year old man with diabetes, hypertension, hyperlipidaemia, end-stage renal failure on dialysis was admitted for NSTE-ACS. He presented with chest pain for 2 days. Physical exam revealed clear chest, dual heart sound with no murmur, no lower limb edema. JVP was not elevated.
Relevant Test Results Prior to Catheterization
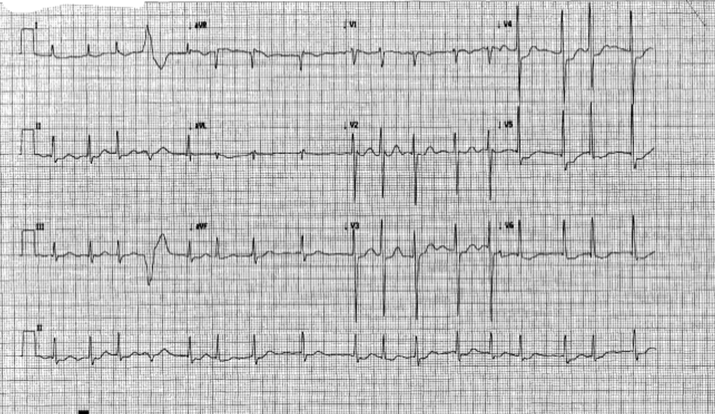
ECG showed ST depression on lateral leads. Troponin was elevated from 571 to 10956 ng/L (Normal: <34). Echo showed mildly impaired LV systolic function with LVEF 46% . Hypokinesia was observed over basal inferolateral wall and apex.
Relevant Catheterization Findings
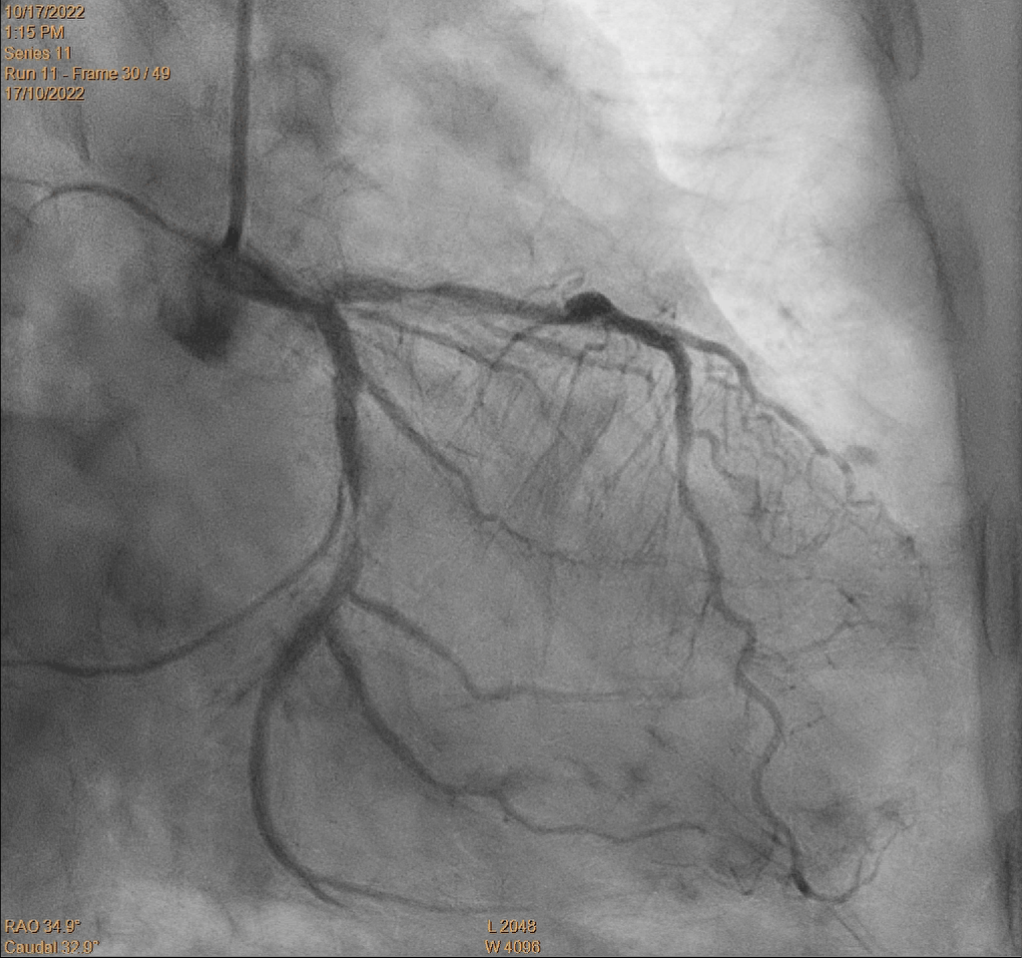
Left main: Moderate disease
Interventional Management
Procedural Step
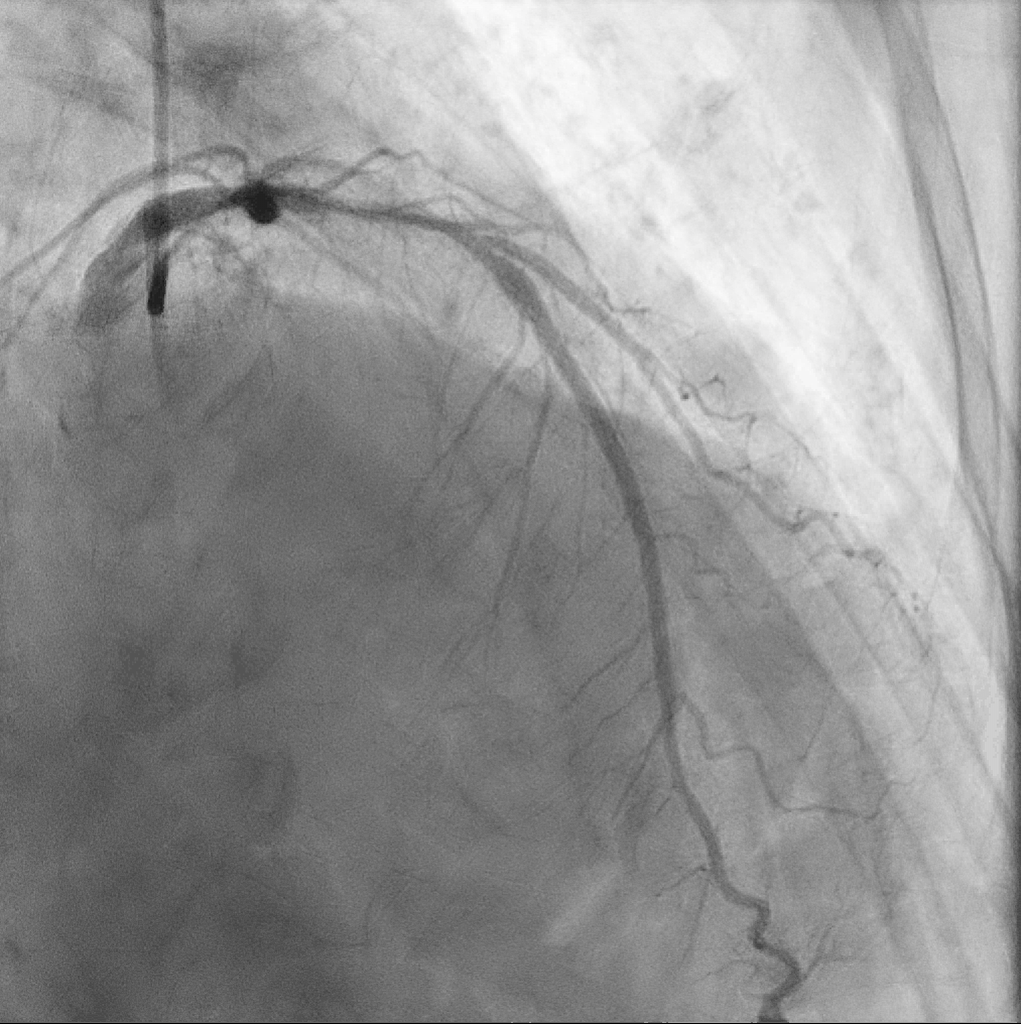
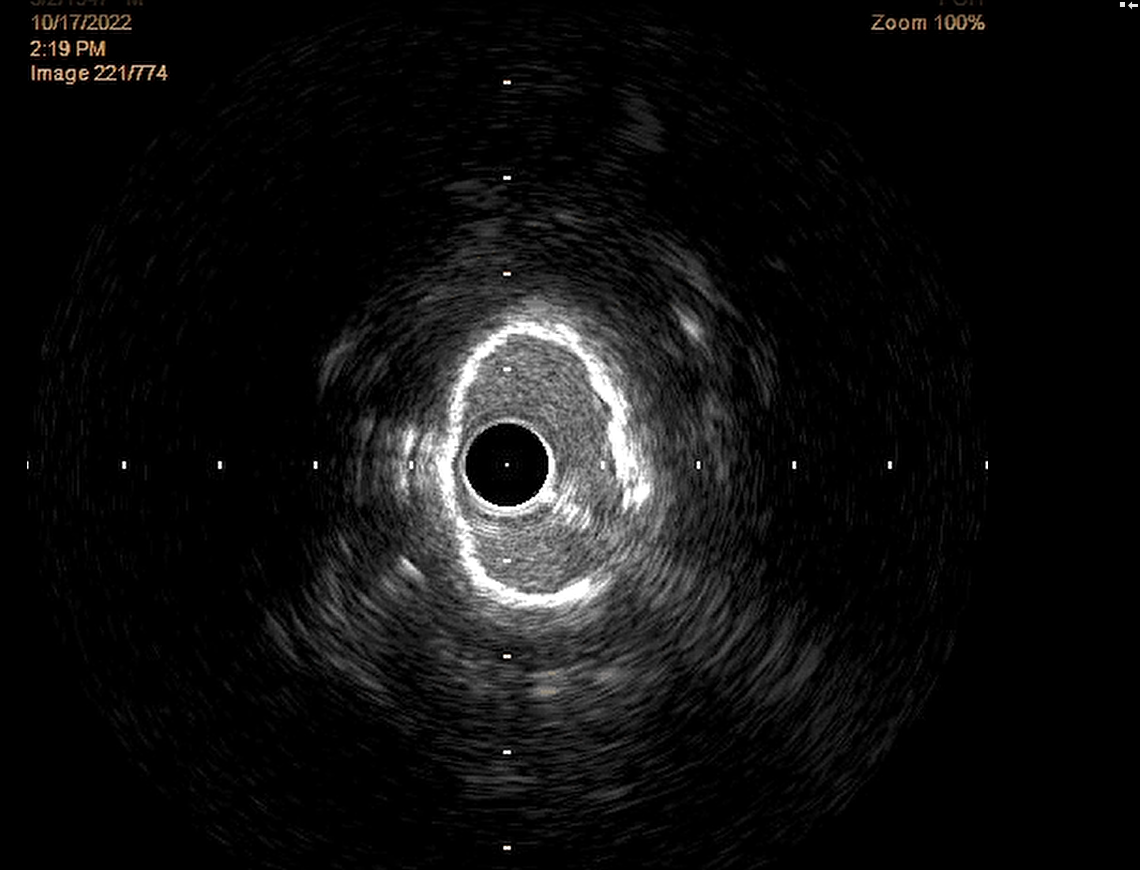
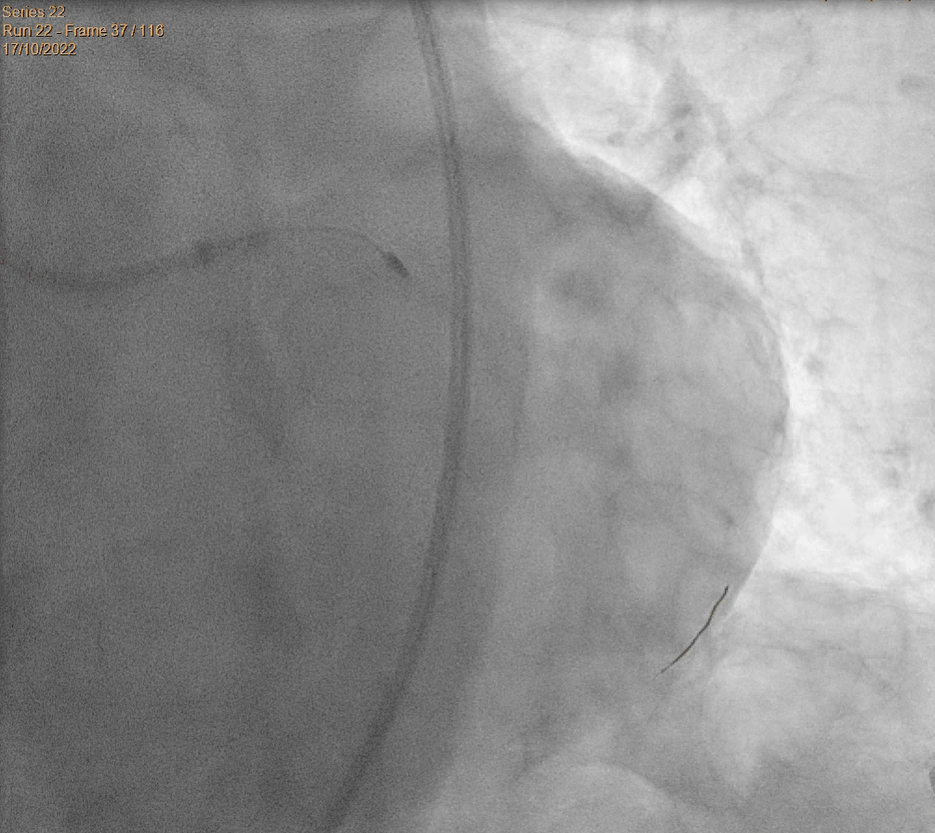
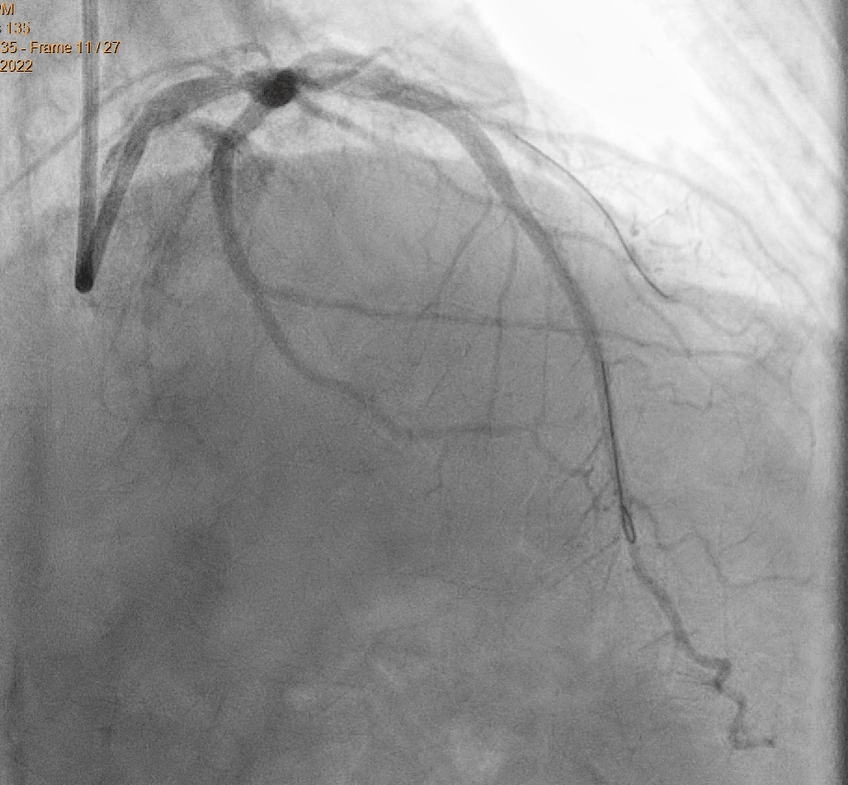
Left main engaged with EBU 3.5 7F guiding catheter. We initially failed to cross the lesion with Runthrough wire to LCx, but eventually wired with Fielder XTA. IVUS assessment showed circumferential calcium from p-mLCx. mLCx was pre-dilated with NC sapphire 3.0/15 at 18atm. Fielder wire was exchanged with Rotawire Floppy with use of Turnpike LP microcatheter. Rotablation was done with 1.5mm burr over p-mLCx at 160k-170krpm. Patient developed transient hypotension and required transient norepinephrine/dopamine support. Lesion was further prepared with Shockwave 3.5/12 over p-mLCx at 4-6atm for 3 therapies. Post-IVUS showed cracked calcium over pLCx but calcium remains uncracked over mLCx, which was further optimised with NC sapphire 3.5/15 and NC Scoreflex 2.5/15 over p-mLCx at 12-16atm. The p-mLCx lesion was stented with Ultimaster 2.75/28 and Ultimaster 3.5/33 at 8-11atm. Accuforce 2.75/15 was deployed at 9-22atm for stent optimisation. Repeated IVUS assessment showed well expanded stent with no edge dissection. Similar technique was repeated to treat the o-mLAD lesion. The o-mLAD lesion was eventually stented with Ultimaster 2.75/28 and Ultimaster 3.5/33 at 8-12atm. TIMI 3 flow achieved.

Case Summary
Good lesion preparation is a pre-requisite for optimal stenting and therefore long term clinical outcome. Combined lesion preparation with rotational atherectomy and intravascular lithotripsy may be a feasible option in lesion preparation.