
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-189
A Challenging Case Report: Transcatheter Occulsion One Coronary Artery Fistula From Right Coronary Artery to Left Ventricule
By Chen-Yu Wu, Yu-Jen Wei, Cheng-Han Lee, Jieh-Neng Wang
Presenter
Chen-Yu Wu
Authors
Chen-Yu Wu1, Yu-Jen Wei1, Cheng-Han Lee2, Jieh-Neng Wang1
Affiliation
National Cheng Kung University Hospital, Taiwan1, Tainan Municipal Hospital, Taiwan2,
View Study Report
TCTAP C-189
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
A Challenging Case Report: Transcatheter Occulsion One Coronary Artery Fistula From Right Coronary Artery to Left Ventricule
Chen-Yu Wu1, Yu-Jen Wei1, Cheng-Han Lee2, Jieh-Neng Wang1
National Cheng Kung University Hospital, Taiwan1, Tainan Municipal Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
21094542
Relevant Clinical History and Physical Exam
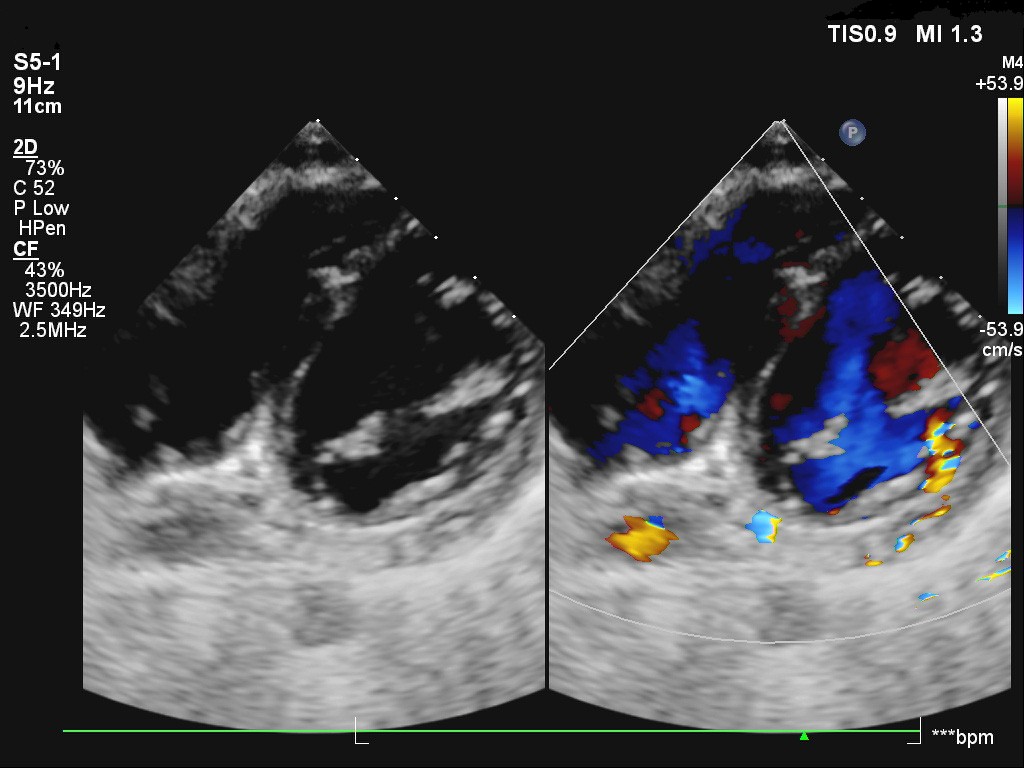
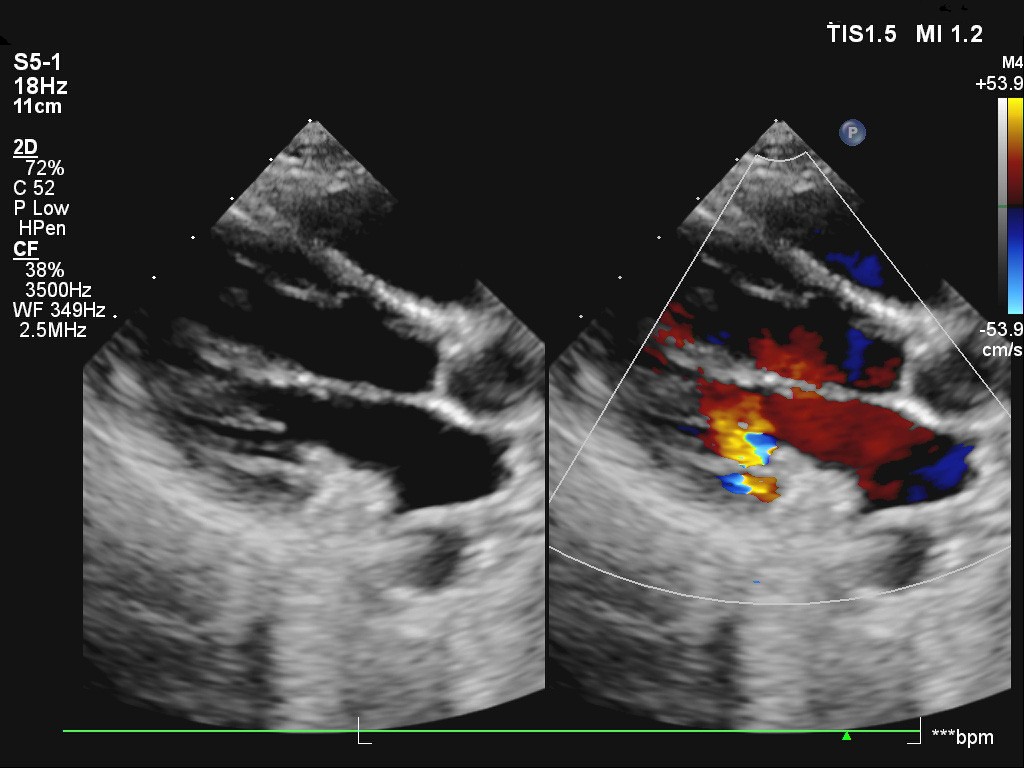
A 12-year-old boy was admitted with frequent syncope episodes up to 2-3 times per day and sudden fall down with loss of consciousness for 2 minutes. He also complained about chest tightness. Physical examination was notable for a grade II/VI early systolic murmur at left sternal border. Echocardiography revealed right proximal coronary artery(RCA) dilation with z-score +3.11, one coronary artery fistula from RCA to left ventricule (LV) just below mitral valve.
Relevant Test Results Prior to Catheterization
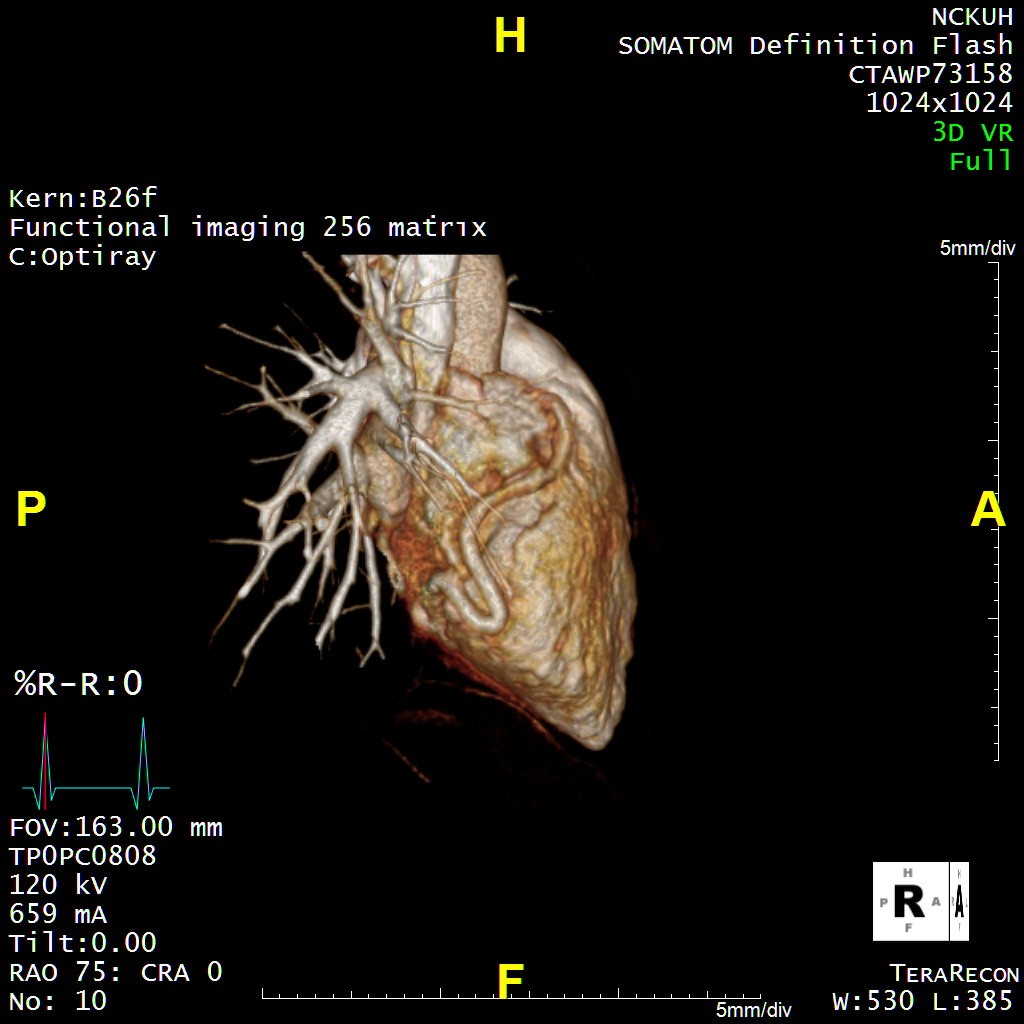
Electrocardiogram showed sinus rhythm without ST-T change. The 3D computed tomography angiography revealed a coronary fistula from the dilated and tortuous RCA to LV blood pool.
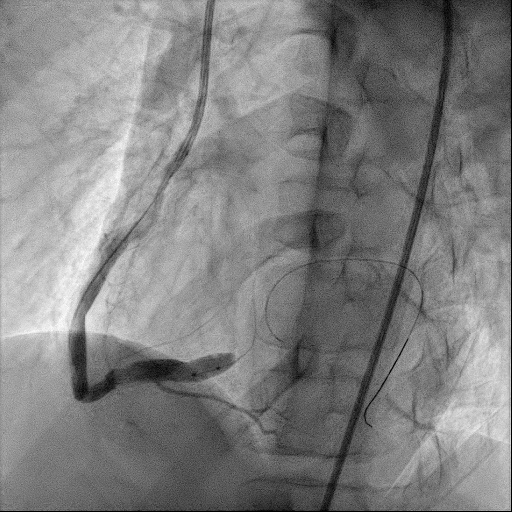
Relevant Catheterization Findings
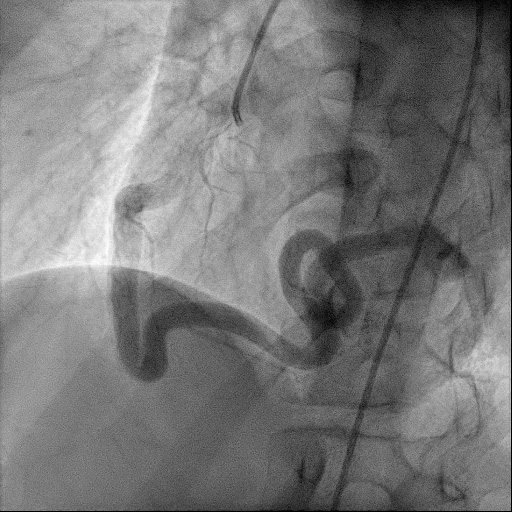
Coronary angiography revealed patent left main artey with relative small diameter. A large and tortuous coronary artery fistula from RCA drainage to LV size with size around 5.66-6.16 mm. After balloon occulsion test revealed RCA branching from the fistula at the proximal site.
Interventional Management
Procedural Step
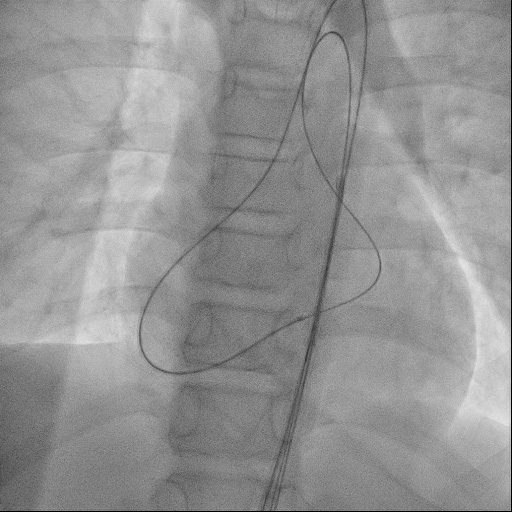
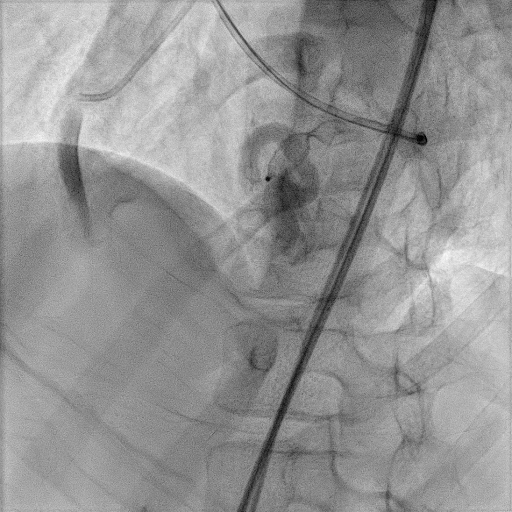
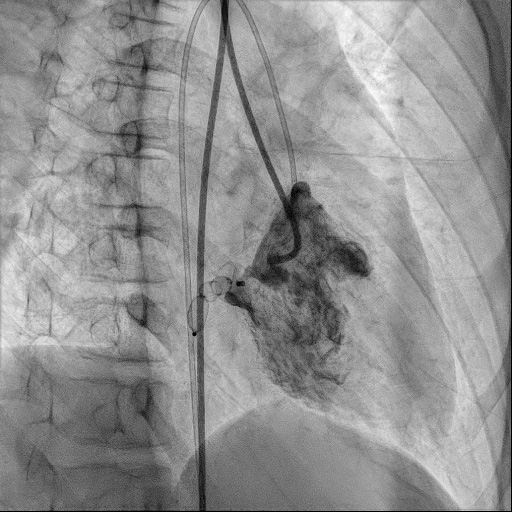
Under general anesthesia, we set up a 6Fr Merit sheath from right femoral artery. We put a 6F JR catheter at RCA orifice. A PTCA Guide wire was advanced from right coronary artery to LV with Guiding Extension Catheter support. We used a Emerge NC balloon 6.0mmx8mm for occlusion test at proximal site of this coronary fistula. However, posterior descending artery was arise from this fistula. We then advanced this PTCA Guide wire to aorta with a CXI Support catheter support. We then exchanged the PTCA Guide wire to a 0.035 Terumo guide wire. Another 6Fr JR catheter was put to aorta. We snared this 0.035 Terumo guide wire down to descending Ao. A 6Fr JR4 guiding catheter was used for occluder delivery. An Amplatzer vascular plug II 12 mm was used to occlude this coronary fistula smoothly. RCA and LV angiogram showed no residual shunt after occlusion.
Case Summary
We describe a rare case of coronary artery fistula from RCA to LV. Due to this coronary artery fistula was very tortuous, we tried to close this coronary artery fistula at proximal portion, initially. However, under occlusion test, there was still some RCA branches arise from this fistula. We finally created an A-A loop and successful used vascular Plug II from the distal site to occlude this fistula.