
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-102
The Separation of Two Coronary Artery by an Unexpected Complication: Coronary Perforation Successfully Managed by Retrograde and Antegrade Gelfoam Injection
By Hsuan-Ling Tseng, Kuang-Te Wang
Presenter
Hsuan-Ling Tseng
Authors
Hsuan-Ling Tseng1, Kuang-Te Wang2
Affiliation
Chi-Mei Hospital, Taiwan1, Mackay Memorial Hospital, Taiwan2,
View Study Report
TCTAP C-102
CORONARY - Complications (Coronary)
The Separation of Two Coronary Artery by an Unexpected Complication: Coronary Perforation Successfully Managed by Retrograde and Antegrade Gelfoam Injection
Hsuan-Ling Tseng1, Kuang-Te Wang2
Chi-Mei Hospital, Taiwan1, Mackay Memorial Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
CKH
Relevant Clinical History and Physical Exam
This 87 y/o man had suffered from intermittent chest pain for one month. He was a case of 1. sick sinus syndrome s/p PPM; 2. hypertension; 3. hyperlipidemia; 4. chronic kidney disease. Physical examination showed clear breathing sound, regular heartbeat with grade 2/6 systolic murmur over left lower sternal border and apex, and no pitting edema.
Relevant Test Results Prior to Catheterization
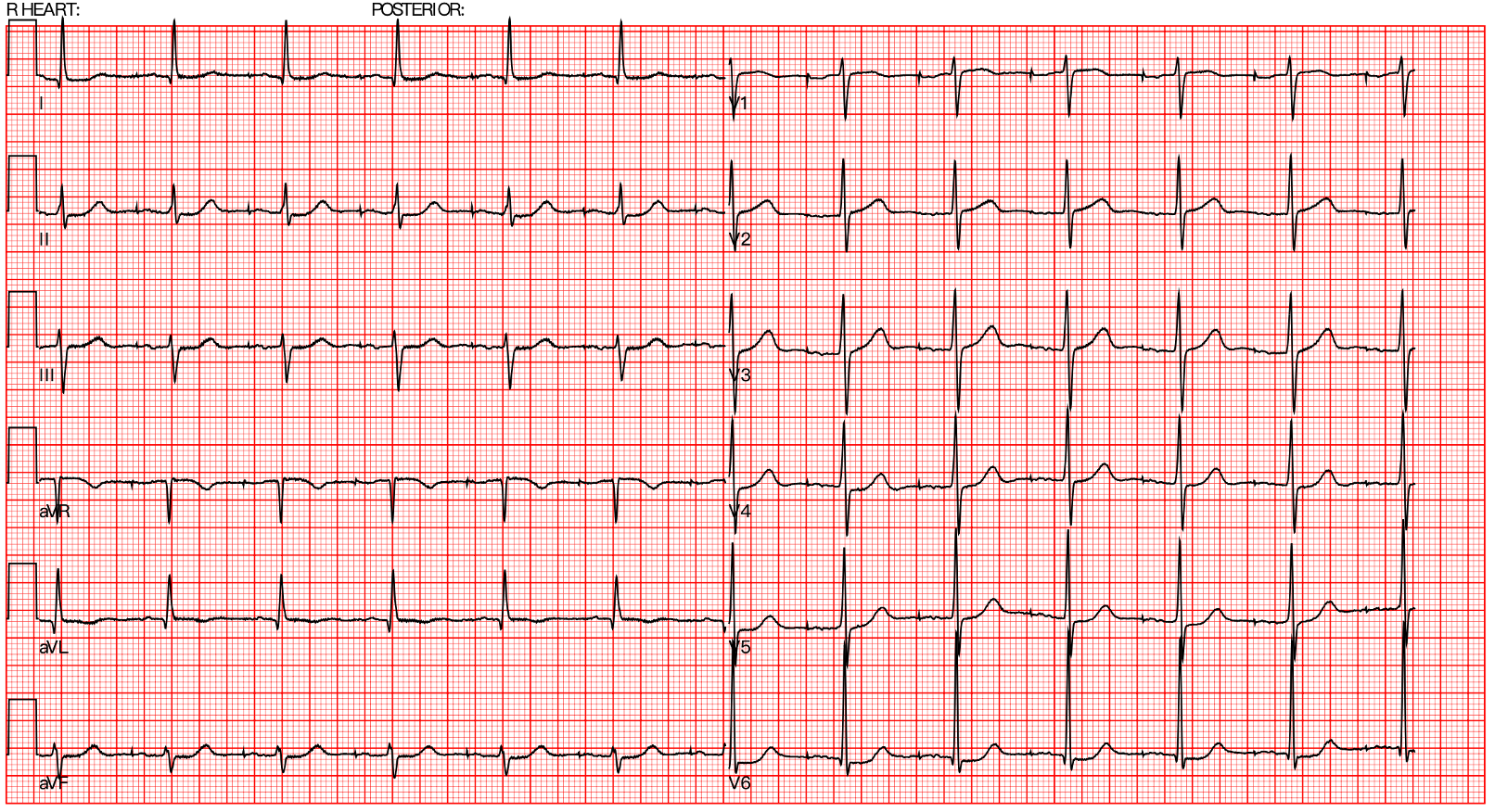
ECG showed pacemaker rhythm without ST segment change but Q wave at lead I and aVL. Lab data showed no leukocytosis but mild anemia. BUN/Cr was 28.5/1.95.
Relevant Catheterization Findings
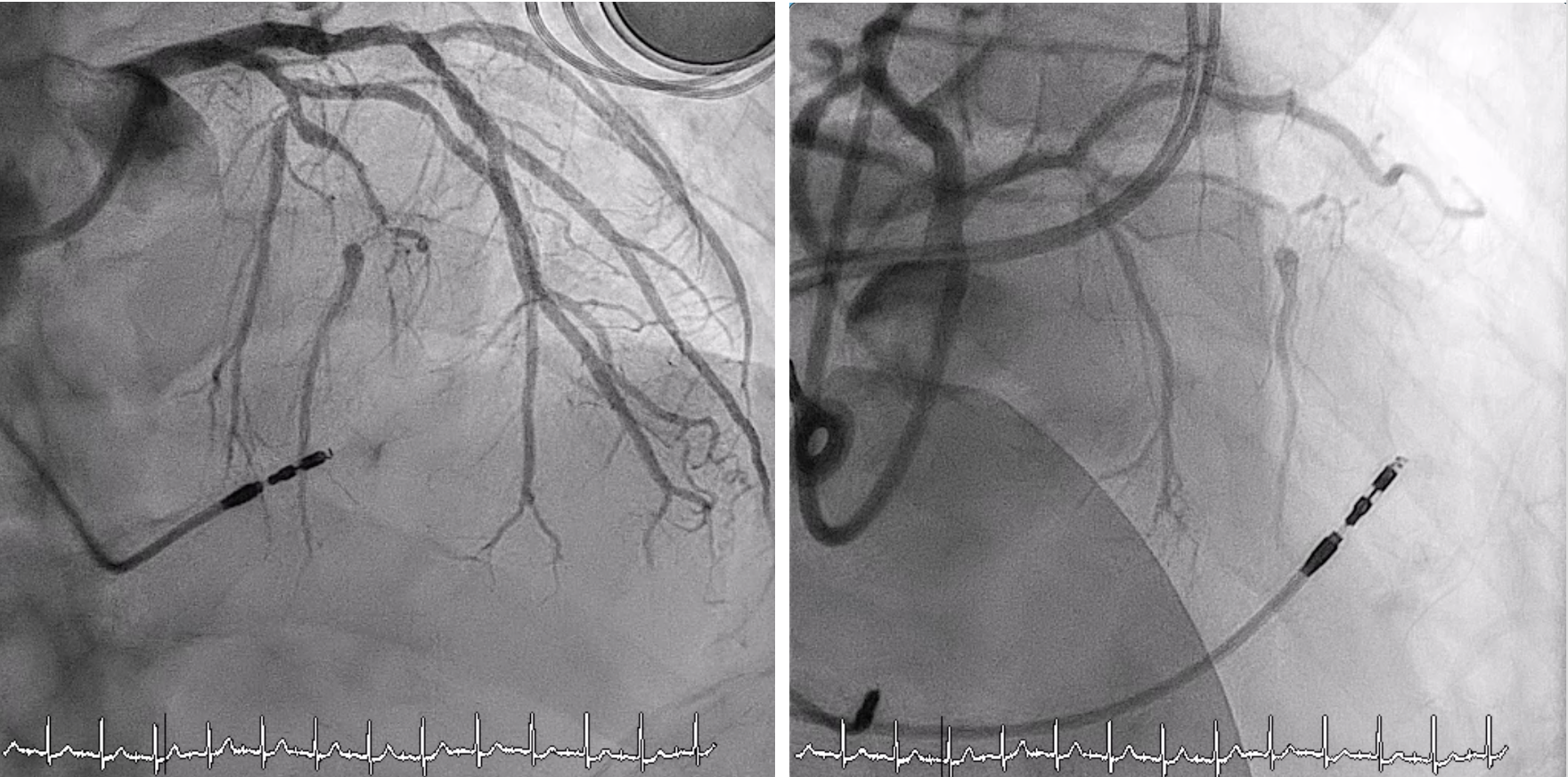
CAD, 2-V-D,LAD-M: 100% stenosisLCX-D: 70% stenosis
Collateral channel:LAD bridgingLCX-OM to LADRCA to LAD
Syntax score: 24J-CTO score: 1(Blunt)
Collateral channel:LAD bridgingLCX-OM to LADRCA to LAD
Syntax score: 24J-CTO score: 1(Blunt)
Interventional Management
Procedural Step
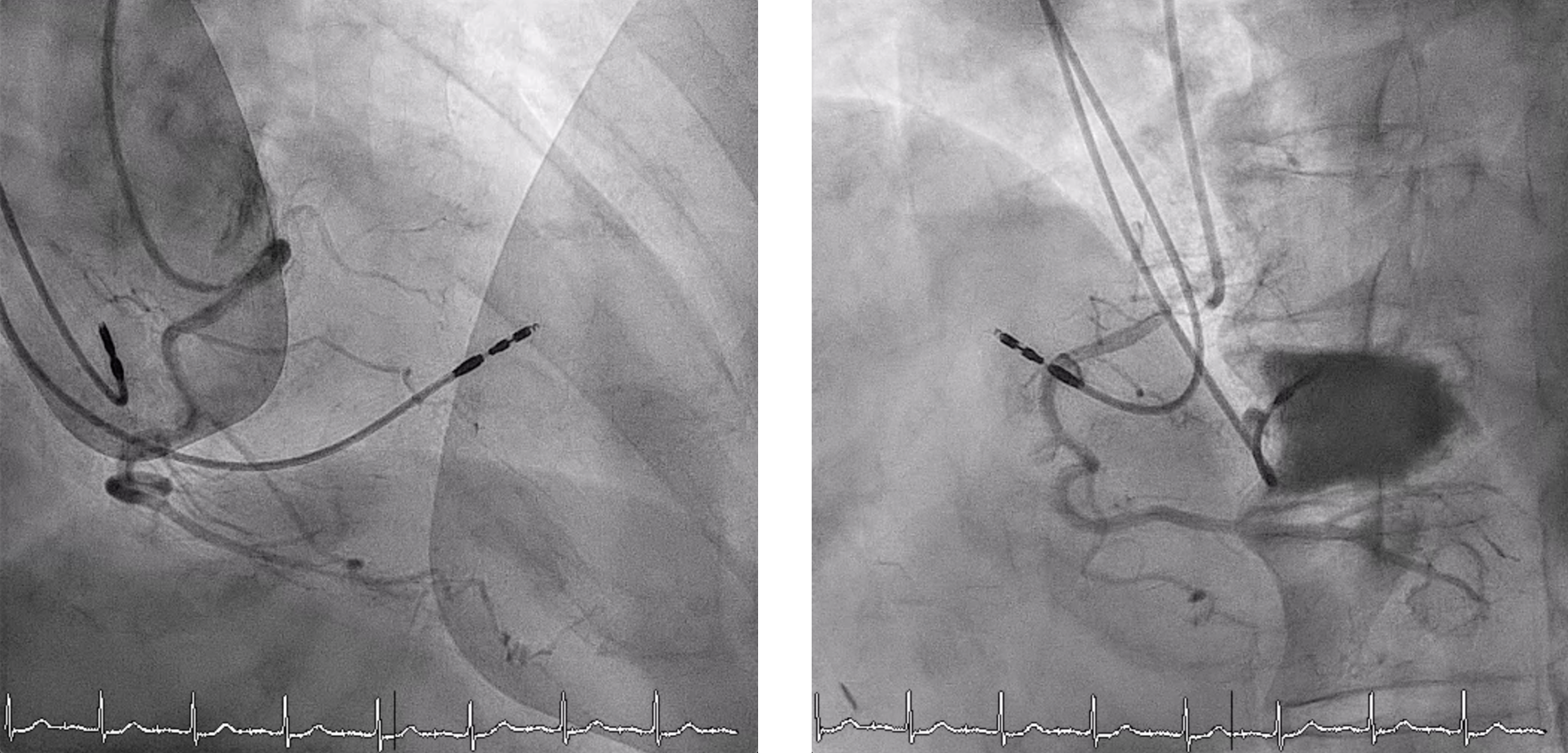
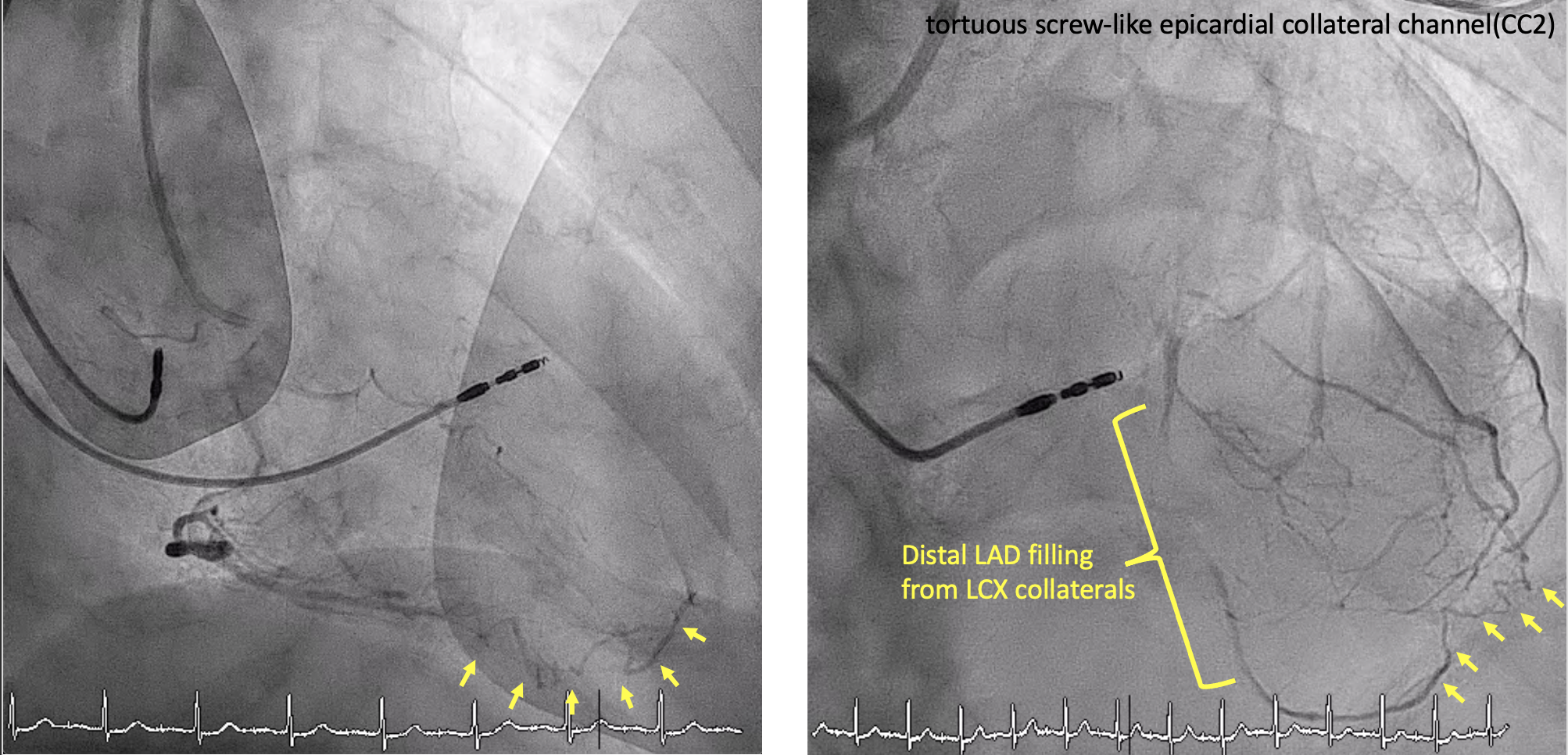
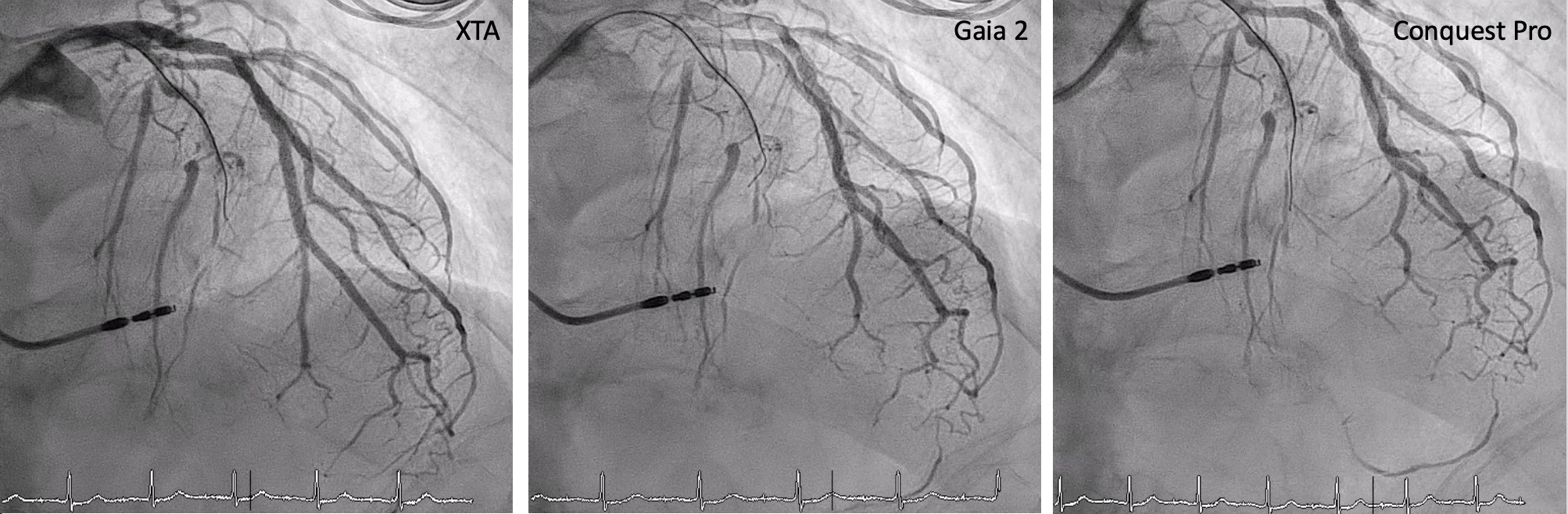
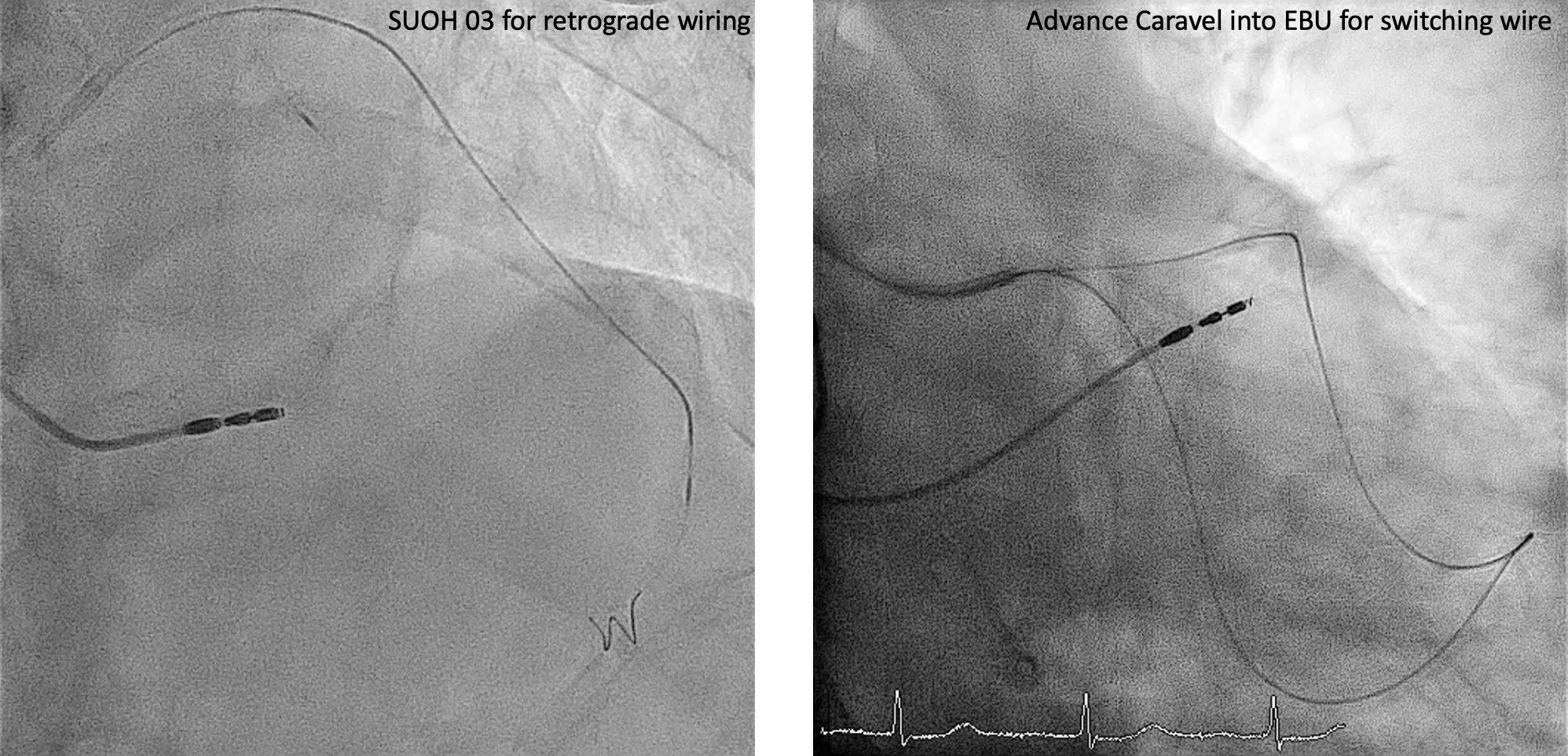
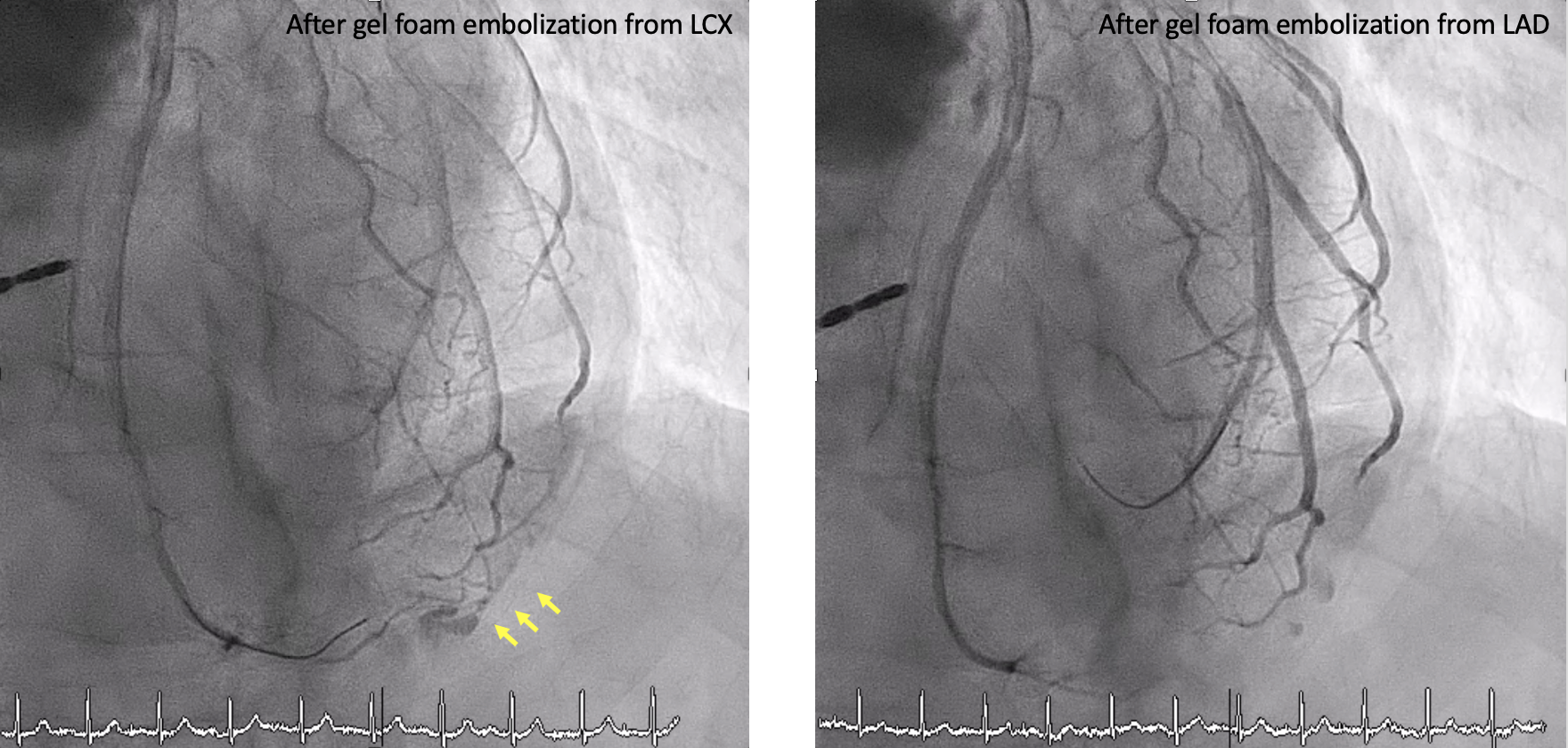
The initial strategy was antegrade wire escalation for LAD CTO lesion. We used Asahi XTR with microcatheter Caravel 135cm under 7-Fr EBU 3.5 guiding catheter. XTR easily went into the side branch and the wire was shifted to XTA. Then we tried Gaia 2 and Conquest Pro but all in vain. Due to failed antegrade wiring, the strategy was shifted to retrograde collateral wiring. We used Run-through NS with microcatheter Caravel 150cm by epicardial collateral approach through LCX-OM. Due to a very tortuous collateral channel, we switched the wire to SUOH 03. The SUOH 03 wire went into the true lumen luckily. Then we changed the wire with Run-through NS and advanced it into EBU guiding. We further advanced the caravel catheter into EBU for switching wire. We switched the wire to RG3 for externalization. We used small balloons (1.0 & 1.25) for pre-dilatation. Then we removed RG3 with the microcatheter and exchanged wire with Run-through NS. We use 2.0 and 2.5 balloons for pre-dilatation. We deployed DES 2.5 x 48mm and 3.0 x 48mm. We used an NC balloon for post-dilatation. However, the angiography showed extravasation at the epicardial collateral channel. Hemodynamic status was stable and the patient denied chest pain. Echocardiography showed no pericardial effusion. We used balloon inflation for 5 minutes twice from LCX-OM and LAD-D but in vain. We performed gelfoam embolization by microcatheter both anterogradely and retrogradely. The final result showed no further extravasation.
Case Summary
1. Epicardial collateral vessels tend to be small and tortuous, with a high risk for uncontained perforation resulting in hemodynamic compromise. They are typically the access route of last resort.2. The collateral perforation can originate from both antegrade and retrograde; therefore, if you treat one, don't forget the other.3. SUOH 03 guidewire allows much smoother and softer channel navigation and provides superb trackability and crossability in severely tortuous vessels.