
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-138
A Challenging Case Report: Intracoronary Streptokinase for Mitragyna Speciosa Associated Large Thrombus
By Wongsaput Boonyakiatwattana
Presenter
Wongsaput Boonyakiatwattana
Authors
Wongsaput Boonyakiatwattana1
Affiliation
Chulabhorn Hospital, Thailand1,
View Study Report
TCTAP C-138
CORONARY - Pharmacology/Pharmacotherapy
A Challenging Case Report: Intracoronary Streptokinase for Mitragyna Speciosa Associated Large Thrombus
Wongsaput Boonyakiatwattana1
Chulabhorn Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
496780
Relevant Clinical History and Physical Exam
A 35-year-old man was presented with persistent retrosternal chest pain for 3 hours prior to admission.The patient had no risk factor except chronic use Mitragyna Speciosa for 1 year.Blood pressure of 138/64 mm Hg and heart rate of 68 beats/minute were recorded at the time of admission. At presentation, Killip class II was recorded.
Relevant Test Results Prior to Catheterization
ECG showed ST segment elevation in II, III, aVF and V1. Troponin I level was 4.6 mcg/L (normal value: <0.03 mcg/L), and other laboratory data were unremarkable.
Relevant Catheterization Findings
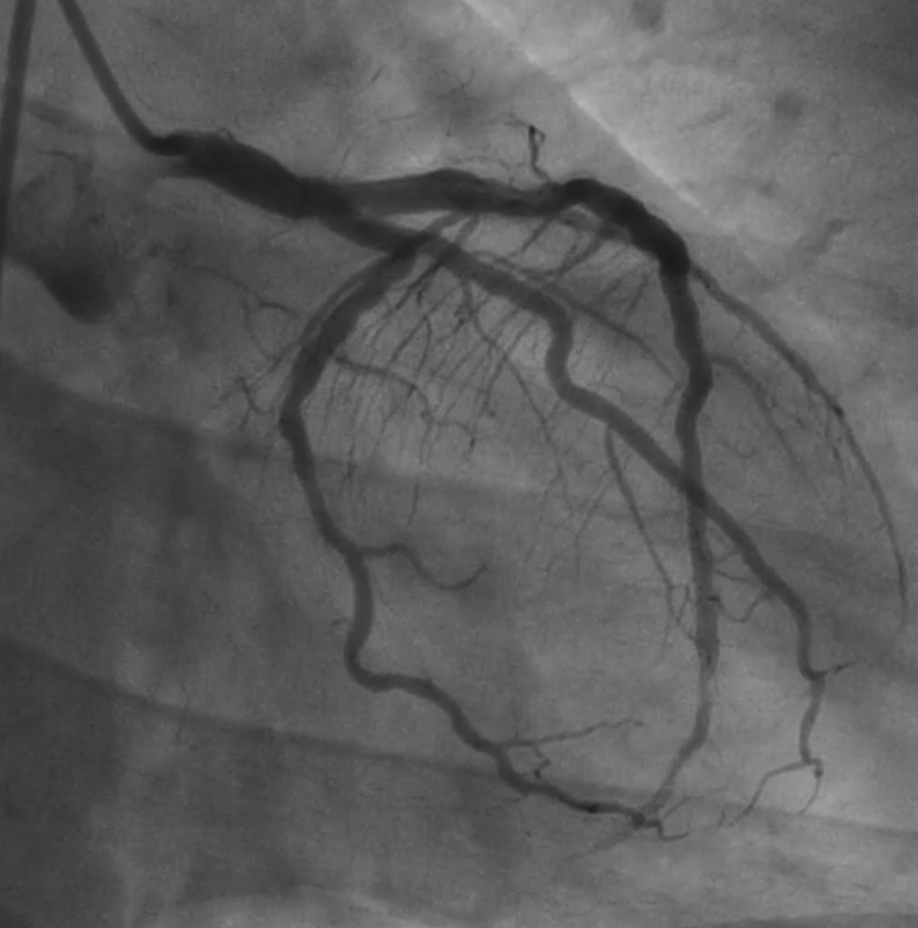
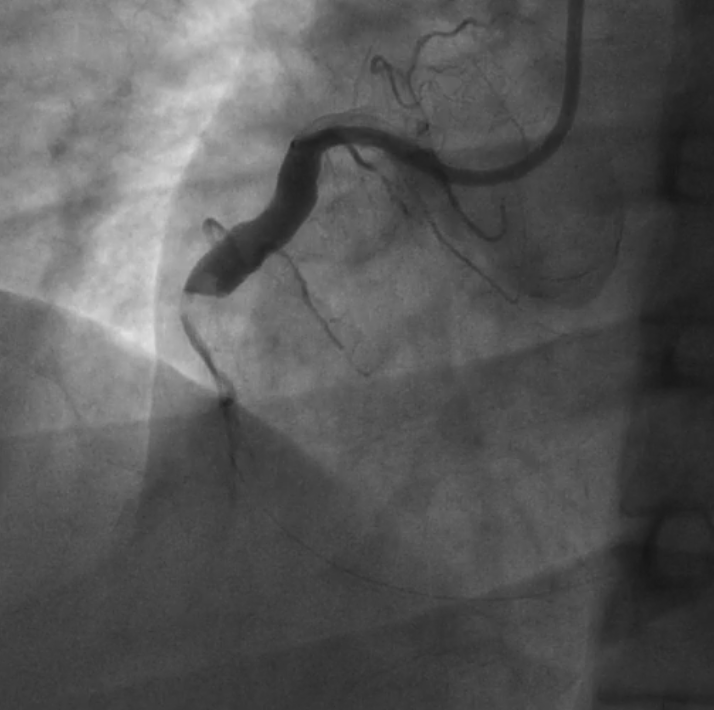
Coronary angiography via the right femoral artery was performed for primary angioplasty, which showed complete thrombotic occlusion of the right coronary artery (Figure A). The left anterior ascending artery was moderate calcified proximal LAD, diffuse mild ectasia with relatively slow flow.The left circumflex was luminal irregularity (Figure B, C).


Interventional Management
Procedural Step
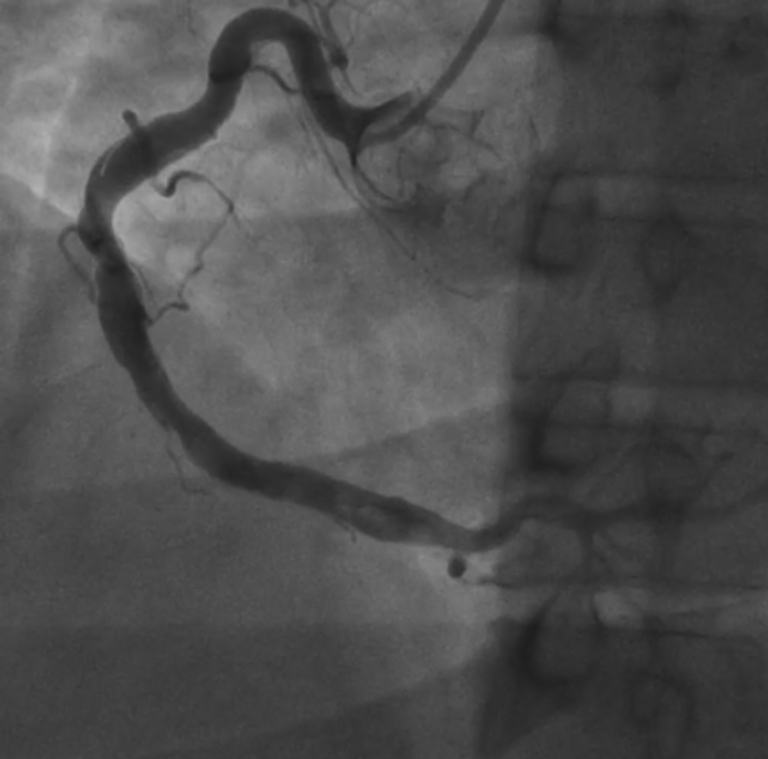
The right coronary artery was primary PCI. 7-Fr Thrombuster II advanced aspiration catheter was done several times, resulting in minimal improvement in RCA artery blood flow with residual large thrombus burden.Bailout intracoronary injection of Eptifibatide injected in two consecutive bolus of 180 mcg/kg each also small plain balloon angiography for thrombus fragmentation failed to improve RCA flow (Figure A). Thus, we decided to try IC thrombolysis. Given that the only available thrombolytic agent was streptokinase, and according to previous studies, using a 250,000 IU of this agent were diluted with 50 mL of 5% dextrose and injected via a thrombo‐aspiration catheter,placed into the proximal portion of the RCA artery, at the rate of 1 ml/minute.Control angiography was performed 15 minutes after the completion of the IC injection of streptokinase, which showed a significant reduction in luminal thrombus burden and TIMI 2 flow of RCA (Figure B) with the patient's chest pain completely relieved and partial resolution of ECG changes.During the hospital stay, the patient was completely asymptomatic and had no bleeding. Subcutaneous enoxaparin was given.Follow‐up angiography was performed 1 week later (Figure C), which showed unmasked previous proximal RCA culprit lesion with partial resolution of the intra‐arterial thrombus.So, we decided to defer stenting and continue use dual-pathway inhibition with rivaroxaban plus P2Y12 inhibitors.

Case Summary
Kratom plant (Mitragyna speciosa) widely used in Southeast Asia is associated with coronary ectasia, microvascular dysfunction and thrombosis.Individualized use of intracoronary fibrinolysis may be usefor bailout setting especially <3 hours of presentation which is associatedwith underlying thrombus pathology (Platelet ++, Fibrin +, Lysis ++).