
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-184
Transcatheter Closure of Post-Bentall Ascending Aortic Pseudoaneurysm Due to Coronary Button Dehiscence
By Huan-Chiu Lin, Wei-Hsian Yin, Yung-Tsai Lee, Tien Ping Tsao
Presenter
Huan-Chiu Lin
Authors
Huan-Chiu Lin1, Wei-Hsian Yin1, Yung-Tsai Lee1, Tien Ping Tsao1
Affiliation
Cheng Hsin General Hospital, Taiwan1,
View Study Report
TCTAP C-184
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
Transcatheter Closure of Post-Bentall Ascending Aortic Pseudoaneurysm Due to Coronary Button Dehiscence
Huan-Chiu Lin1, Wei-Hsian Yin1, Yung-Tsai Lee1, Tien Ping Tsao1
Cheng Hsin General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
D600214
Relevant Clinical History and Physical Exam
A 53-year-oldman with history of hypertension presented with ascending aortic aneurysm andsevere aortic regurgitation underwent Bentall procedure with 26 mm conduit and mechanicalaortic valve in 2021.
Relevant Test Results Prior to Catheterization
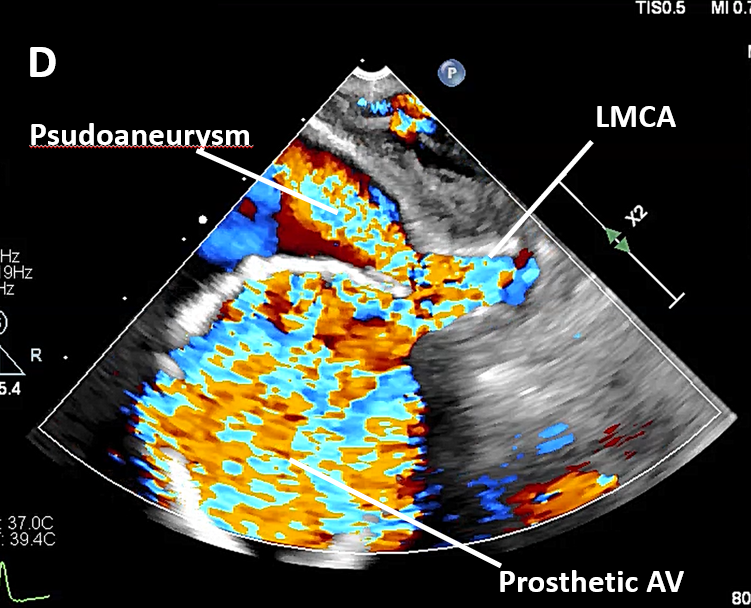
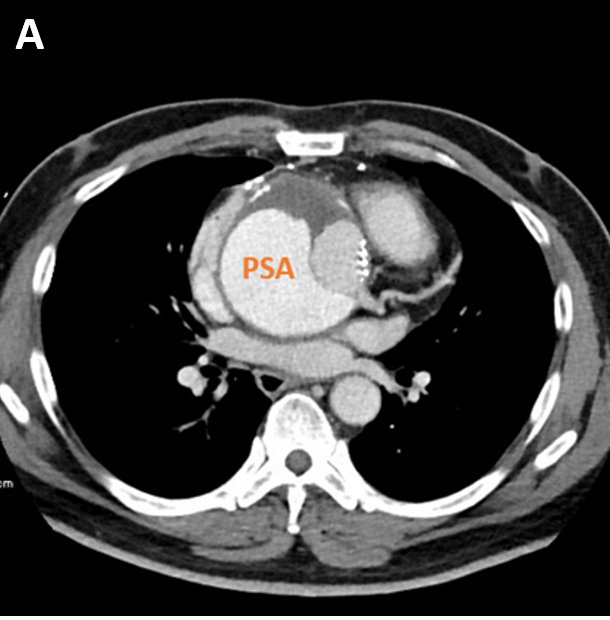
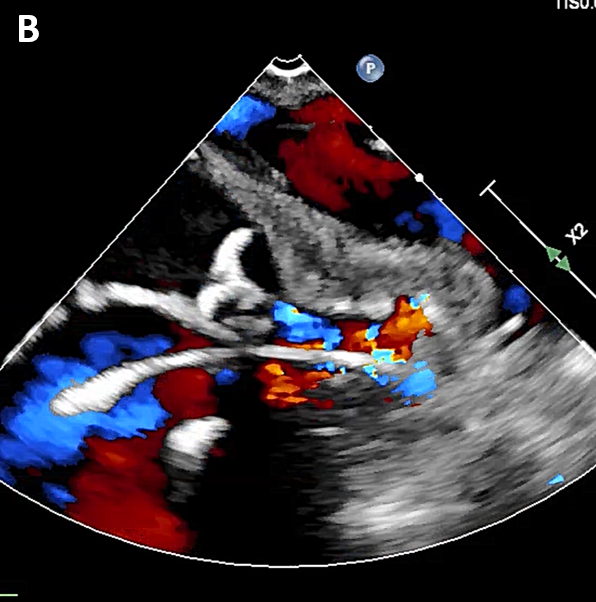
Chestcomputed tomography revealed aortic root pseudoaneurysm, which measured 8.8 x6.4 cm in the mediastinum, with mural thrombus inside. Coronary buttondehiscence with pseudoaneurysm are diagnosed, where the entry point is rightnext to the re-implantation site of left main coronary artery. Transesophagealechocardiography showed a huge pseudoaneurysm right next to the aortic valveprosthesis, connectedwith orifice of left main coronary.
Relevant Catheterization Findings
A hugepseudoaneurysm right next to the aortic valve prosthesis, connectedwith orifice of left main coronary, with systolic pulsatile flow from the aortainto the pseudoaneurysm cavity.
 Video A.AVI
Video A.AVI
Interventional Management
Procedural Step
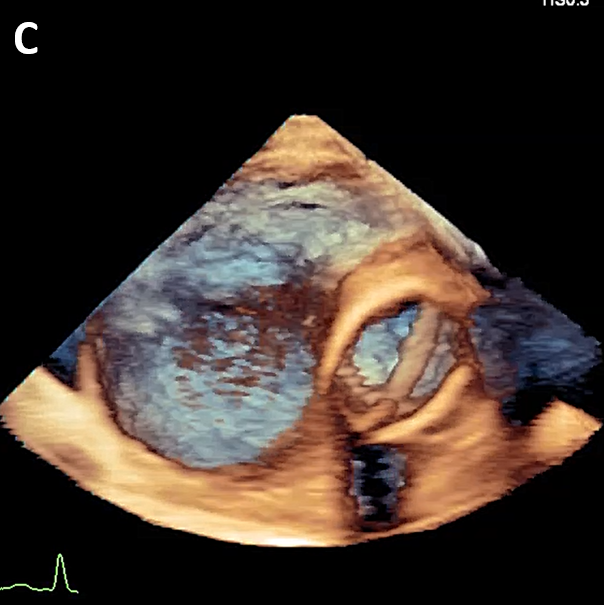
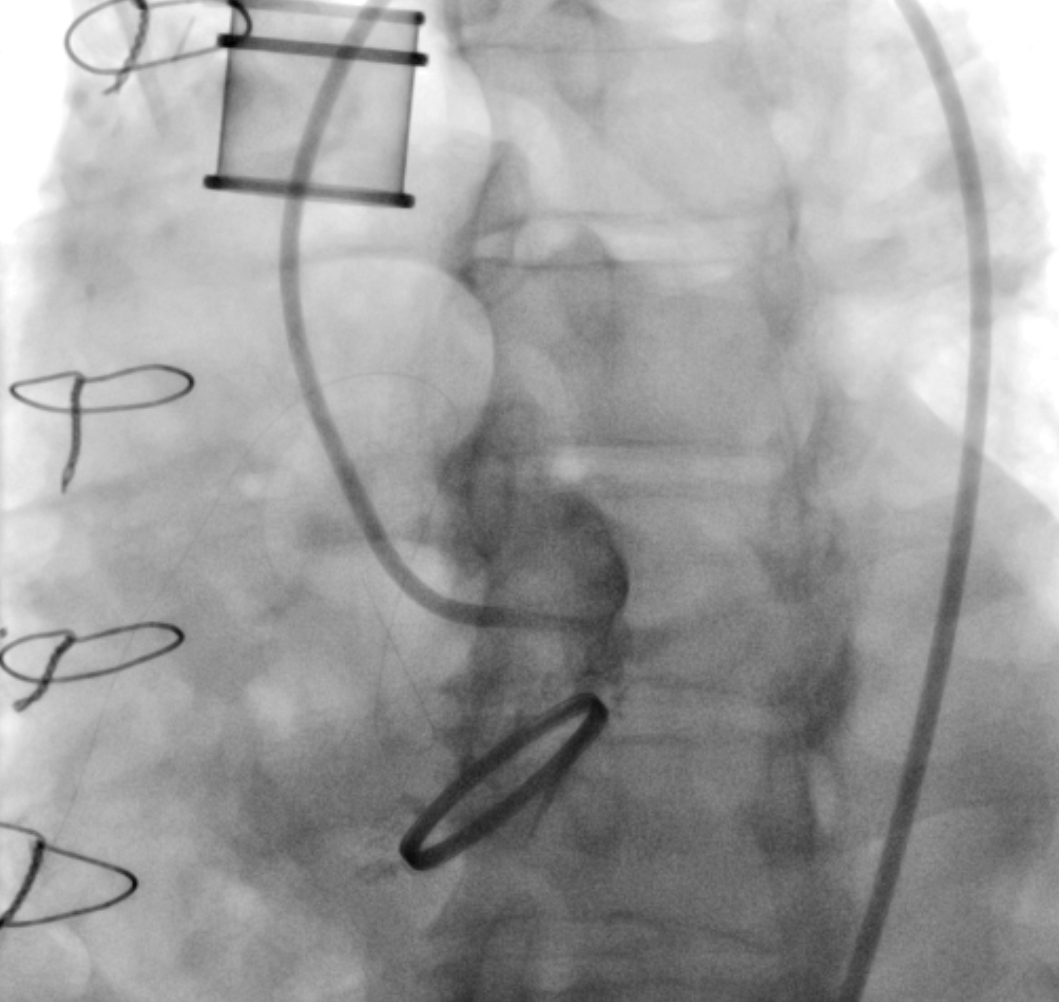
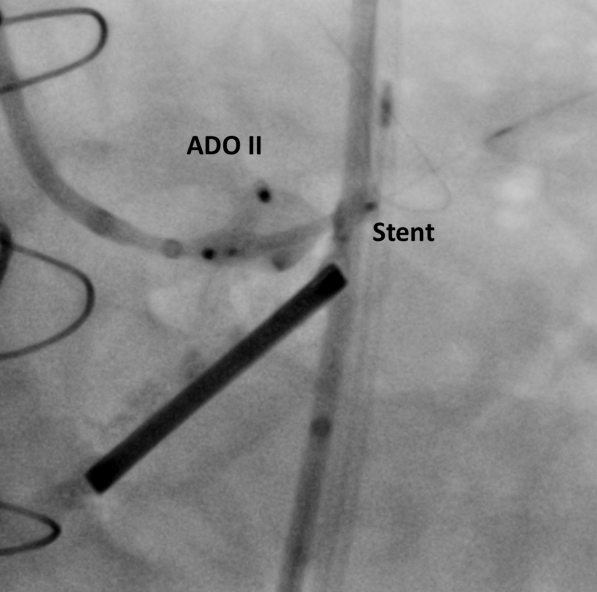
UnderTEE and fluoroscopic guidance, the pseudoaneurysm was selectively engaged with a7F Judkins right coronary guide catheter, followed by passage of two 0.014” coronaryguidewire to increase support, while a second 6F Judkins right guide catheterintroduced through contralateral femoral access was used to engage left maincoronary artery, followed by passage of one 0.014” coronary guidewire into terminalleft anterior descending coronary artery. Sequentially, we then used a guideextension to cross pseudoaneurysm, then introduced Confida pre-shaped guidewire, and finally 7F Judkins right coronary guide catheter was passed into thepseudoaneurysm. The Judkins right guide catheter facilitated for a 5F shuttlesheath, for placement of an 6 x 4mm Amplatzer Duct Occluder. Meanwhile, a drug-eluting stent was standby inleft anterior descending coronary artery by using guide extension catheter. Amplatzer Duct Occluder II 6 x 4mm was deployed at the entry point ofcoronary button dehiscence under TEE guidance, and immediate thrombus formationwas demonstrated. Owing to partial protrusion of occluder into leftmain coronary artery, the 4.0 x 15mm drug-eluting stent which was standby in leftanterior descending artery was pull back and deployed consecutively. Three-dimensionalechocardiography showed patent left main coronary artery after occluderdeployment and left main coronary stenting. Finalangiogram and TEE showed well-seated devices with minimal residual leak.

Case Summary
Post-Bentall pseudoaneurysms were reported in 6% to 10% of patientsdue to anastomotic and coronary dehiscence. Even though surgical repair ofpseudoaneurysms following aortic surgery can be safely performed with goodlong-term outcomes, these procedures carry high mortality and prolongs hospitalstay. In ourpatient, the pseudoaneurysm bleed originated at the anastomosis of the aorticroot graft involving the left coronary button. Cathetermanagement in post-Bentall pseudoaneurysms is limited.4 To the best of ourknowledge, there has been no specific prior report addressing simultaneousoccluder deployment and coronary stenting.