
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-136
Acute Coronary Occlusion After Drug-Eluting Balloon
By Sunanto Ng
Presenter
Sunanto Ng
Authors
Sunanto Ng1
Affiliation
Universitas Pelita Harapan, Indonesia1,
View Study Report
TCTAP C-136
CORONARY - Drug-Eluting Balloons
Acute Coronary Occlusion After Drug-Eluting Balloon
Sunanto Ng1
Universitas Pelita Harapan, Indonesia1,
Clinical Information
Patient initials or Identifier Number
RSUS.829703
Relevant Clinical History and Physical Exam
A male patient, 66 year-old, presented with angina-on-effort which was increasing in intensity within few months. He had history of previous percutaneous coronary intervention (PCI) and history of ischemic stroke. His atherosclerotic risk factor was hypertension and ex-smoker. He had refused coronary by-pass surgery since the first PCI. His routine medication was aspirin 80 mg, clopidogrel 75 mg, atorvastatin 40 mg, amlodipin 10 mg, candesartan 16 mg, and bisoprolol 5 mg.
Relevant Test Results Prior to Catheterization
His electrocardiogram revealed sinus rhythm without any Q wave nor ST-T segment deviation. He has moderately impaired kidney function with estimated glomerular filtration rate of 45 mL/min/1.73 m2. His echocardiogram revealed mildly reduced systolic function (left ventricular ejection fraction of 45%) with hipokinesia of anteroseptal wall.
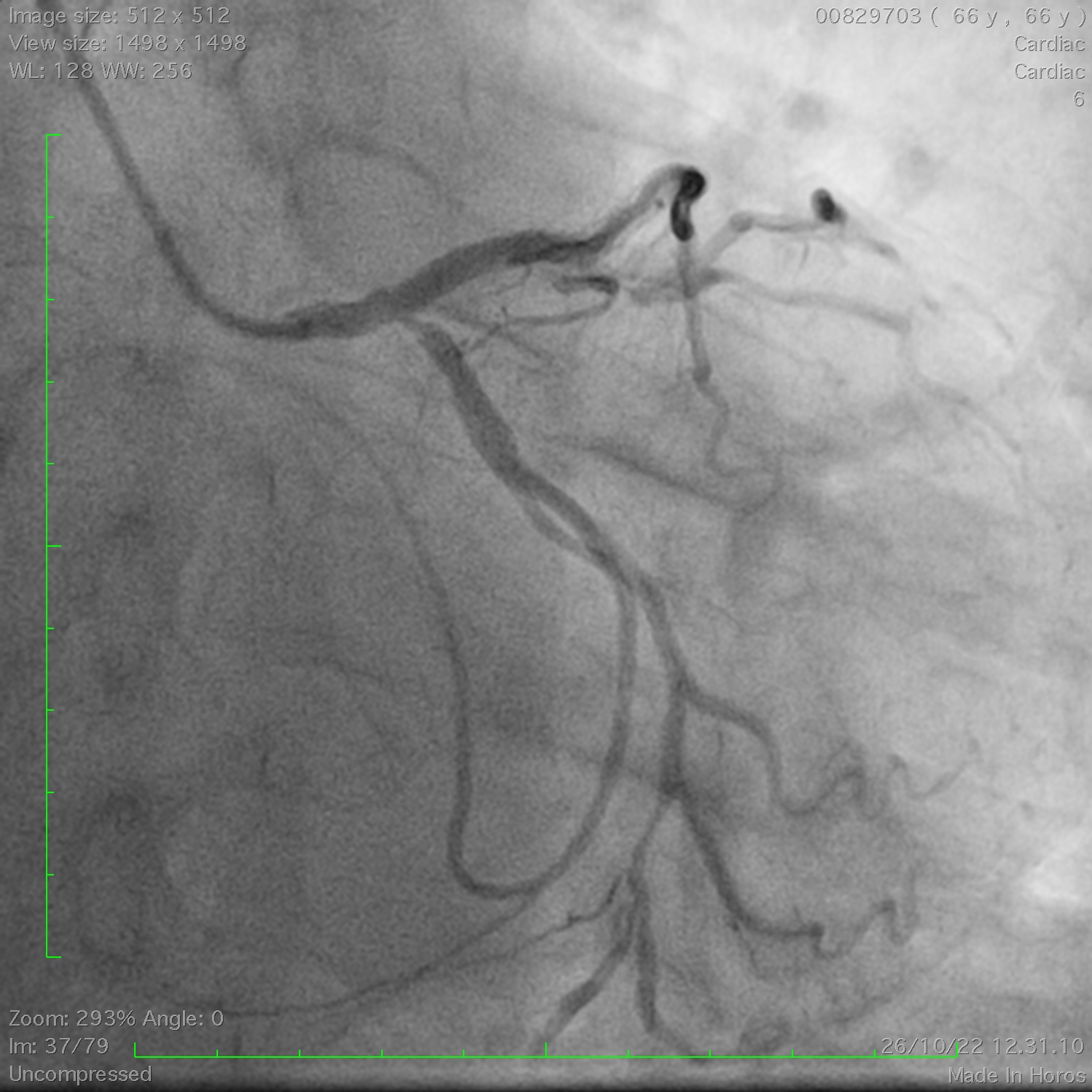
Relevant Catheterization Findings
Angiography revealed patent stents at the right coronary (RCA) and left anterior descending (LAD) coronary artery. The left main stem (LM) was dubiously having tubular stenosis without significant angiographic obstruction. There was a severe stenosis at the ostium of left circumflex artery (LCx) and at the distal part of the LCx (Figure). Considering his reluctance to surgery, a PCI to the LCx ostium with drug-eluting balloon (DEB) was planned to relieve his ischemic symptom.
Interventional Management
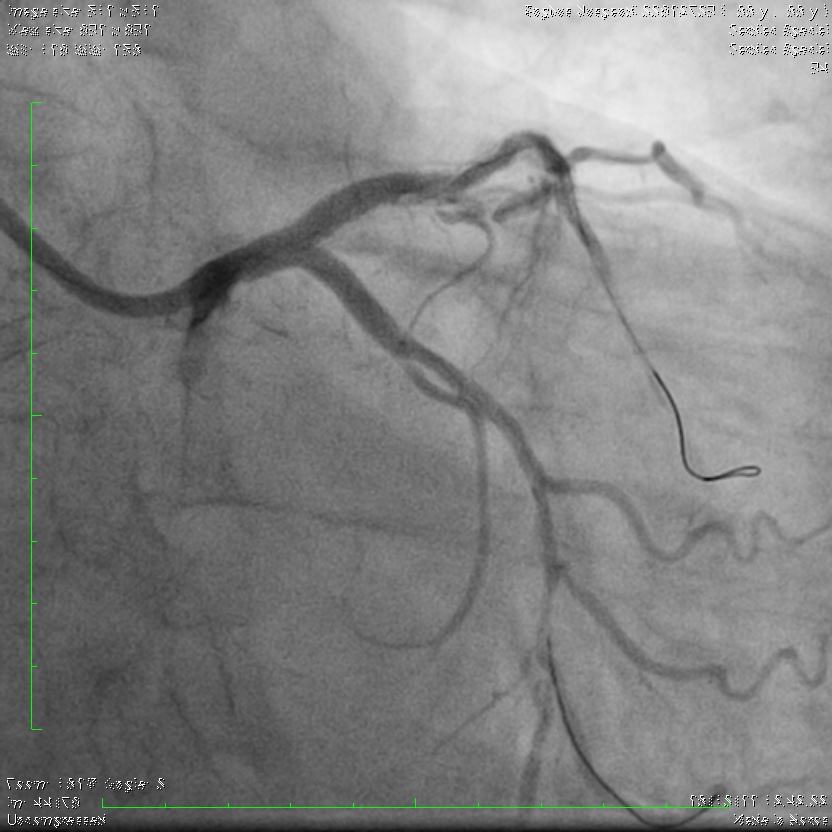
Procedural Step
PCI to the osteal LCx was done as follow: optimal lesion preparation and DEB. Lesion preparation was done with non-compliant (NC) scoring balloon 2.75 mm up to 20 atm. Lesion was subsequently treated with Paclitaxel-coated balloon 3.0 mm. Because of geometric change at the ostium of LAD, procedure was ended with kissing balloon to the LM-LAD-LCx, with good result. Four hours later, the patient experienced severe chest pain. ECG did not showed any new ST-T segment deviation. Nevertheless, an immediate PCI was done. Angiography revealed subtotal occlusion of ostium LCx (Figure). Occlusion was immediately dilated. Subsequently, two drug-eluting stent (DES) was implanted to the LM-LAD-LCx with double-kissing crush (DK crush) technique. Proximal optimisation technique was done to the LM part of the stent (Figure). Patient was relieved from chest pain and discharged the day after.

Case Summary
Coronary occlusion is one of the complication of angioplasty with DEB. Close observation within hours should be done after such procedure. If coronary occlusion occurred at the coronary ostium after an angioplasty with DEB, a two-stent strategy (such as DK crush) for bifurcation might be needed to mitigate that complication.