
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-084
When CTO Case Turns to Simple
By Azfar Hossain Bhuiyan
Presenter
Azfar Hossain Bhuiyan
Authors
Azfar Hossain Bhuiyan1
Affiliation
Evercare Hospital Dhaka, Bangladesh1,
View Study Report
TCTAP C-084
CORONARY - Chronic Total Occlusion
When CTO Case Turns to Simple
Azfar Hossain Bhuiyan1
Evercare Hospital Dhaka, Bangladesh1,
Clinical Information
Patient initials or Identifier Number
MR. AH, 45 YRS
Relevant Clinical History and Physical Exam
THIS NON DIABETIC PATENT CAME WITH EXERTIONAL CHEST PAIN (ANGINA CLASS-II)
CAD RISK FACTORS: HYPERTENSION, DYSLIPIDAEMIA, POSITIVE F/H OF CAD, SMOKER.
PULSE:80 B/MIN, BP: 120/80 MMHG, HEART & LUNGS: NAD
Relevant Test Results Prior to Catheterization
ECG: SINUS BRADICARDIA with ST-T CHANGES IN ANTERIOR LEADS
ECHO: NO RWMA. GOOD LV SYSTOLIC FUNCTION (EF- 60%)
TROPONIN-I- NORMAL, CREATININE: 1.20 MG/DL,HB- 15.2 GM/DL
ANTI HCV RAPID TEST- NEGATIVE, ANTI HIV I/II RAPID TEST- NEGATIVE, HBSAG RAPID TEST: NEGATIVE
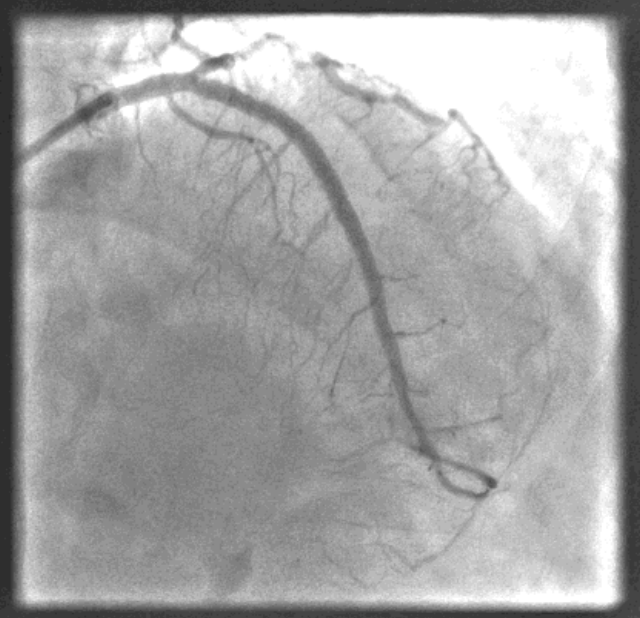
Relevant Catheterization Findings
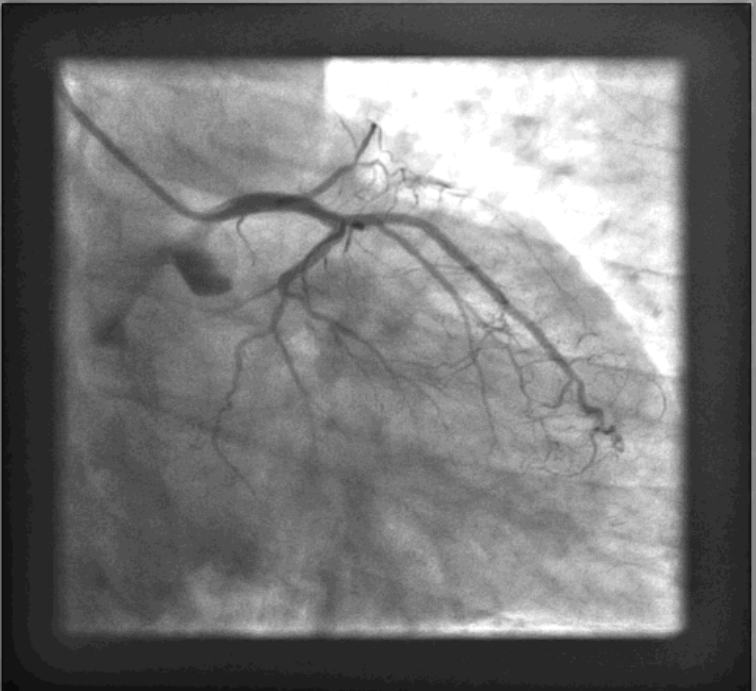
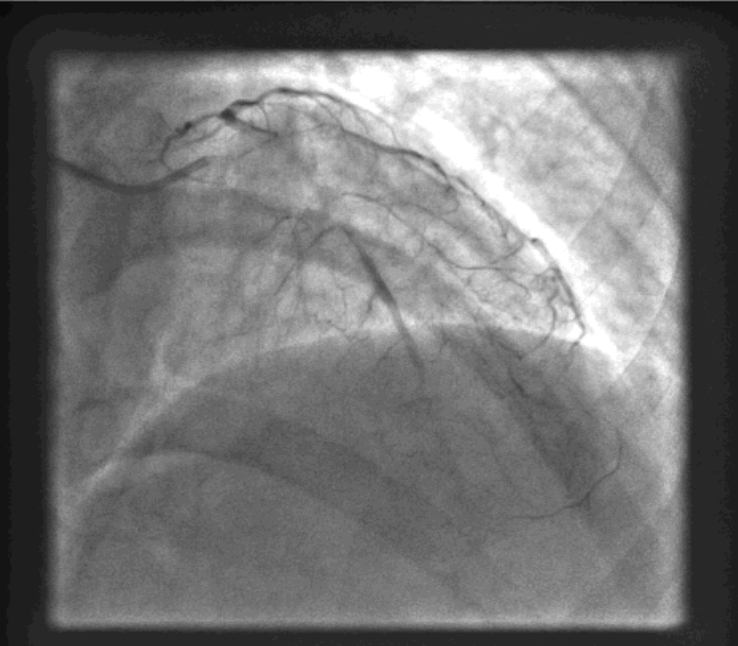
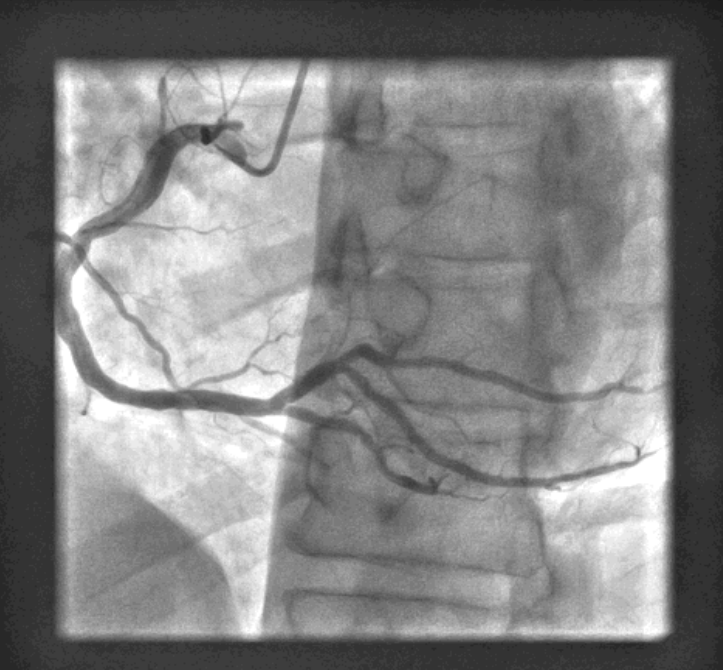
LMCA: Normal. LAD: Totally occluded from its ostium. Distal LAD filled retrogradely by right system. LCX: Medium size vessel & normal. OM1 is a resonable size vessel & normal. RCA: Dominant, Good size vessel and normal.
Interventional Management
Procedural Step
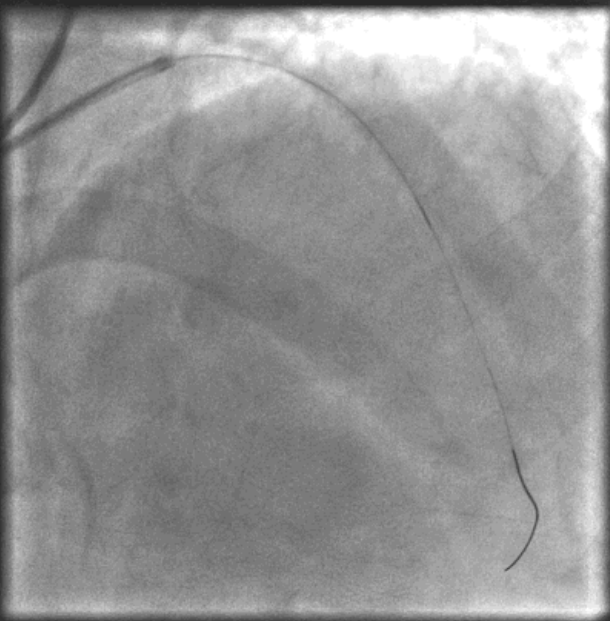
LM-LAD: LCA was engaged with the guiding catheter EBU-3.5 (6F). An Intermediate wire was attempted to cross the lesion with the help of caravel Cath but failed. Finally, a Gaia first wire was crossed the lesion of LAD with the help of caravel cath. Gaia wire exchange with caravel catheter. Pre-dilatation was done with 1.25 x 10 mm, 2.0 x 15 mm balloon at 08-10 ATM successively. LM-mid LAD lesion was stented with a 3.0 x 48 mm DES at 12 ATM. Overlapping the previous stent and covering thedistal LAD lesion with a 2.5 x 32 mm DES was deployed at12-14 ATM. Post dilatation was done with 3.5 x 10mm & 3.0x 12 mm balloon successively at 14-20 ATM. Final angiogram showed LM-LAD was well dilated with TIMI-III distal flow.

Case Summary
●No Case is Simple in Intervention.
●But sometimes complex case becomes simple when everything goes smoothly.
●In our case patient was financially poor & we were not fully prepared as usually CTO case should be prepared. We just tried and succeeded.
●CTO lesion is always a challenge for the interventionists. It doesn't always require full armament to be successful.
●Patience is the key to success.
●Patients are the main center of focus. Courage & Preparedness to tackle any untoward consequence is the key to success and save lives.