
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-058
Operation Shock and Awe: The Use of Intravascular Lithotripsy in a Critical Left Main Bifurcation Lesion
By Jian-Chen Lim, Koon Wee Koay, Ho Lam, Ping Wa Yam
Presenter
Jian-Chen Lim
Authors
Jian-Chen Lim1, Koon Wee Koay2, Ho Lam3, Ping Wa Yam3
Affiliation
Hospital Serdang, Malaysia1, Penang General Hospital, Malaysia2, Tuen Mun Hospital, Hong Kong, China3,
View Study Report
TCTAP C-058
CORONARY - Bifurcation/Left Main Diseases and Intervention
Operation Shock and Awe: The Use of Intravascular Lithotripsy in a Critical Left Main Bifurcation Lesion
Jian-Chen Lim1, Koon Wee Koay2, Ho Lam3, Ping Wa Yam3
Hospital Serdang, Malaysia1, Penang General Hospital, Malaysia2, Tuen Mun Hospital, Hong Kong, China3,
Clinical Information
Patient initials or Identifier Number
WYM
Relevant Clinical History and Physical Exam
A 68-year-old lady with underlying hypertension and type 2 diabetes mellitus for 20 years. She presented to the Accident and Emergency Department with sudden onset of left sided chest pain for 1 day while resting, associated with diaphoresis. She did not complain of dyspnea on exertion nor heart failure symptoms, but has strong family history of ischemic heart disease. Vital signs were stable and physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
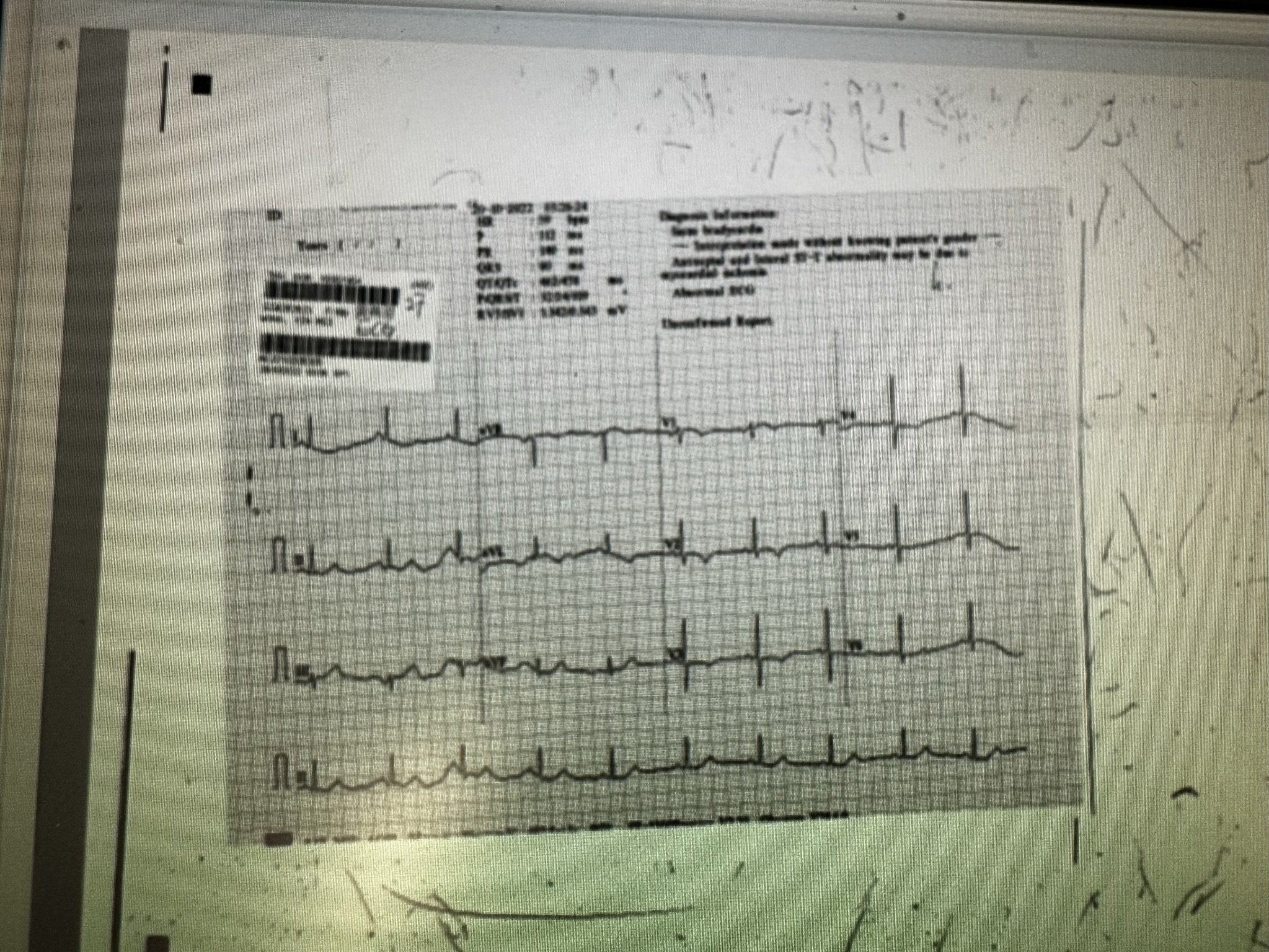
12-lead electrocardiography (ECG) showed ST elevation at lead aVR and V1, with wide spread ST depression and T inversion at the other leads. Chest X ray was unremarkable. Echocardiography showed normal left ventricular function with ejection fraction (EF) of 65% without regional wall motion abnormality. High-sensitive Troponin I was markedly raised. Full blood count, liver function, and renal profile tests were normal.
Relevant Catheterization Findings
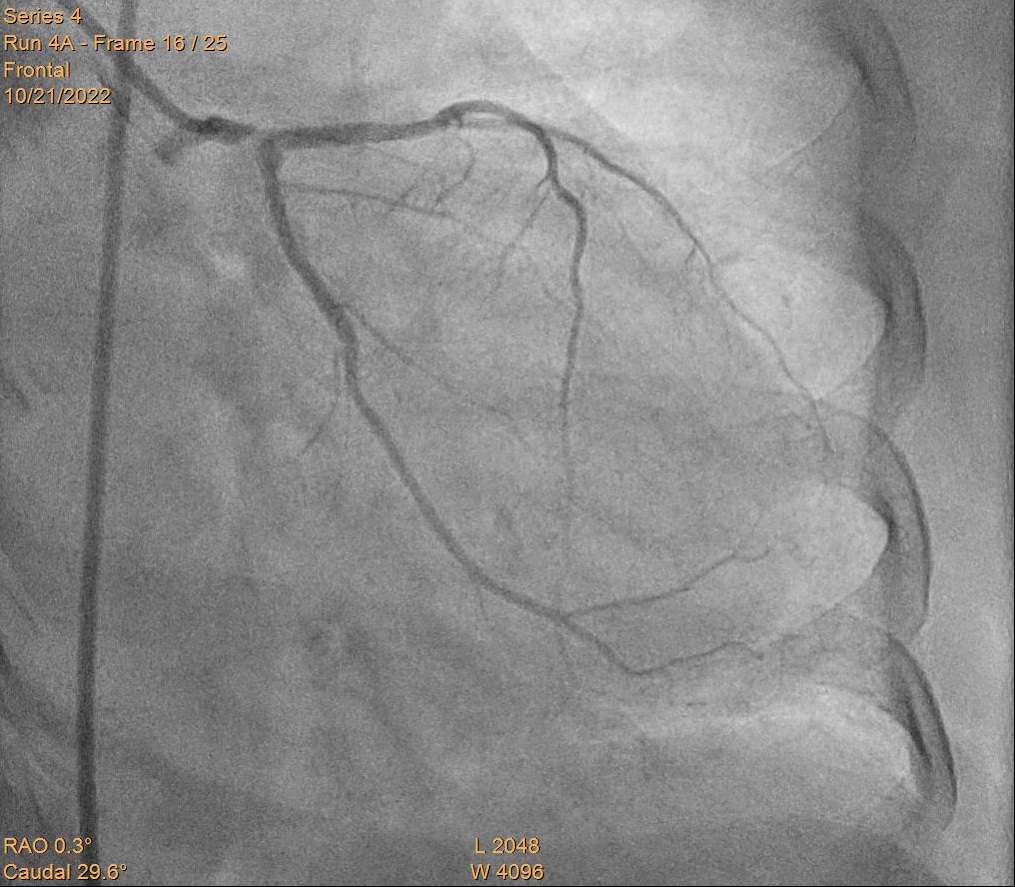
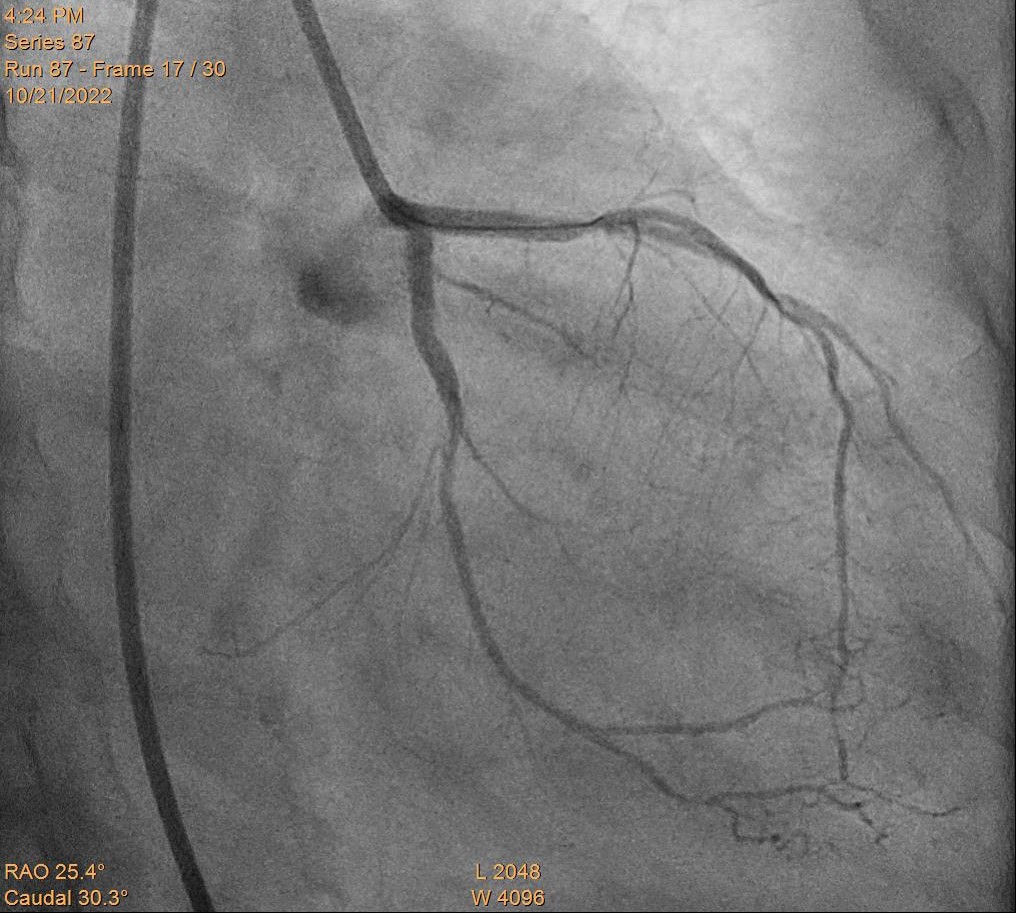
Coronary angiography via right femoral artery (RFA) with 6F Judkins left (JL) 3.5 and Judkins right (JR) 4 diagnostic catheters showed critical calcified stenosis at distal left main(LM), ostial left anterior descending (LAD) artery, and ostial left circumflex(LCX) artery (Medina 1.1.1). There was a dominant obtuse marginal branch (OM) and smallish distal true LCX. Mid right coronary artery (RCA) was noted to have moderate stenosis.
Interventional Management
Procedural Step
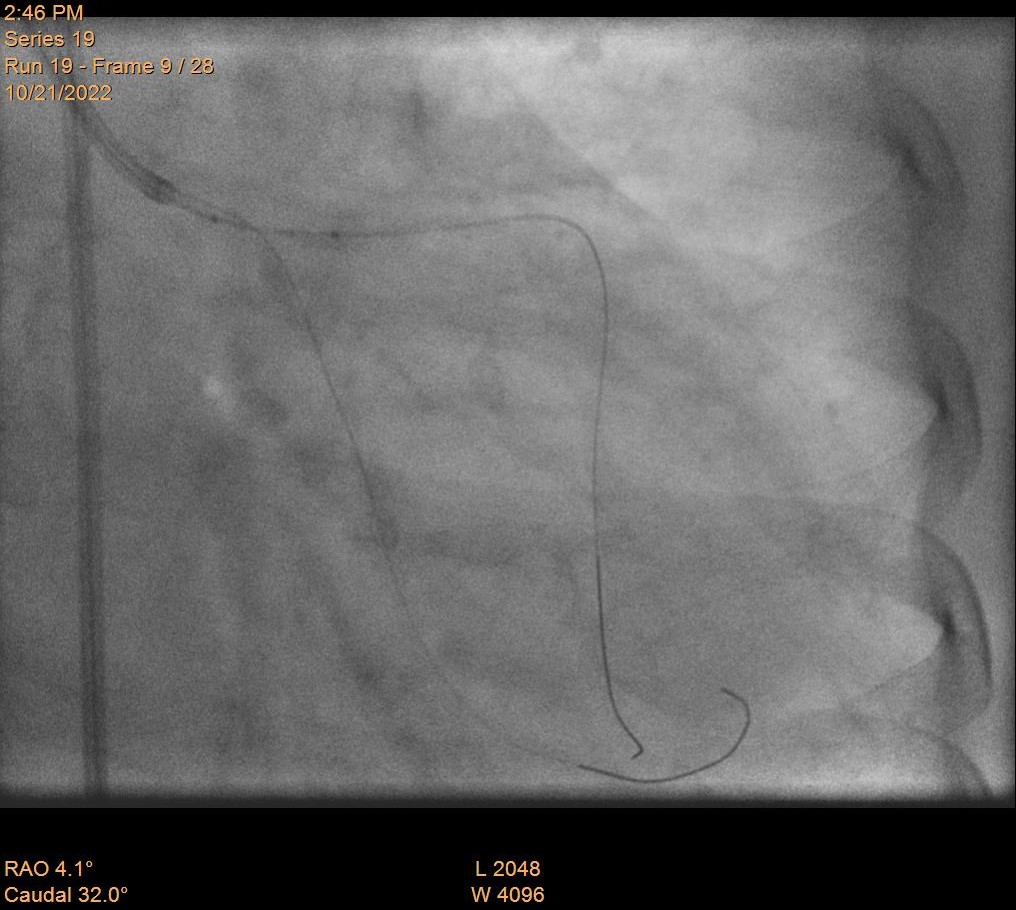
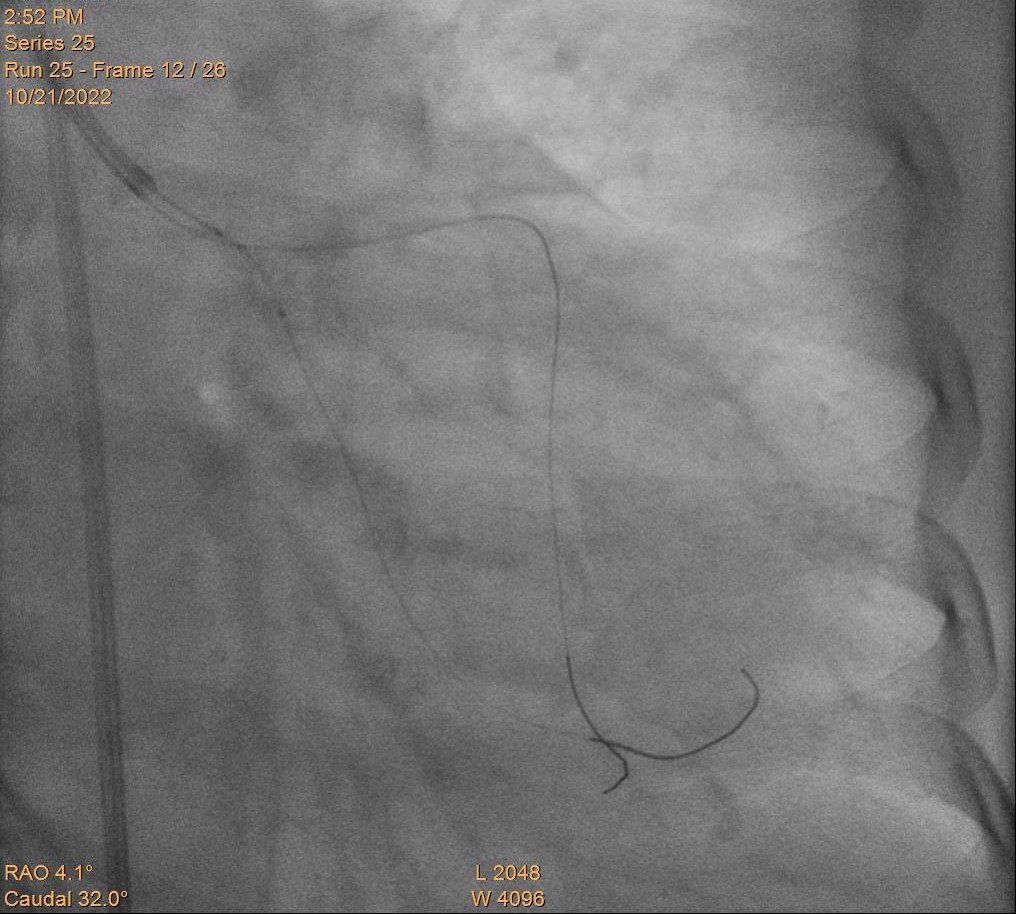
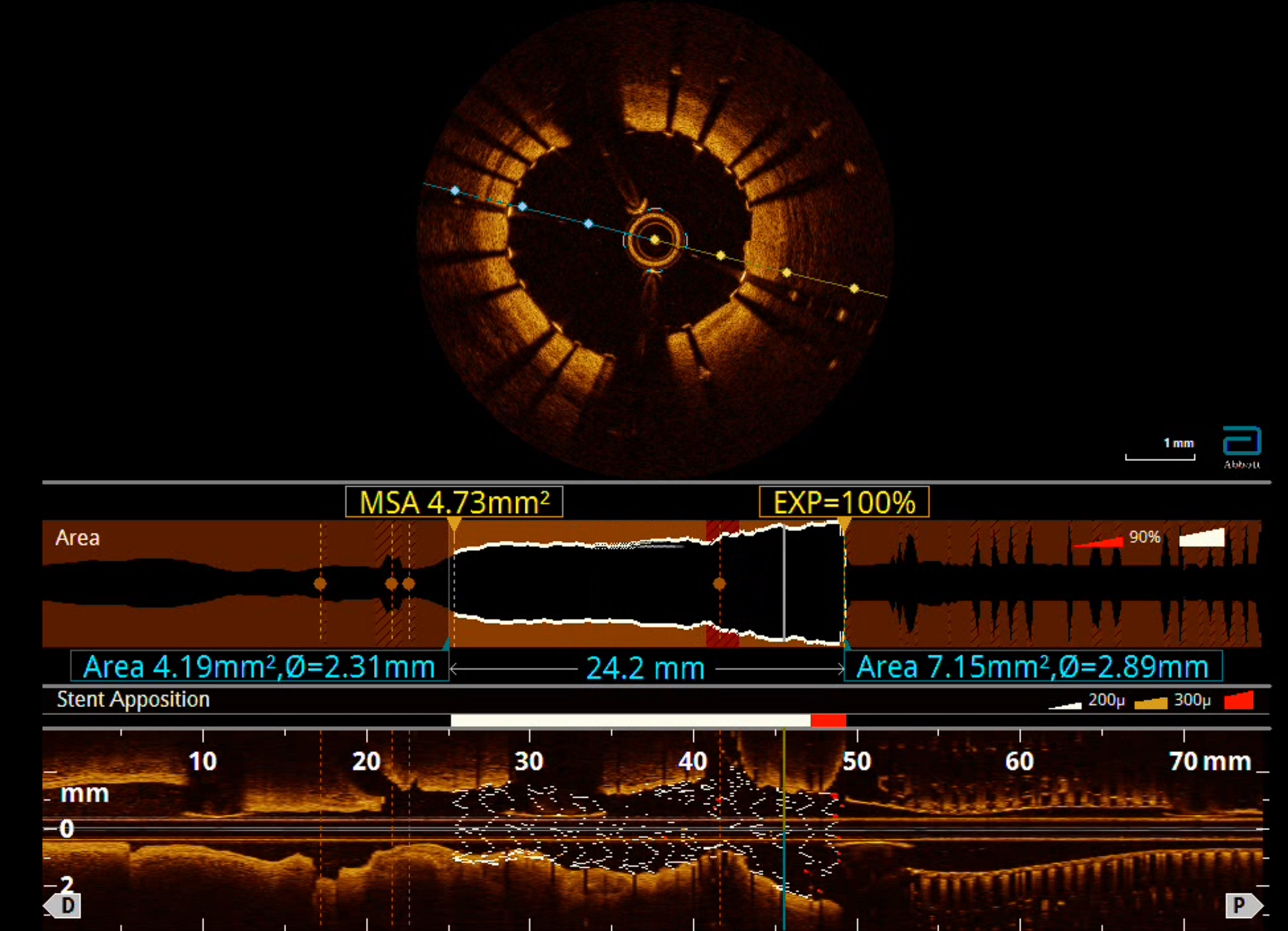
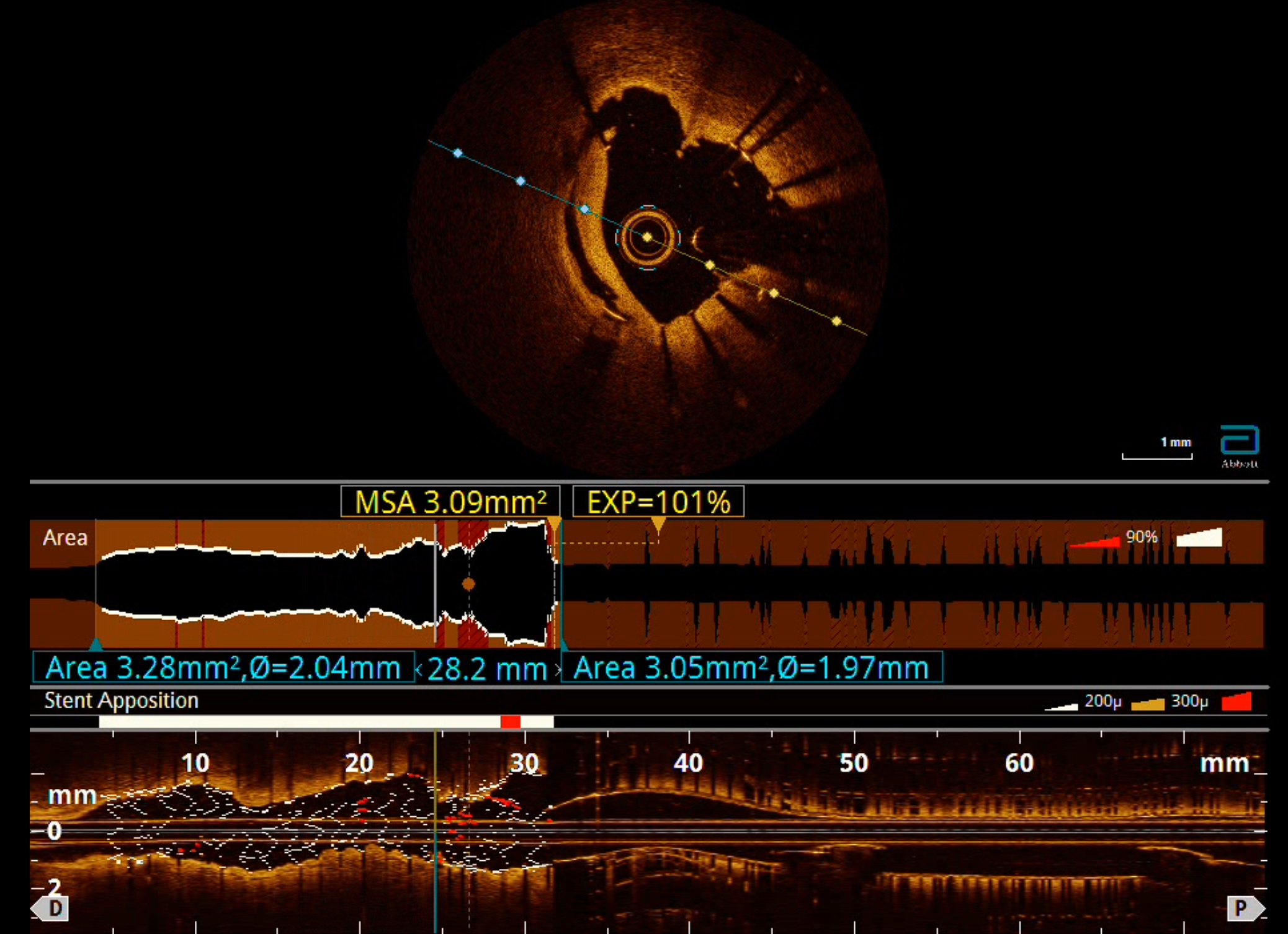
Left coronary artery was engaged with 7F JL 3.5 guiding catheter via RFA. Sion Blue was wired into LAD. Distal LM was predilated with a semi-compliant (SC) 1.5 mm balloon, followed by a non-compliant (NC) 2 mm balloon. Runthrough NS Floppy was wired into main OM. Shockwave Intravascular Lithotripsy (S-IVL) was done with a 3 mm IVL catheter at proximal LAD to distal LM for 8 cycles. This was followed by S-IVL from proximal to ostial LCX with a 2.5 mm IVL catheter for 8 cycles. Proximal to ostial LCX was predilated with a NC 2.5mm balloon, and was stented with a 2.5 x 23mm drug eluting stent (DES), followed by postdilatation with a NC 2.75 mm balloon. The LCX wire was removed and proximal LCX stent strut was crushed with a NC 2.75 mm balloon placed in the LM. The proximal LAD was stented with a 2.5 x 15 mm DES, followed by a 3.5 x 12 mm DES from proximal LAD to ostial LM. Postdilatation was done with a NC 4 mm balloon at ostial LM, then with a NC 3 mm balloon from proximal LAD to distal LM. Main OM was rewired and ostial LCX stent strut was opened with a SC 1 mm balloon, then a SC 1.5 mm balloon. Sequential kissing balloon inflation was performed with a NC 3 mm balloon each at LM-LAD and LM-LCX. Proximal optimization was done at ostial LM with a NC 4.25 mm balloon. Optical coherence tomography at both LM-LAD and LM-LCX showed stents were well expanded and apposed. Prolapsed tissue was seen within the proximal LCX stent but final angiographic result was satisfactory.
Case Summary
Patient was admitted overnight for observation and was discharged well the next day. Patient remained well and asymptomatic during clinic follow up 4 weeks after the percutaneous coronary intervention. This case shows that Shockwave Intravascular Lithotripsy is an effective, feasible, and safe calcium modification technique even when performed in a critical LM bifurcation lesion.