
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-116
A Challenging Case Report: Management of Elongated Entrapped Coronary Wire in a Challenging Left Main Bifurcation left
By Tsz Ho Chan, Shung Yee Wong, Chi Wing Wong, Eugene Brian Wu
Presenter
Tsz Ho Chan
Authors
Tsz Ho Chan1, Shung Yee Wong1, Chi Wing Wong1, Eugene Brian Wu2
Affiliation
Pok Oi Hospital, Hong Kong, China1, Prince of Wales Hospital, Hong Kong, China2,
View Study Report
TCTAP C-116
CORONARY - Complications (Coronary)
A Challenging Case Report: Management of Elongated Entrapped Coronary Wire in a Challenging Left Main Bifurcation left
Tsz Ho Chan1, Shung Yee Wong1, Chi Wing Wong1, Eugene Brian Wu2
Pok Oi Hospital, Hong Kong, China1, Prince of Wales Hospital, Hong Kong, China2,
Clinical Information
Patient initials or Identifier Number
Cheung LK
Relevant Clinical History and Physical Exam
75 years old, good past health, independent daily living, was admitted for Acute coronary syndrome and congestive heart failure
He presented mainly as shortness of breath on exertion, orthopnea and lower limb edema. He complained of mild or minimal chest discomfort.
Blood pressure was stable. On 2L oxygen support. Heart sound dual. 2/6 diastolic murmur heard at left lower sternal border
Relevant Test Results Prior to Catheterization
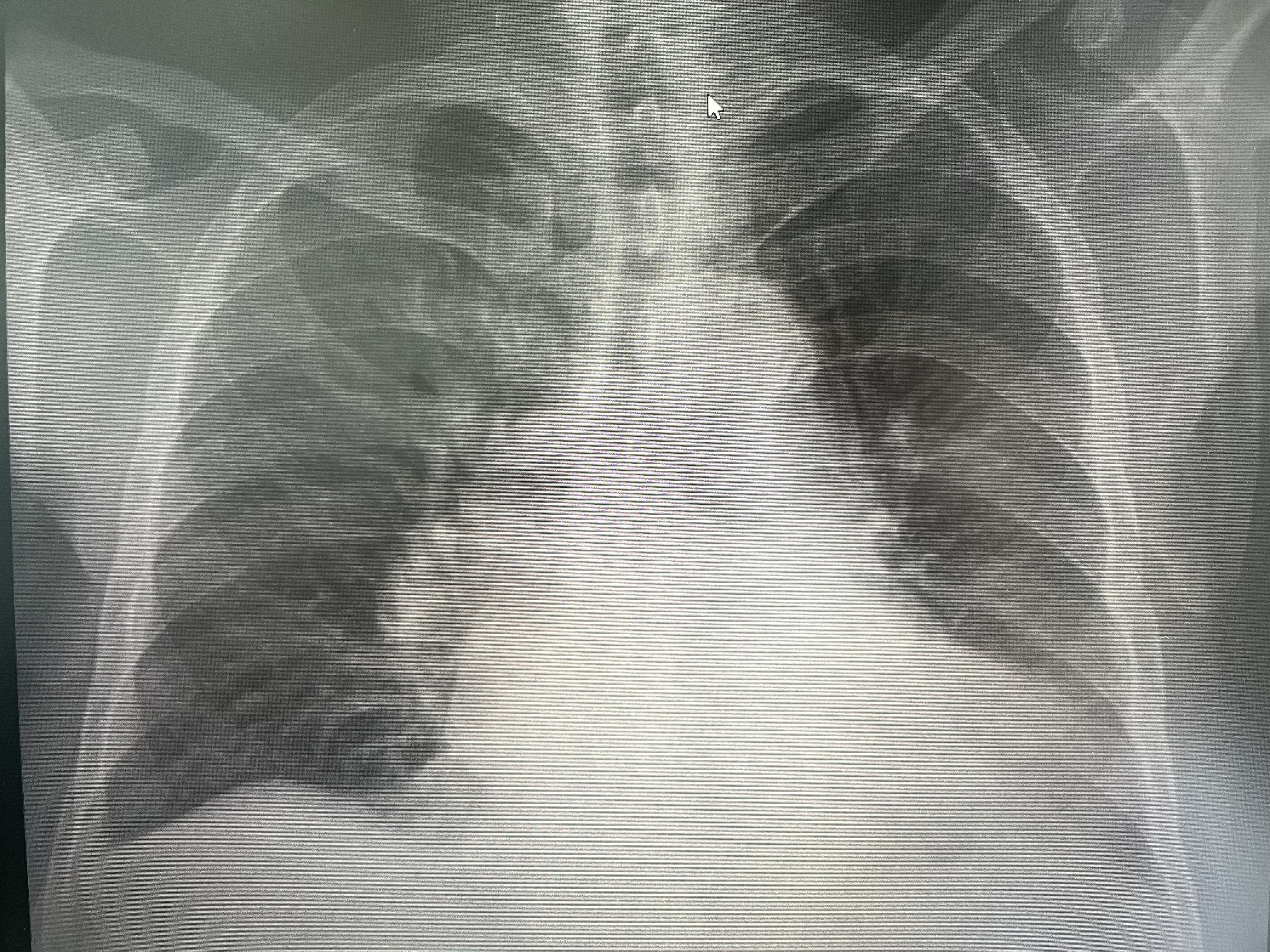
Chest X ray showed mild right lower zone haziness and slightly congested

Electrocardiogram showed sinus rhythm, no ST changes, new T wave inversion seen over lateral leads
Serial troponin I showed peak at 700 ng/L
Echocardiogram showed dilated bi-atrium and left ventricle, impaired left ventricular systolic function, 38.7%, global hypokinesia, trileaflet aortic regurgitation with mod aortic regurgitation, other valves are unremarkable.
Echocardiogram showed dilated bi-atrium and left ventricle, impaired left ventricular systolic function, 38.7%, global hypokinesia, trileaflet aortic regurgitation with mod aortic regurgitation, other valves are unremarkable.
Relevant Catheterization Findings
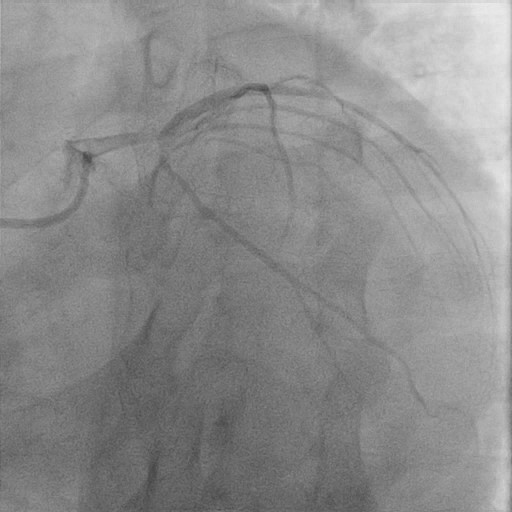
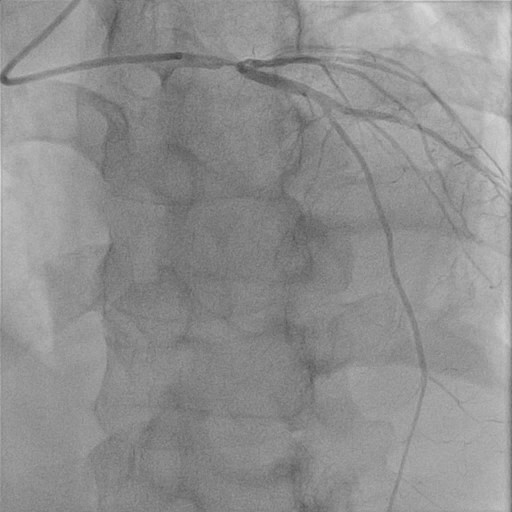
Coronary angiogram showed significant distal left main lesion bifurcation 90%; ostial LAD 90%; ostial LCX 80% with calcified lesions
 Mov 1.jpg
Mov 1.jpg
Mov 2.jpg

Mov 3.jpg
(angulation between LM-LCX can be seen in RAO caudal view & distal LM severity best seen in LAO Cranial view)
Other part of LAD and LCX arteries was minor disease; RCA showed dominant lesion but mild disease
LM bifurcation lesions classified as medina 1,1,1 & DEFINITION criteria as 2major+2 minor
Mov1: LAO Caudal view
Mov2: LAO Cranial view
Mov3: RAO Caudal view
Interventional Management
Procedural Step
Patient refused CABG

mov 4.jpg

Mov 5.jpg
Mov 6.jpg
The strategy was DK crush technique
After predilatation & IVUS analysis, LCX was stented and afterwards crushed with LM-LAD NC balloon. After rewiring the LCX by hydrophilic wire, we did the 1st kissing balloon step and LM-LAD was stented with the wire removed
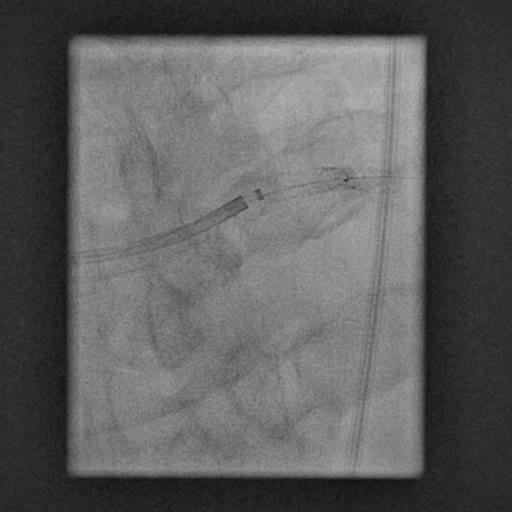
During rewiring to LCx again, the coronary wire was trapped and elongated after operator try to pull out the wire.
During rewiring to LCx again, the coronary wire was trapped and elongated after operator try to pull out the wire.
We first advanced the microcatheter down to try to release trapped area, then remove the wire. Afterwards the whole system including guiding catheter was removed with balloon inflated at the tip of guiding catheter to trap the wire. Another guiding catheter was engaged with ping pong technique. At first bedside echocardiogram did not show wire in aorta. We decided to put another stent in LM-LAD to cover the free floating wire.
Patient was brought to CT showing 20cm elongated wire protruding out to ascending aorta. Afterwards we decided to bring the patient to cath lab again. First we use trifold snare and to shorten the elongated trapped wire by removal. Afterwards the wire was pushed down to LAD by guideliner and covered with 3rd stent. Repeated IVUS showed no wire protruding aorta with confirmation of CT later. TIMI 3 flow all along. Patient was asymptomatic. FU echo in 1 yearshowed improvement in LVEF
Mov4: entrapped and elongated wire in guiding
Mov5: trifold snare to grab the free floating wire in aorta
Mov6: Guideliner pushing wire to LAD
Case Summary
This case demonstrated the tacking of entrapped coronary wire during procedure. Learning points including 1. Not to pull harshly when trapped to prevent the elongation wire happening2. Techniques discussion on trapped elongated wire : advancement of microcatheter, snare, twisted wire technique3. Discussion on conservative management vs treatment strategies on entrapped coronary wire4. General principle and techniques in treating entrapped gadgets in coronary intervention procedure