
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-067
To Invest or Not to Invest?
By Ying-Chang Tung
Presenter
Ying-Chang Tung
Authors
Ying-Chang Tung1
Affiliation
Linkou Chang Gung Memorial Hospital, Taiwan1,
View Study Report
TCTAP C-067
CORONARY - Chronic Total Occlusion
To Invest or Not to Invest?
Ying-Chang Tung1
Linkou Chang Gung Memorial Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
F.-S. Y.
Relevant Clinical History and Physical Exam
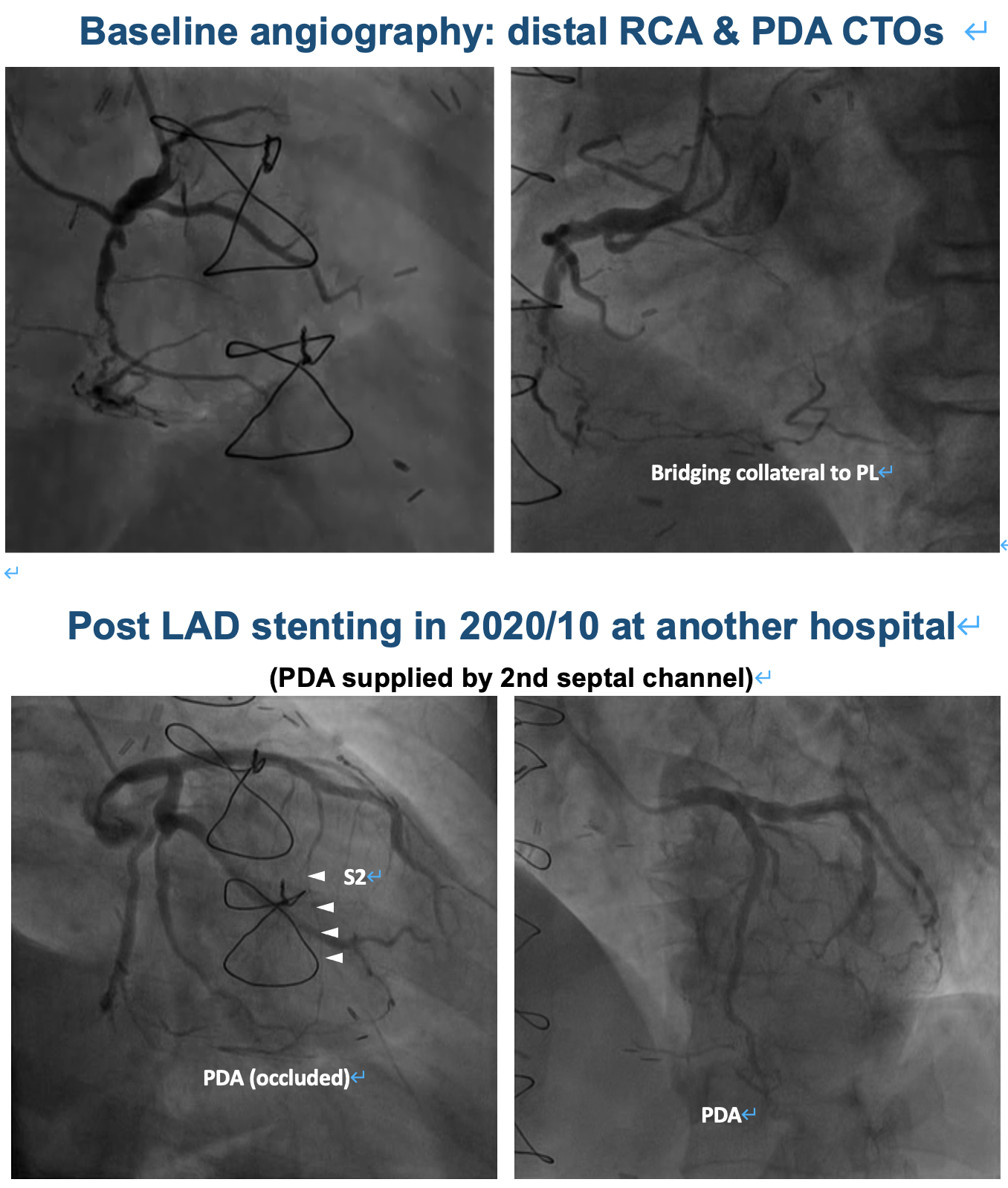
The patient is a 78-year-old man wit a history of HTN and CAD post CABG at an outside institute in 2019. He received LAD stenting due to graft failure in 2020/10 at another hospital. He was admitted to our hospital in 2022/1 for unstable angina. The thallium scan showed mixed myocardial ischemia and infarction in inferior segment of LV. CAG showed two CTOs in RCA and patent LAD stent and LCx. Add hoc PCI for RCA CTOs was attempted but failed.
Relevant Test Results Prior to Catheterization
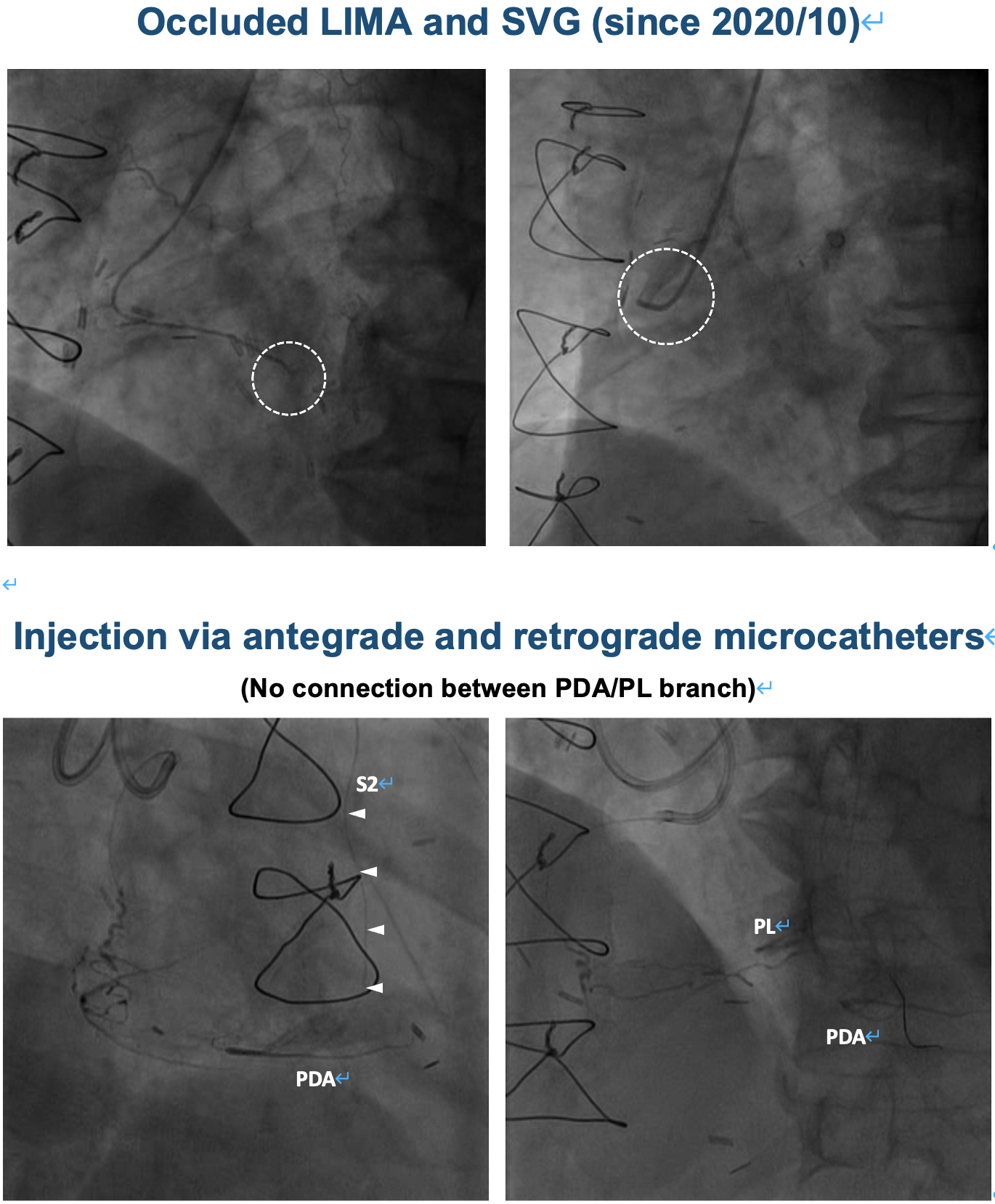
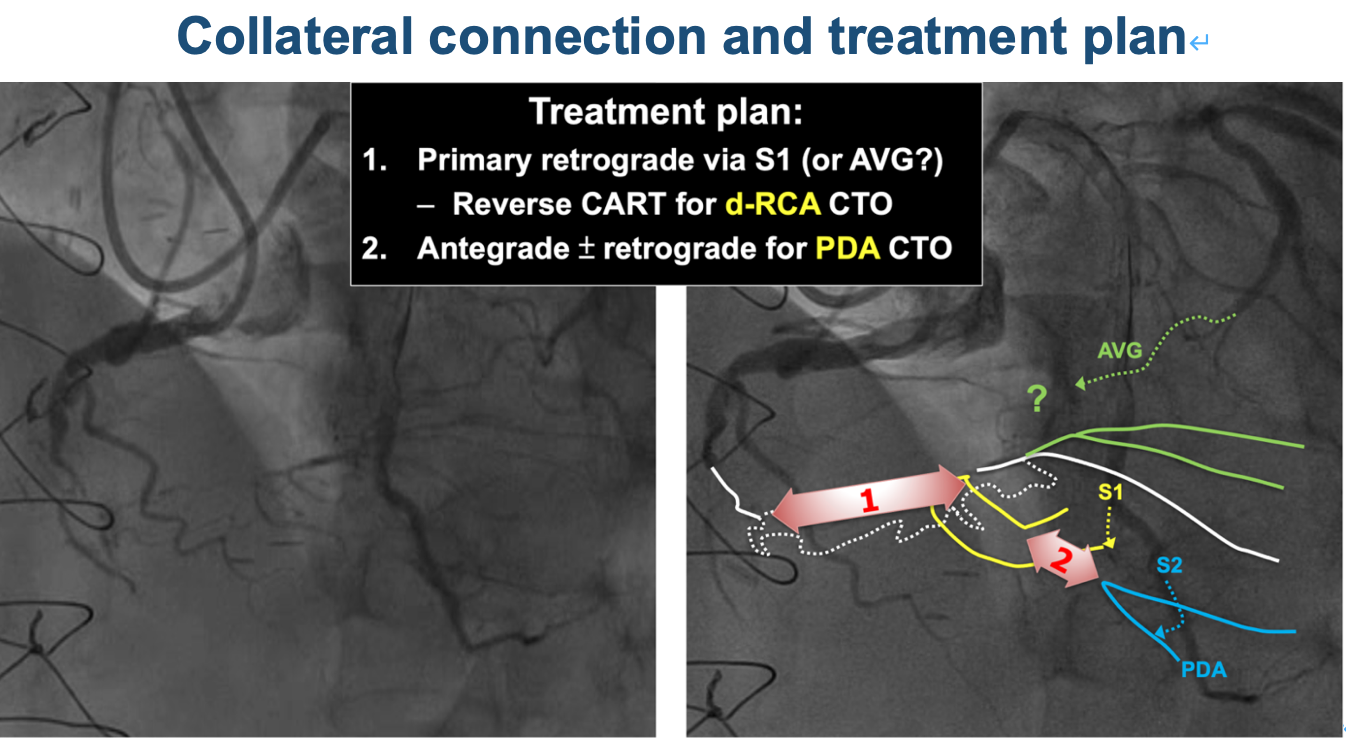
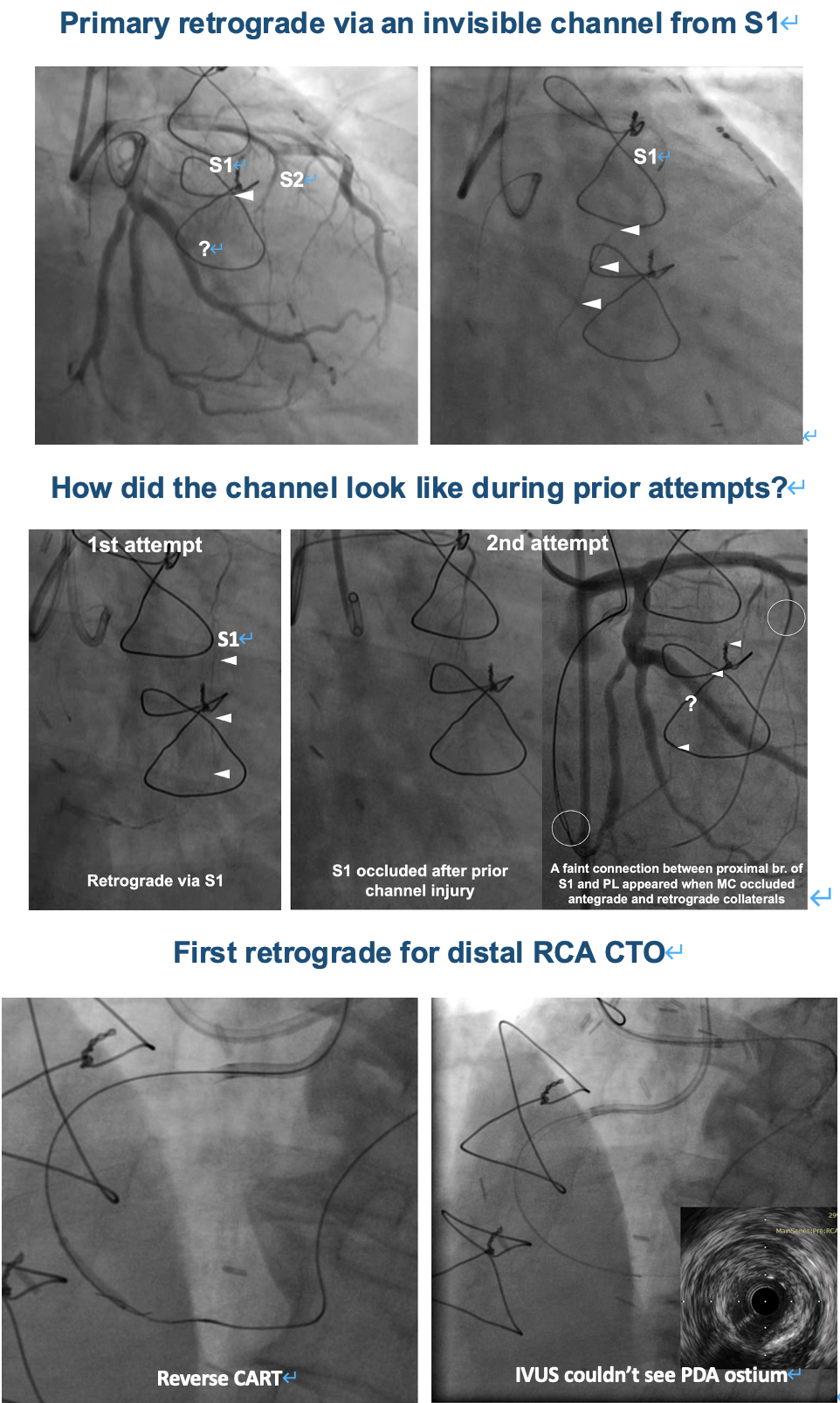
1st (ad hoc) PCI for distal RCA and PDA CTOs (2022/1/3):1. Failure to advance IVUS to examine proximal cap ambiguity2. Retrograde via S2 to PDA; failure to pass PDA CTO retrogradely3. Failure to pass AVG collateral4. Retrograde via S1 to a small branch before PDA5. Retrograde puncture of CTO exit at PDA/PLV bifurcation with the support of retrograde dual lumen catheter6. Failed reverse CART in distal RCA due to: (1) Inadequate antegrade GC support (2) S2 and PLV injury (3) Patient fatigue
Relevant Catheterization Findings
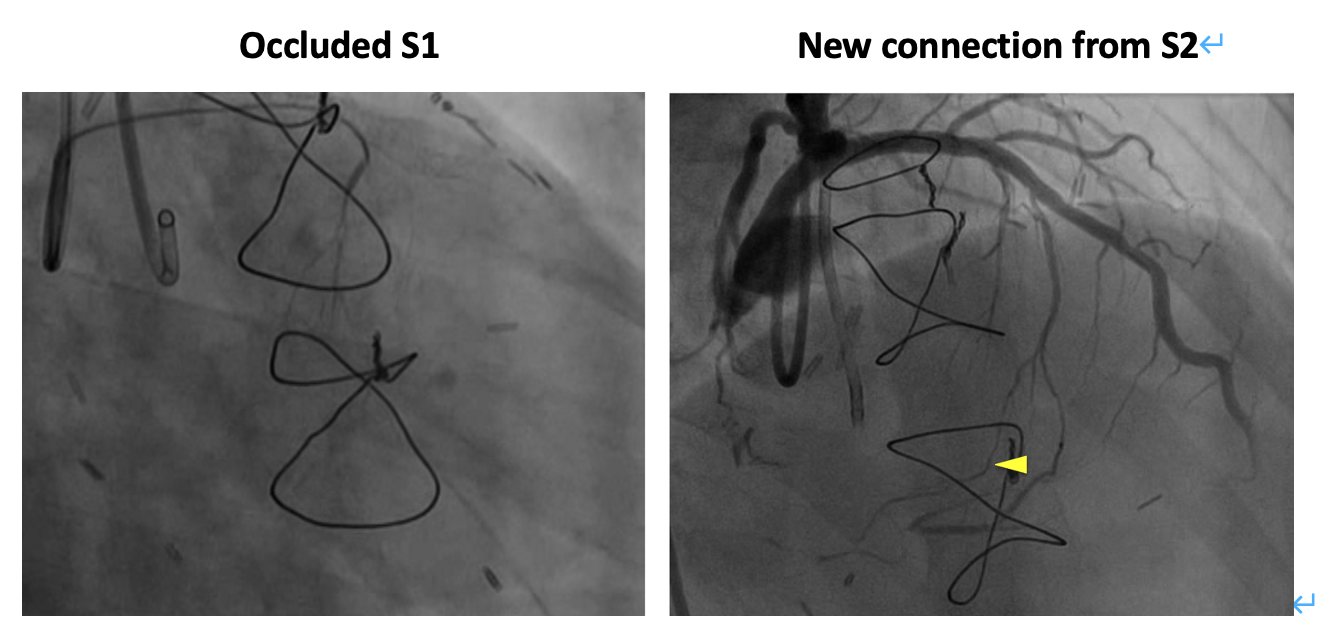
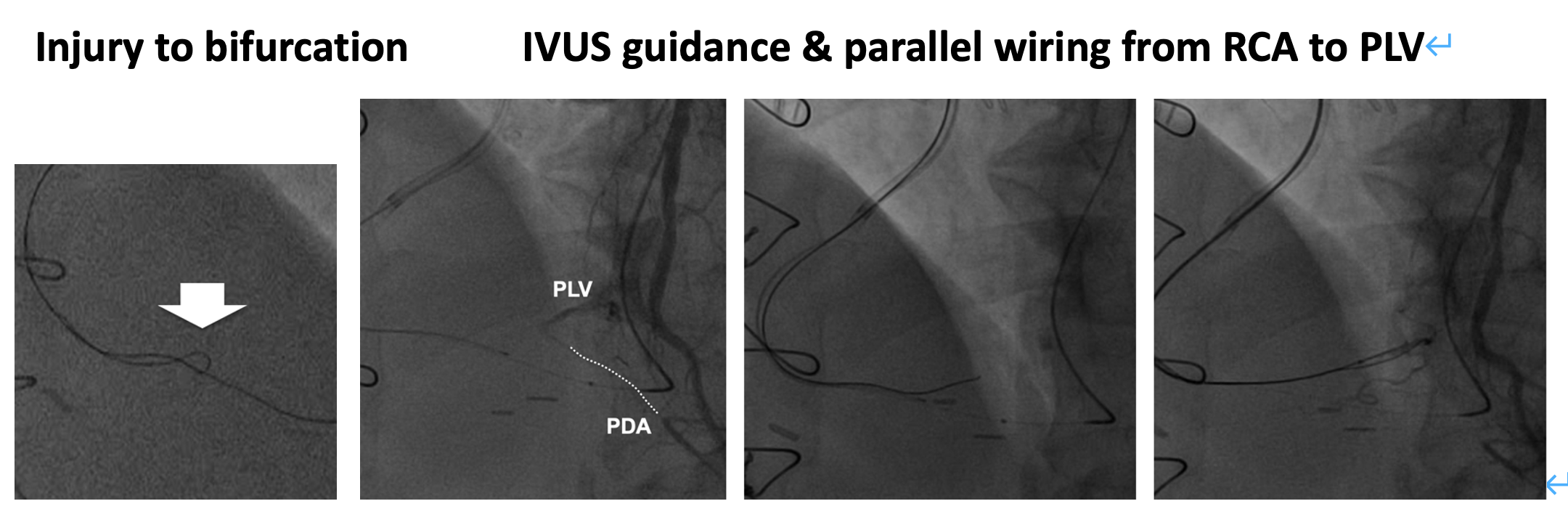
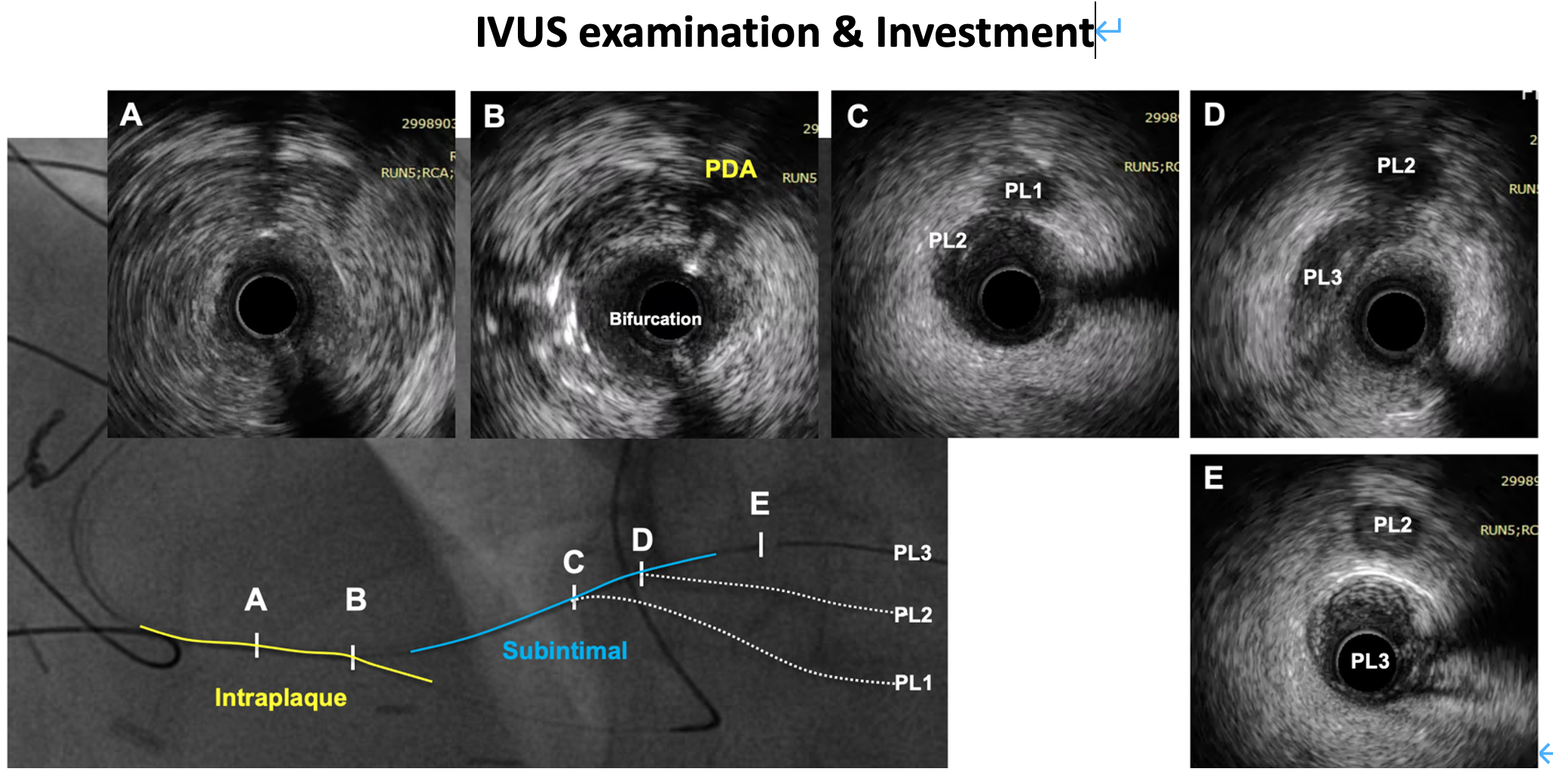
2nd attempt for distal RCA and PDA CTOs (2022/2/18):1. S1 was occluded after channel injury during prior attempt2. Primary retrograde via a new connection from a proximal branch of S2 to the small branch before PDA3. Successful reverse CART for distal RCA CTO, with the bifurcation injured by the antegrade wire4. IVUS-guided wiring from RCA to PLV 5. Parallel wiring to re-enter PLV at a very distal segment6. IVUS showed long subintimal tracking in PLV7. Investment and deferred stenting
Interventional Management
Procedural Step
3rd attempt (2022/4/19):
1. Angiography showed re-occlusion of the RCA CTO
2. Primary retrograde via an invisible channel from a proximal branch of S1 to PLV:
- No clear connection shown by selective injection of S1 in prior attempts
- Better alignment with the RCA CTO, thereby enhancing retrograde support and reducing the risk of injury to the bifurcation
3. Successful reverse CAR in distal RCA
- Prior investment procedure reduced tissue resistance and facilitated CTO recanalization
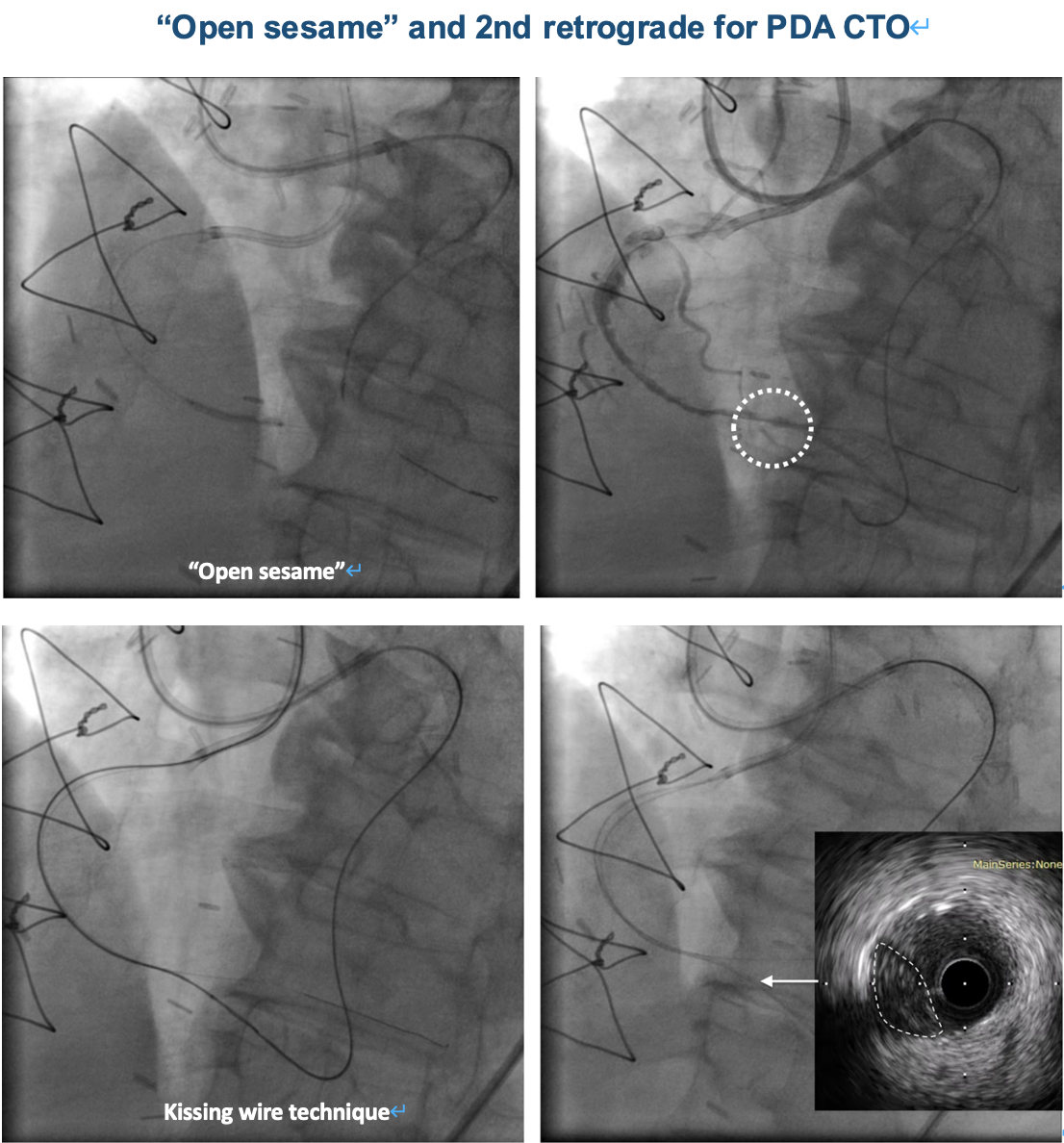
4. IVUS pullback showed intraplaque tracking but could not identify PDA entry
5. Stepwise balloon dilation from RCA to PLV to help visualize the orifice of PDA ("open sesame" technique)
6. Kissing wire technique to cross the PDA CTO
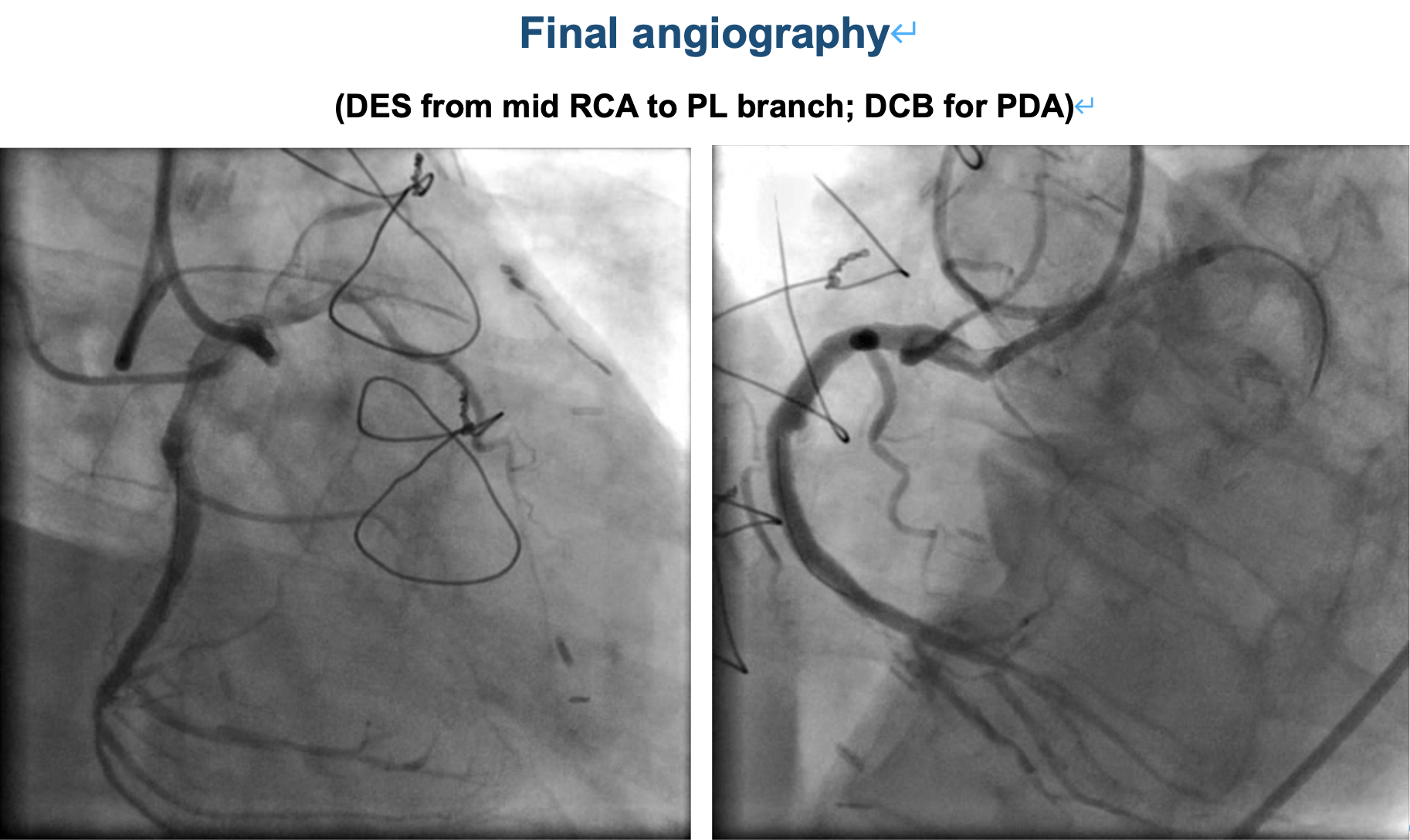
6. Stenting from PLV back to proximal RCA; DCB for PDA
Case Summary
1. Post-CABG CTO PCI: very challenging anatomy