
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-010
Covered Stents for the Management of Coronary Artery Aneurysm Thrombosis Causing ST-Elevation Myocardial Infarction
By Samir Ahnia, Mohamed Saad-Eddine Bouzghaia
Presenter
SAMIR AHNIA
Authors
Samir Ahnia1, Mohamed Saad-Eddine Bouzghaia2
Affiliation
King Abdulaziz Medical City, Saudi Arabia1, El Besma Private Hospital, Algeria2,
View Study Report
TCTAP C-010
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Covered Stents for the Management of Coronary Artery Aneurysm Thrombosis Causing ST-Elevation Myocardial Infarction
Samir Ahnia1, Mohamed Saad-Eddine Bouzghaia2
King Abdulaziz Medical City, Saudi Arabia1, El Besma Private Hospital, Algeria2,
Clinical Information
Patient initials or Identifier Number
M.A.
Relevant Clinical History and Physical Exam
The patient is a 45 year old male without remarkable past medical history. He presented to the emergency department 2 hours after the onset of a crushing chest pain.On physical examination he was slightly diaphoretic and his blood pressure was 90/50 mmHg.
Relevant Test Results Prior to Catheterization
An electrocardiogram (ECG) was obtained and showed inferior ST-elevation myocardial infarction (STEMI).
Aspirin, Ticagrelor and unfractionned heparin boluses were given and the patient was immediately admitted to the catheterization laboratory for primary percutaneous coronary intervention (PCI).
Aspirin, Ticagrelor and unfractionned heparin boluses were given and the patient was immediately admitted to the catheterization laboratory for primary percutaneous coronary intervention (PCI).
Relevant Catheterization Findings
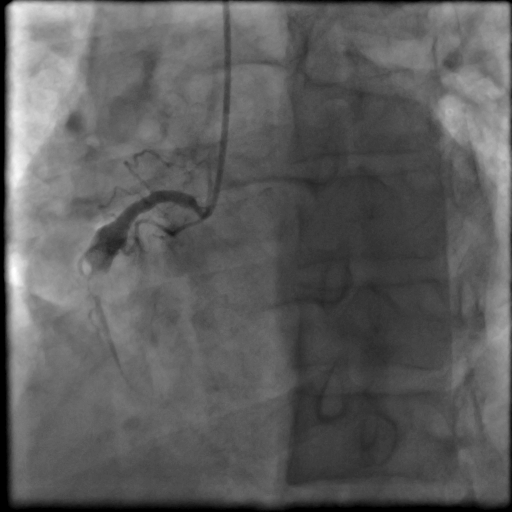
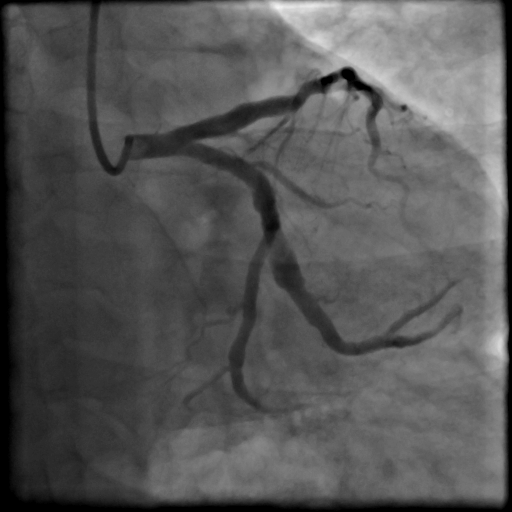
Right coronary angiography (Figure 1) revealed a subtotal occlusion of the right coronary artery (RCA) middle segment with a Thrombolysis In Myocardial Infarction (TIMI) 1 flow. A large thrombus was seen in an aneurysm just proximal to the subtotal occlusion and extending to the more distal non-aneurysmal segment.Left coronary angiography (Figure 2) showed ectatic obtuse marginal and severe stenosis of the left anterior descending artery (LAD) middle segment.
Interventional Management
Procedural Step
After vessel wiring, several balloon predilatations (4.0/20 mm non compliant balloon) and thrombus aspirations (6F Export™ catheter, Medtronic, USA) were necessary to restore a TIMI 3 flow.
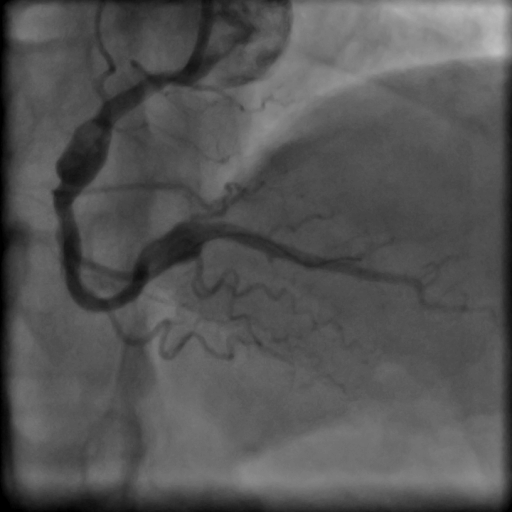
A residual large thrombus was present in the middle RCA aneurysm and another aneurysm was identified in the distal RCA segment (Figure 3).However, despite intravenous GP IIb IIIa inhibitors infusion (Tirofiban), flow rapidly deteriorated and RCA reoccluded.We decided to implant covered stents to exclude aneurysms in order to relieve blood stasis as a trigger of thrombus generation and to avoid distal embolization and subsequent no reflow.Two Graftmaster™ (Abbott, USA) covered stents were implanted to exclude aneurysms , a 3.5/19 mm for the distal RCA aneurysm and a 4.5/26 mm post-dilated with a 5.0 non compliant balloon for the mid-RCA aneurysm. Stenotic lesions of the ostio-proximal RCA and between the two covered stents were treated respectively with a 4.5/22 mm and 4.0/26 mm Resolute Onyx™ (Medtronic, USA) drug eluting stents. Immediate angiographic result was satisfactory (TIMI 3 flow, no distal embolization) (Figure 4)The patient was discharged after five days of uneventful course on dual antiplatlet therapy including Ticagrelor and Aspirin.A systematic angiographic and optical coherence tomography (OCT) control was performed 2 months later and showed complete stent endothelialization (Figure 5) without evidence of significant restenosis.


A residual large thrombus was present in the middle RCA aneurysm and another aneurysm was identified in the distal RCA segment (Figure 3).However, despite intravenous GP IIb IIIa inhibitors infusion (Tirofiban), flow rapidly deteriorated and RCA reoccluded.We decided to implant covered stents to exclude aneurysms in order to relieve blood stasis as a trigger of thrombus generation and to avoid distal embolization and subsequent no reflow.Two Graftmaster™ (Abbott, USA) covered stents were implanted to exclude aneurysms , a 3.5/19 mm for the distal RCA aneurysm and a 4.5/26 mm post-dilated with a 5.0 non compliant balloon for the mid-RCA aneurysm. Stenotic lesions of the ostio-proximal RCA and between the two covered stents were treated respectively with a 4.5/22 mm and 4.0/26 mm Resolute Onyx™ (Medtronic, USA) drug eluting stents. Immediate angiographic result was satisfactory (TIMI 3 flow, no distal embolization) (Figure 4)The patient was discharged after five days of uneventful course on dual antiplatlet therapy including Ticagrelor and Aspirin.A systematic angiographic and optical coherence tomography (OCT) control was performed 2 months later and showed complete stent endothelialization (Figure 5) without evidence of significant restenosis.
Case Summary
In the context of acute total or subtotal coronary artery occlusion involving large aneurysms and high thrombus burden, covered stents allow aneurysm exclusion, removing blood stasis as a trigger of thrombus generation, and reduce the risk of thrombus embolization.
Neo-intimal hyperplasia induced by covered stents is less likely to be angiographically significant and clinically relevant in large coronary segments.
Intra-coronary OCT control after few months is useful to evaluate covered stents endothelialization and further adapt antiplatelet treatment strategy and duration.
Neo-intimal hyperplasia induced by covered stents is less likely to be angiographically significant and clinically relevant in large coronary segments.
Intra-coronary OCT control after few months is useful to evaluate covered stents endothelialization and further adapt antiplatelet treatment strategy and duration.