
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-098
A Challenging Case Report: Fenestration of a Papyrus PK Covered Stent to Rescue Jailed Left Circumflex Artery
By Jieli Kua, Poay-Huan Loh
Presenter
Jieli Kua Jieli Kua
Authors
Jieli Kua1, Poay-Huan Loh2
Affiliation
Ng Teng Fong Hospital, Singapore1, National University Heart Centre, Singapore2,
View Study Report
TCTAP C-098
CORONARY - Complications (Coronary)
A Challenging Case Report: Fenestration of a Papyrus PK Covered Stent to Rescue Jailed Left Circumflex Artery
Jieli Kua1, Poay-Huan Loh2
Ng Teng Fong Hospital, Singapore1, National University Heart Centre, Singapore2,
Clinical Information
Patient initials or Identifier Number
S
Relevant Clinical History and Physical Exam
67-year-old gentleman who is a non-smoker and works as a taxi driver. He has history of hypertension and hyperlipidemia and underwent angioplasty before in 2014. He presented to hospital initially for melena and was found to have a duodenal ulcer. During the same admission, he had recurrent episodes of chest pain with troponin suggestive of type 2 myocardial infarction. In view of his symptoms and risk factors, he was advised to undergo an invasive coronary angiogram.
Relevant Test Results Prior to Catheterization
Echocardiogram shows normal systolic function with regional wall motion abnormalities in RCA/LCx territory. No significant valvular abnormalities.
Relevant Catheterization Findings
Distal left main calcified severe 80% stenosis
Proximal LAD 70% stenosis1st diagonal 90% stenosisProximal circumflex 60% stenosis. Distal circumflex 90% stenosisProximal to distal RCA long diffuse 70 to 80% stenosis. Distal RCA focal 80% stenosis

Proximal LAD 70% stenosis1st diagonal 90% stenosisProximal circumflex 60% stenosis. Distal circumflex 90% stenosisProximal to distal RCA long diffuse 70 to 80% stenosis. Distal RCA focal 80% stenosis
Interventional Management
Procedural Step
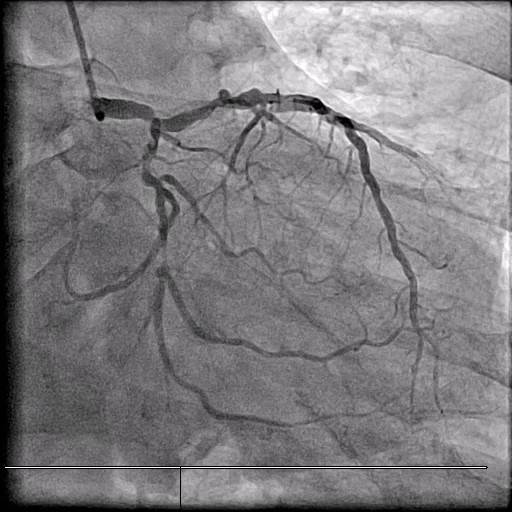
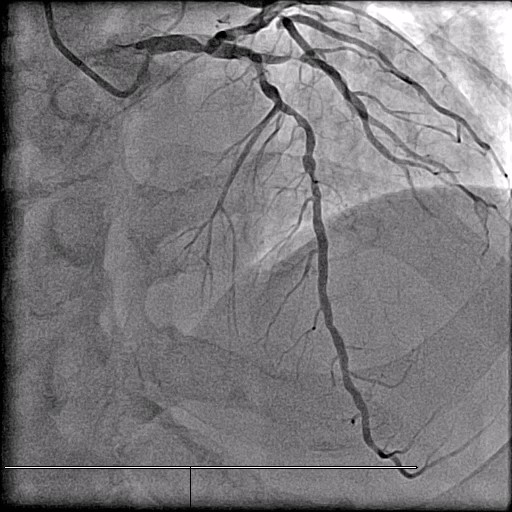
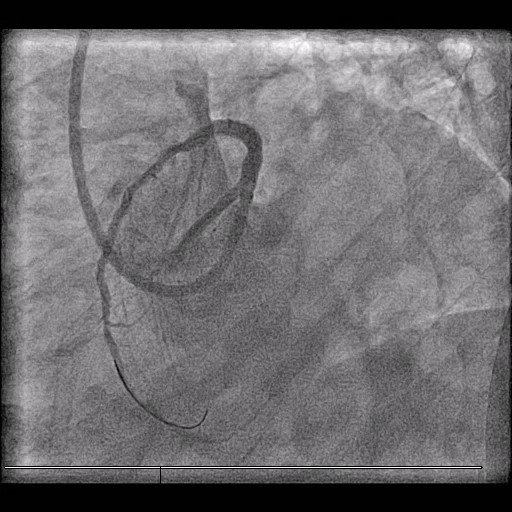
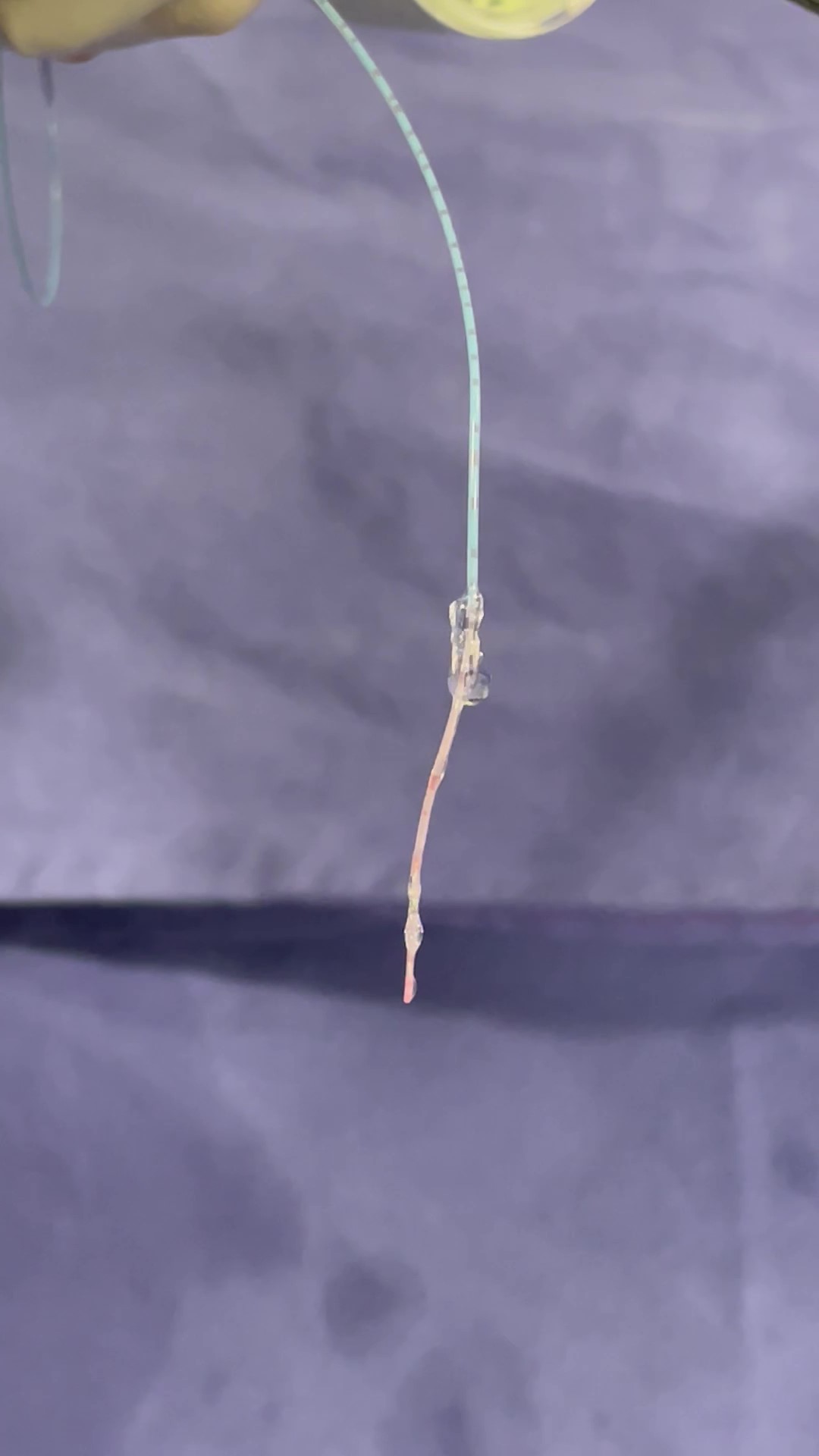
7 Fr EBU 3.5 guide catheter. 1.5 rotaburr with 9 runs at 160000 RPM to LM-LAD. Predilated along LM-LAD with 2.0 SC balloon.Unable to cross 1st diagonal with 2.0 SC balloon. 1.0 SC balloon inflated in 1st diagonal with intentional rupture at 22 atm (balloon assisted microdissection).Angiogram shows perforation. 3.0 SC balloon inflated in LAD proximal to diagonal did not seal perforation. Inflated across LM-LAD.3 x 26 mm Papyrus covered stent deployed across LM-LAD which managed to seal perforation.Post dilated in LAD with 3.5 NC and LM with 4.0 NC.Repeat angiogram shows jailed circumflex artery (Figure A)Jailed circumflex recrossed with Gaia 3rd wire fenestrating the papyrus covered stent (Figure B)Predilated with 1.5 SC and 2.0 SC balloon. Ostial circumflex treated with 2.0 x 15 mm drug coated balloon.mLAD stented with 2.5 x 38 mm DES stent and pLAD with 3 x 18 mm DES stent. Further post dilated with 3.5 NC balloon.Repeat angiogram shows ostial LCx recoil and poor flow despite repeated ballooning. Patient very symptomatic.2.5 x 12 mm DES stent was deployed in ostial LCx (T with minimal protrusion).Post dilated LM with 4.0 NC balloonChecking the ruptured 1.0 balloon after procedure shows rupture occurred in shaft of device and not at the balloon (Figure C). The force likely was directed towards LM-LAD causing the perforation in LM-LAD and not diagonal.

Case Summary
Patient was sent to ICU and remained stable. Repeat echocardiogram shows severe left ventricular systolic dysfunction. He was referred to the heart failure clinic for further optimisation of medications.