
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-001
Occlusive Explosion
By Saravanan Pillai, Faizal Khan Bin Abdullah, Kim Fong Ng, Asri Ranga
Presenter
Kim Fong Ng
Authors
Saravanan Pillai1, Faizal Khan Bin Abdullah2, Kim Fong Ng3, Asri Ranga2
Affiliation
Hospital Serdang, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, Sultanah Aminah Hospital, Malaysia3,
View Study Report
TCTAP C-001
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Occlusive Explosion
Saravanan Pillai1, Faizal Khan Bin Abdullah2, Kim Fong Ng3, Asri Ranga2
Hospital Serdang, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, Sultanah Aminah Hospital, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Arry
Relevant Clinical History and Physical Exam
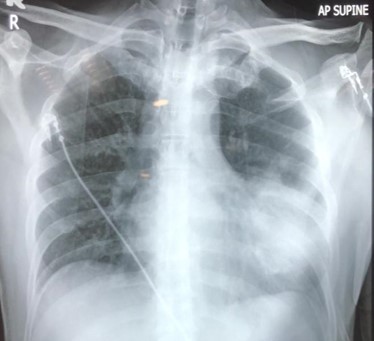
47yr old man, suffered a blast injury at the workplace after an O2 tank exploded while he was transferring liquid gas into a tank for welding purposes. The impact has caused him to temporary loss of consciousness. Upon awakening, he had severe chest pain associated with shortness of breath. On examination, superficial partial thickness injury on the chest wall, and lungs: reduced breath sound bi-basally, no murmur heard. BP:106/77mmHg, HR:100/min, SPO2 100% on HFM 15L/min.

Relevant Test Results Prior to Catheterization
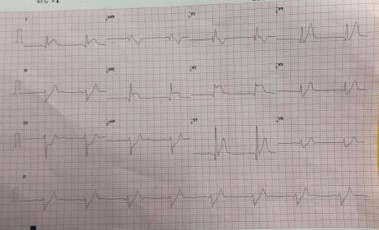
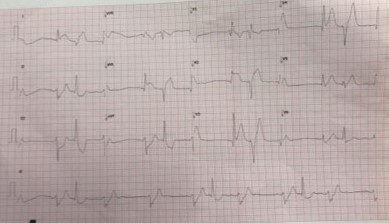
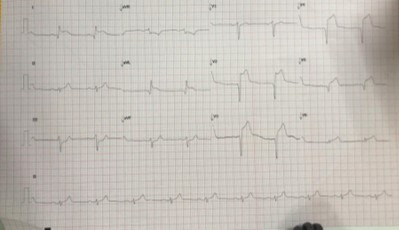
Serial ECGs were done and showed dynamic changes in the anterior leads Bedside echo before invasive coronary angiograms shows mild LVSD, normal valves, and no pericardial effusion
Relevant Catheterization Findings
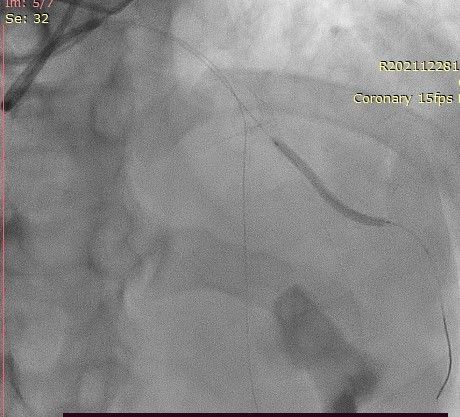
Right radial approach6F systemOpitorque catheter for diagnostic angiogramLMS: smoothLAD: ATO mid LAD, DG1 prox ATOLCx: smoothRCA: smooth
Impression: ATO to LAD and Diagonal 1( Dual ATO)
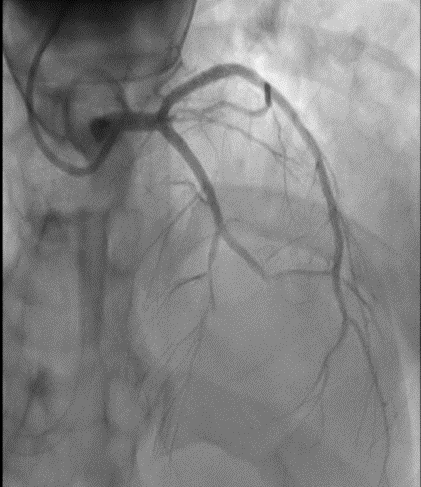
Impression: ATO to LAD and Diagonal 1( Dual ATO)
Interventional Management
Procedural Step
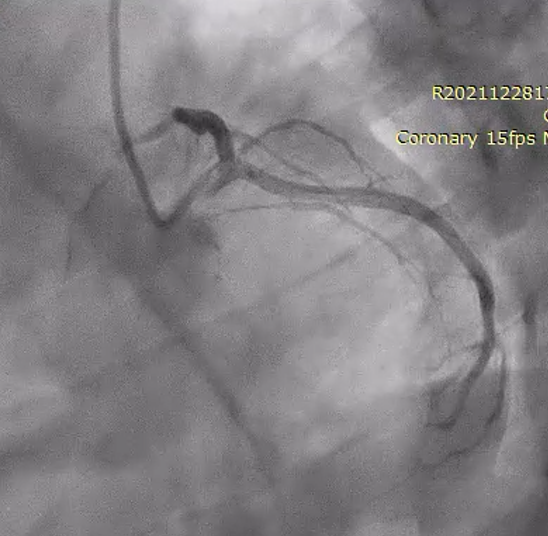
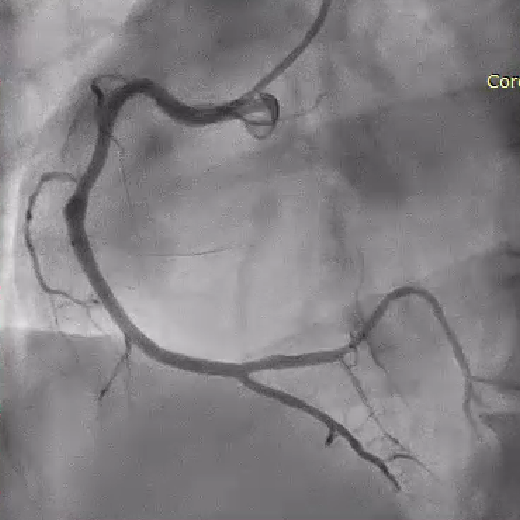
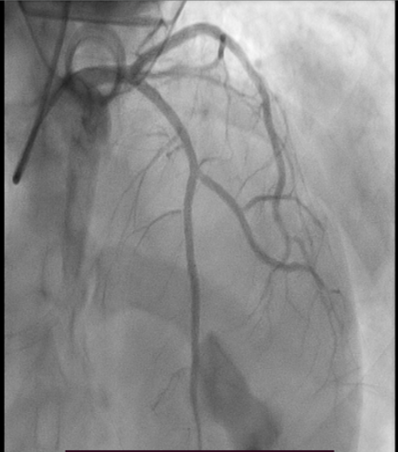
Right radial coronary angiogram via 6F systemEBU 3.0 engaged with good supportSion blue wired into LAD, export catheter delivered, and aspirated red thrombusPre-dilated with Sapphire 3 SC 2.5x15mm @ 6-10ATMFlow established in LAD, however, decided to interrogate DG1 as it shows ATOBMW wired into the DG1 and pre-dilated with Sapphire 3 SC 2.0x15mmNoted nonflow limiting dissection and decided to stent DG1 with 2.25x34mm@12ATM, dissection sealed and TIMI III flow establishedStented mid LAD with 2.5x30mm @12ATM just before LAD/DG1 bifurcation, then stented proximal LAD with 2.5x 26mm@ 12ATM.Post-dilated LAD with 2.75x15mm@ 14-20ATMTIMI II-III flowIV Tirofiban has been given a loading dose due to a high thrombus burden and sluggish flow
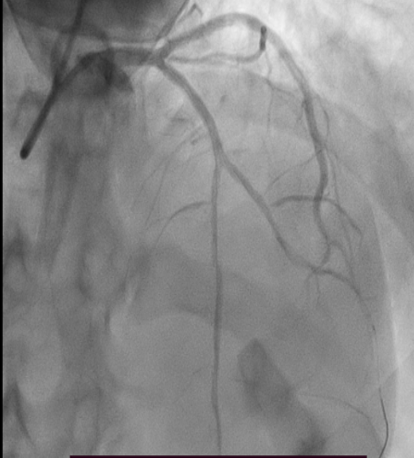
Case Summary
Myocardial infarction is a rare complication of blunt chest trauma. This case demonstrates how blast shock waves result in the dissection of the coronary vessel leading to total occlusion of the two vessels. It also promotes red thrombus within the coronary vessels. Percutaneous coronary intervention is the most suitable way to treat this condition. Intravascular imaging such as IVUS or OCT would be beneficial to demonstrate the physiology behind this MI and would also be helpful in planning and optimizing the lesions. Unfortunately, intravascular imaging was not used for this patient to reduce procedural time as he was treated during the height of the COVID pandemic.