
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-064
Mini-Crush Technique and Imaging Guided Bifurcation Stenting in Complex Percutaneous Coronary Intervention : Less Steps but Feasible
By Koon Wee Koay, Jian-Chen Lim, Ho Lam, Ping Wa Yam
Presenter
Koon Wee Koay
Authors
Koon Wee Koay1, Jian-Chen Lim2, Ho Lam3, Ping Wa Yam3
Affiliation
Penang General Hospital, Malaysia1, Hospital Serdang, Malaysia2, Tuen Mun Hospital, Hong Kong, China3,
View Study Report
TCTAP C-064
CORONARY - Bifurcation/Left Main Diseases and Intervention
Mini-Crush Technique and Imaging Guided Bifurcation Stenting in Complex Percutaneous Coronary Intervention : Less Steps but Feasible
Koon Wee Koay1, Jian-Chen Lim2, Ho Lam3, Ping Wa Yam3
Penang General Hospital, Malaysia1, Hospital Serdang, Malaysia2, Tuen Mun Hospital, Hong Kong, China3,
Clinical Information
Patient initials or Identifier Number
Mr CS
Relevant Clinical History and Physical Exam
58 years old gentleman with no previous medical history presented to emergency department with complain of chest pain for 2 days associated with sweating. Upon arrival, his blood pressure was 134/80 mmHg, pulse rate was 102 beats per minute and oxygen saturation was 98% under room air. Physical examination was normal and he was not in heart failure.
Relevant Test Results Prior to Catheterization
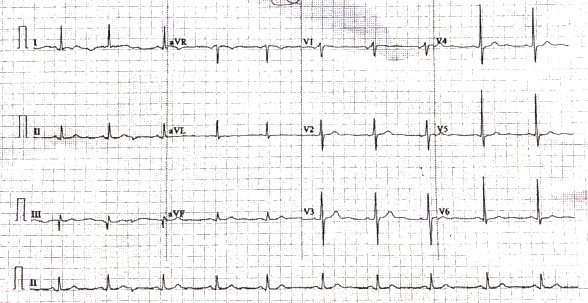
Electrocardiogram showed sinus rhythm with Q wave at lead III. Echocardiogram showed left ventricular ejection fraction of 45% with hypokinesia at anteroseptal, anterolateral and inferior wall. His hemoglobin and renal function were normal. His cardiac troponin I was 27000 ng/L and creatine kinase was 1140 u/L. He was treated as NSTEMI and was planned for cardiac catheterization.
Relevant Catheterization Findings
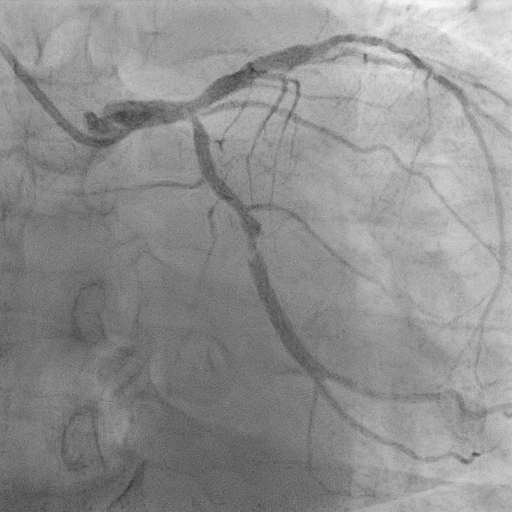
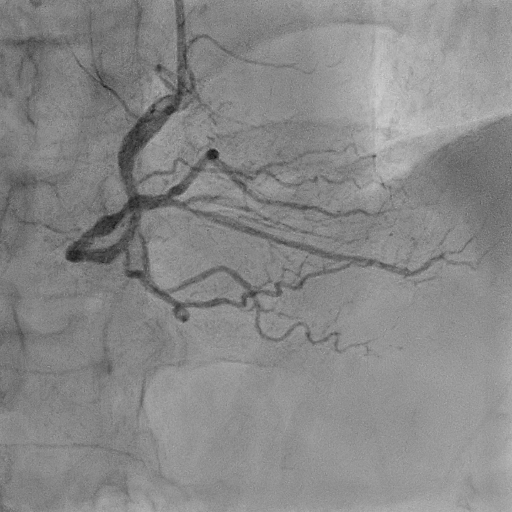
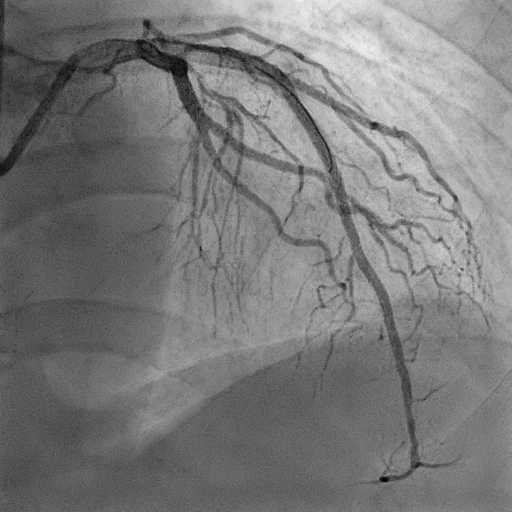
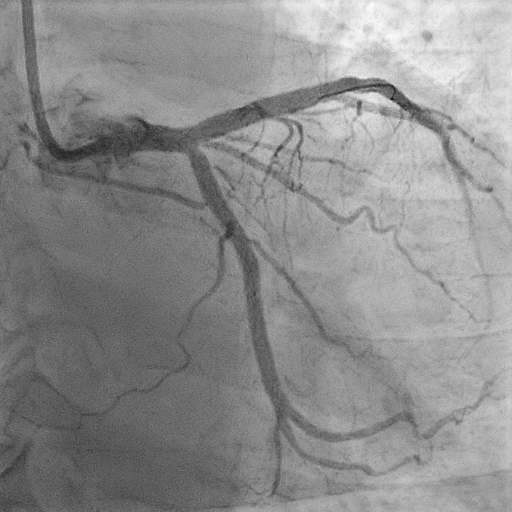
Coronary angiogram showed a 40% stenosis at distal left main and diffuse disease of 80% stenosis from proximal to distal left anterior descending (LAD) artery with bifurcation lesion at mid-LAD and first Diagonal branch (D1). There was also 80% stenosis at ostial left circumflex artery (LCX) and mid-LCX. Right coronary artery (RCA) was a dominant system with moderate disease at mid-RCA and 70% stenosis at distal-RCA. Patient refused option of bypass surgery and opted for multivessel PCI.

Interventional Management
Procedural Step
Procedure was done via 7F radial sheath. 6F JR4 was used to engage RCA. Distal-RCA was direct stented with Synergy XD 3.0/24 mm and postdilated with NC Emerge 3.5mm. For left system, 2-stents strategy by Mini-crush technique was planned for both bifurcation lesion at LM/LAD/LCX and LAD/D1. 7F EBU 3.5 guiding catheter was used. IVUS assessment was done at each vessel. Mid till distal-LAD was stented with Synergy XD 2.25/38 mm after lesion preparation. D1 was stented with Xience Skypoint 2.0/28 mm with minimal protrusion to LAD, optimized and crushed with NC Emerge 3.0 mm. Proximal LAD was then stented with Synergy XD 3.0/48 mm. LAD stents were optimized according to IVUS measured vessel size before rewiring to D1. Subsequently, sequential postdilatation was done to both LAD/D1 and kissing balloon inflation (KBI) was done with NC Emerge 2.0 mm at D1 and NC Emerge 3.0 mm at LAD. LCX was prepared with NC Emerge 2.25 mm and stented with Synergy XD 3.0/38 mm at mid till distal LCX and another Synergy XD 3.5/16 mm at ostial-LCX with minimal protrusion to LM. Optimization of LCX stents was done and crushed by NC Emerge 4.0 mm at LM. Ostial LM was stented with Synergy XD 4.5/8 mm and overlap with LAD stent. Rewiring was done to LCX after proximal optimization (POT) of LM with NC Emerge 4.5 mm. Sequential postdilatation was done to ostial-LCX with Raiden 3.5 mm and ostial-LAD with Raiden 4.0 mm and then KBI to both branches. Finally, LM was POT again with NC Emerge 4.5 mm.

Case Summary
This case is a triple vessel disease which involve 2 bifurcation lesion at LM/LAD/LCX and LAD/D1. As both D1 and LCX are heavily disease, upfront 2-stent strategy was planned for both bifurcation lesion. Mini-crush technique was used for both bifurcation lesion in this patient as it has less steps, less procedural time and able to achieve minimal metal layer overlapped at the carina. IVUS assessment pre and post procedure are crucial to ensure precise stent sizing, good stent apposition and expansion for bifurcation stenting. Sequential dilatation at both ostial branches, final KBI and final POT are vital steps to obtain a good result and thus reduce the risk of in-stent restenosis in future.