
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-037
Orbitotripsy in Emergent PCI: The Combined Use of Orbital Atherectomy and Intravascular Lithrotripsy for Heavily Calcified Coronary Lesions in a Patient Presented With Acute ST-Segment Elevation Myocardial Infarction
By Siu Fung Wong, Chun Yue Mui, Tak-Shun Chung
Presenter
Siu Fung Wong
Authors
Siu Fung Wong1, Chun Yue Mui2, Tak-Shun Chung2
Affiliation
Royal Sussex County Hospital, United Kingdom1, United Christian Hospital, Hong Kong, China2,
View Study Report
TCTAP C-037
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Orbitotripsy in Emergent PCI: The Combined Use of Orbital Atherectomy and Intravascular Lithrotripsy for Heavily Calcified Coronary Lesions in a Patient Presented With Acute ST-Segment Elevation Myocardial Infarction
Siu Fung Wong1, Chun Yue Mui2, Tak-Shun Chung2
Royal Sussex County Hospital, United Kingdom1, United Christian Hospital, Hong Kong, China2,
Clinical Information
Patient initials or Identifier Number
MPP
Relevant Clinical History and Physical Exam
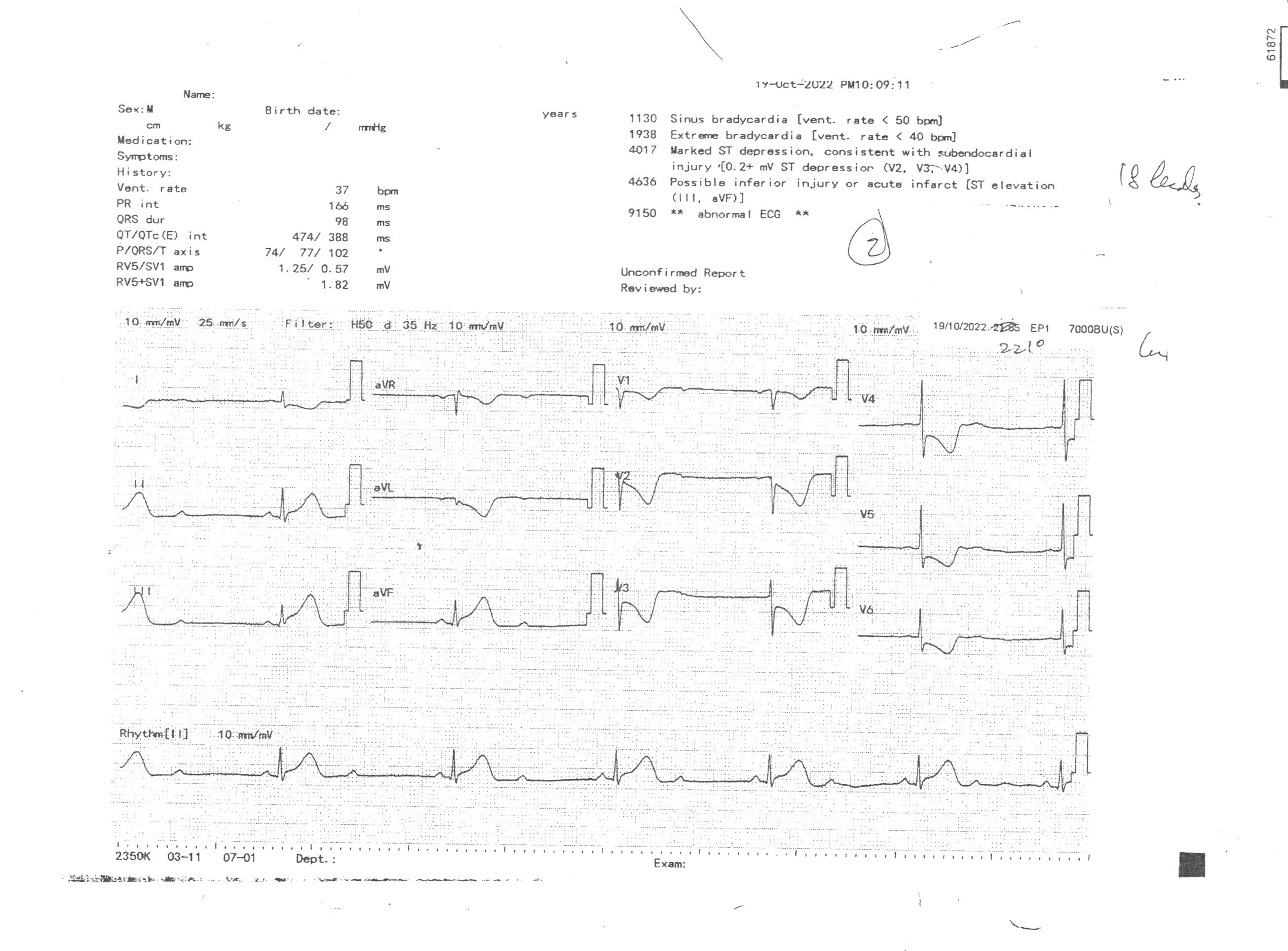
A 76 years old man presented with sudden onset of retrosternal chest pain at night after dinner, followed by an episode of loss of consciousness. He was a chronic smoker and suffered from stroke many years ago. He was immediately sent to hospital an hour after the onset of chest pain. On arrival he was hypotensive and developed bradycardia. Physical examination was unremarkable otherwise. ECG showed 2:1 2nd degree heart block with ST-segment elevation on leads 2, 3 and aVF.
Relevant Test Results Prior to Catheterization
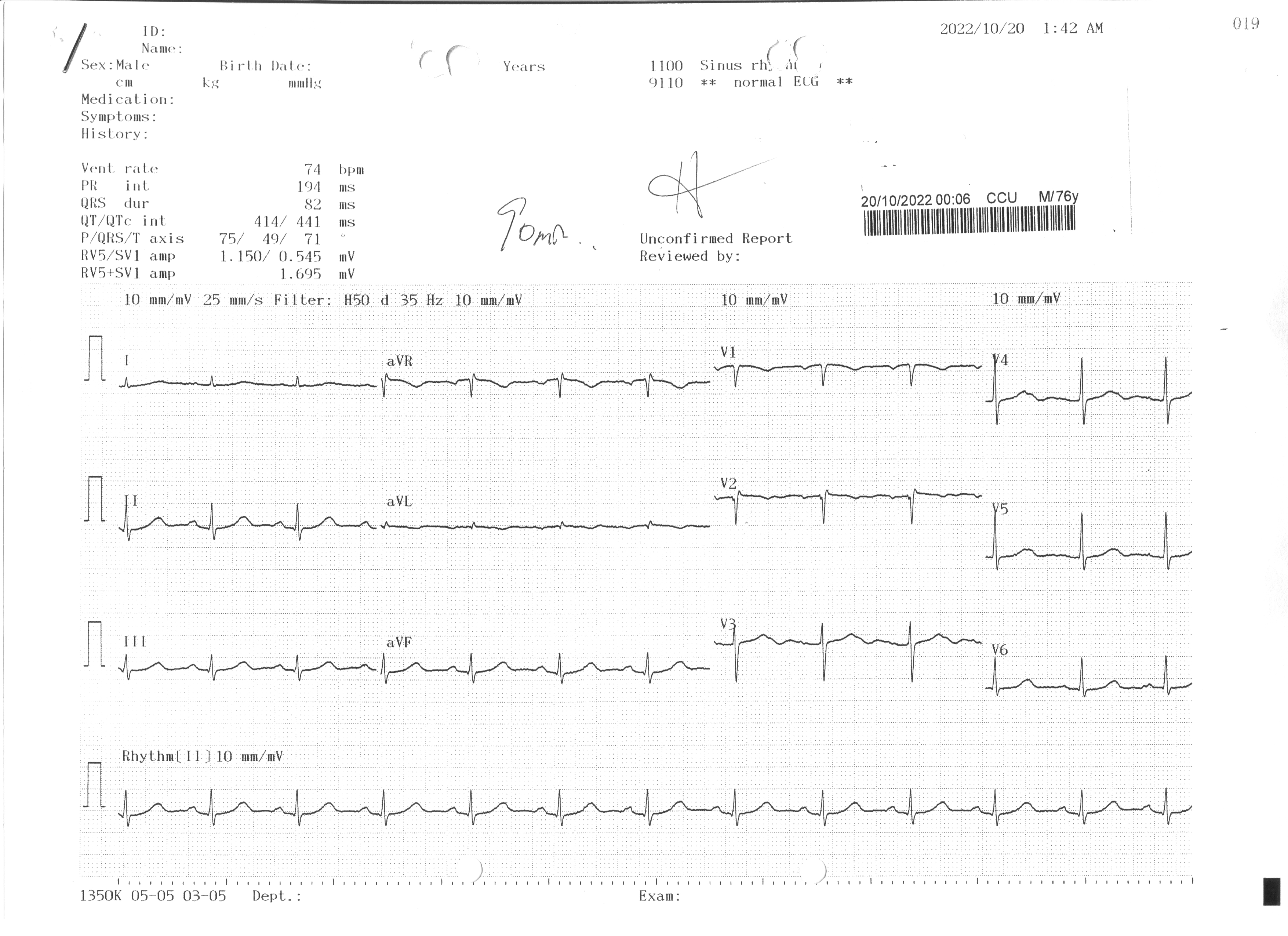
Atropine was given with resolution of heart block. As emergent percutaneous coronary intervention was not available outside office hours in the current regional hospital, thrombolytic was given, followed by signs of successful reperfusion. The patient was subsequently taken over to CCU for close monitoring and was prepared for emergent PCI at its earliest availability.
Relevant Catheterization Findings
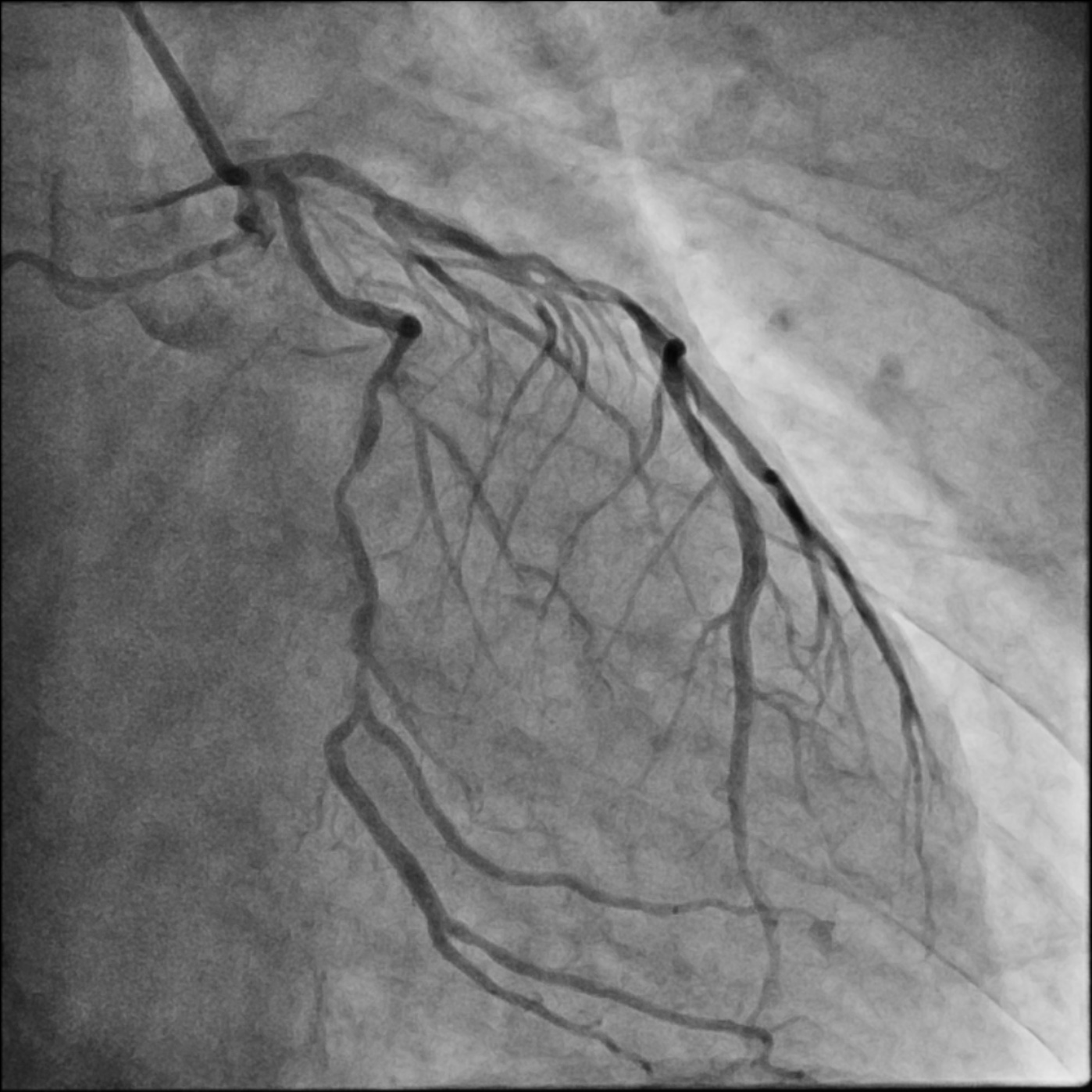
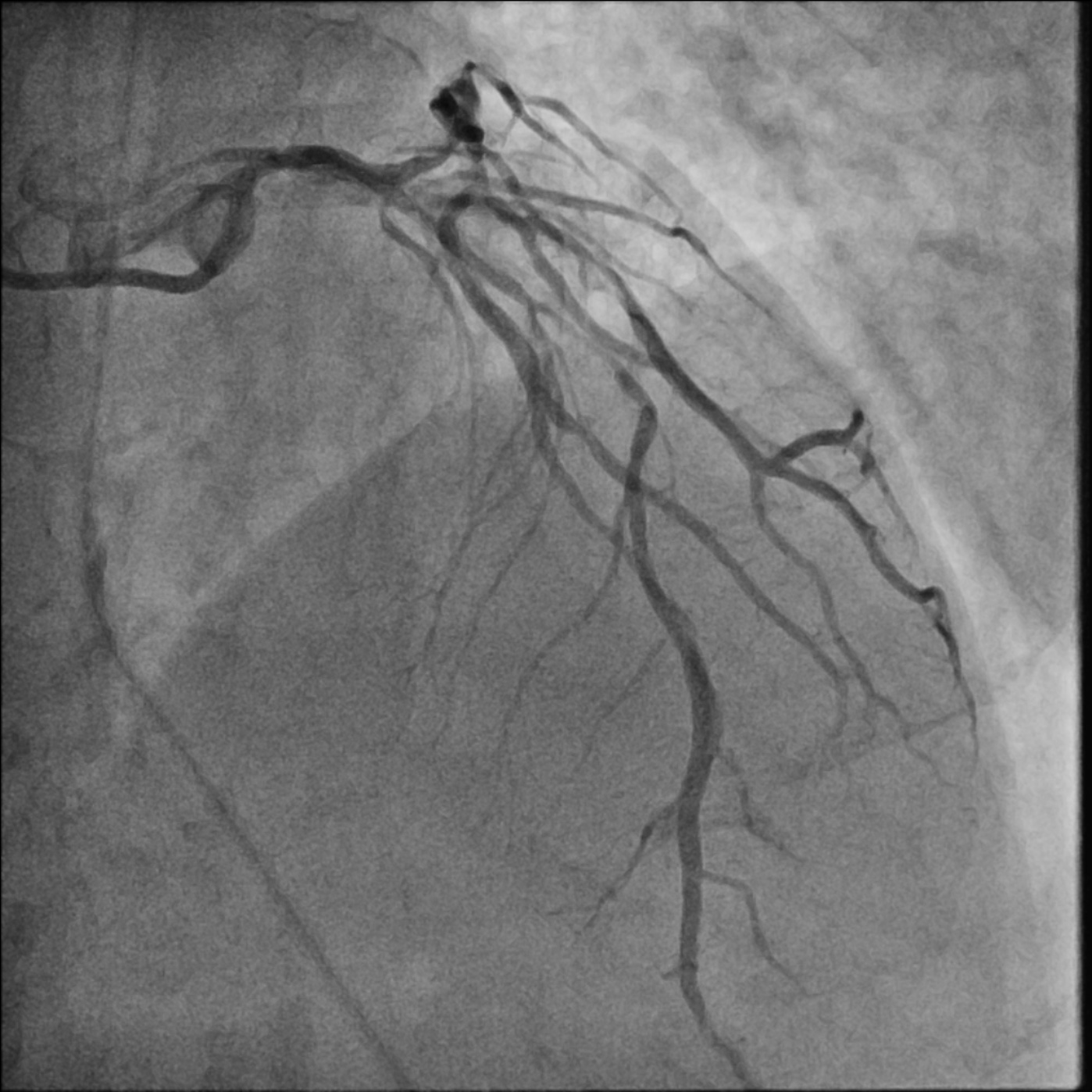
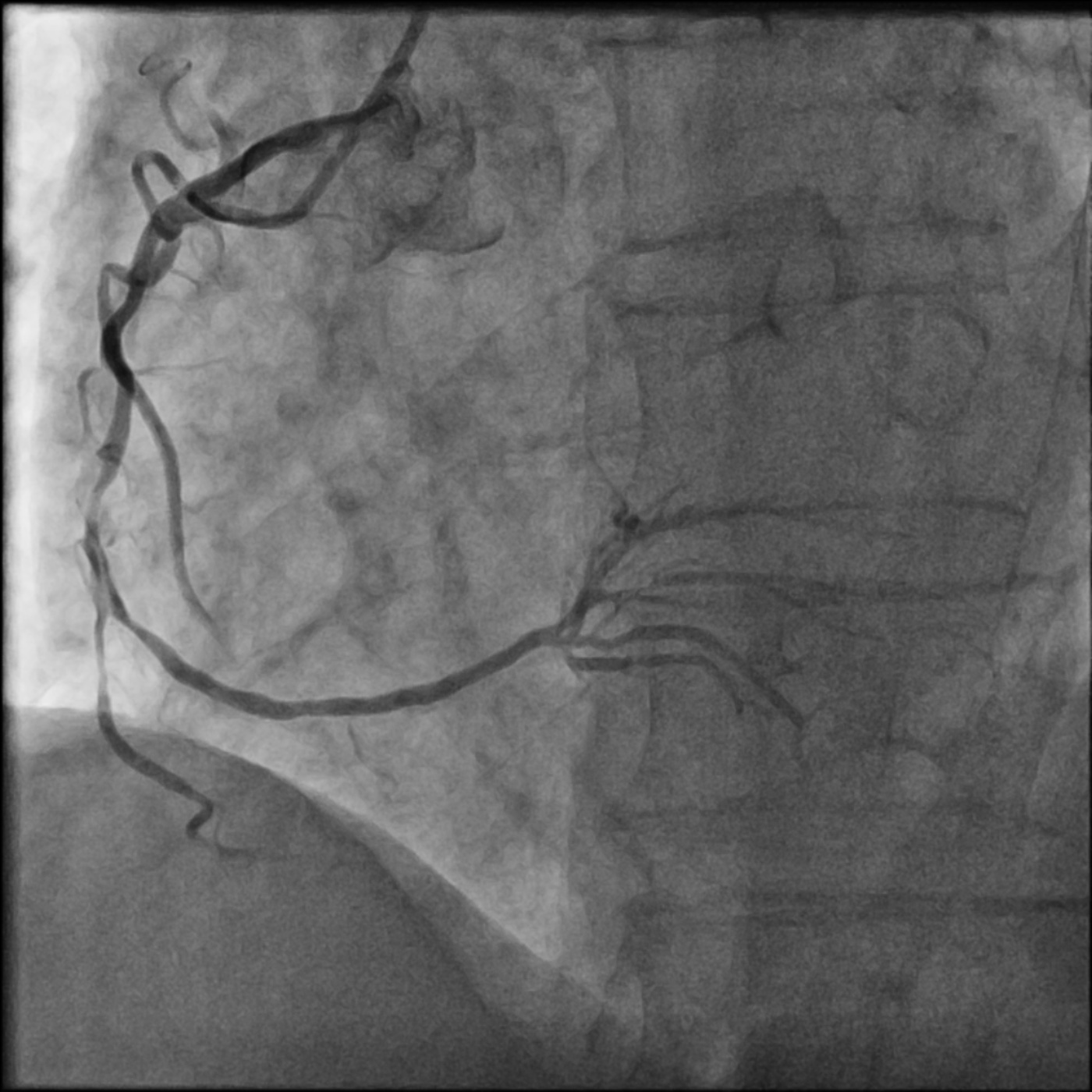
Coronary angiogram showed heavily calcified coronary vessels, with diffuse severe left main stem and triple vessel disease. Because of the advanced age of the patient and the lack of emergency CABG service, emergent PCI was performed for the culprit right coronary artery disease.
Interventional Management
Procedural Step
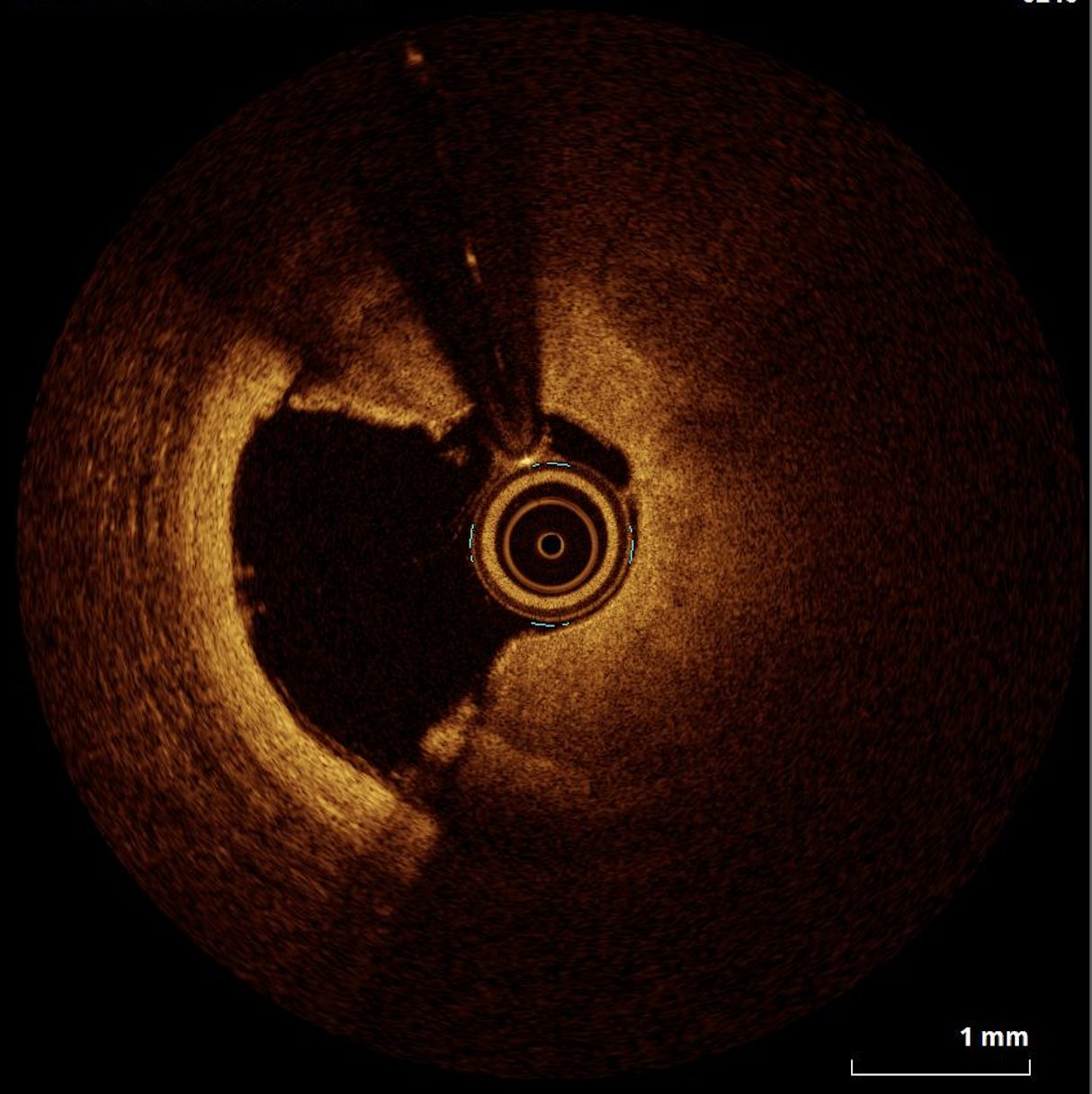
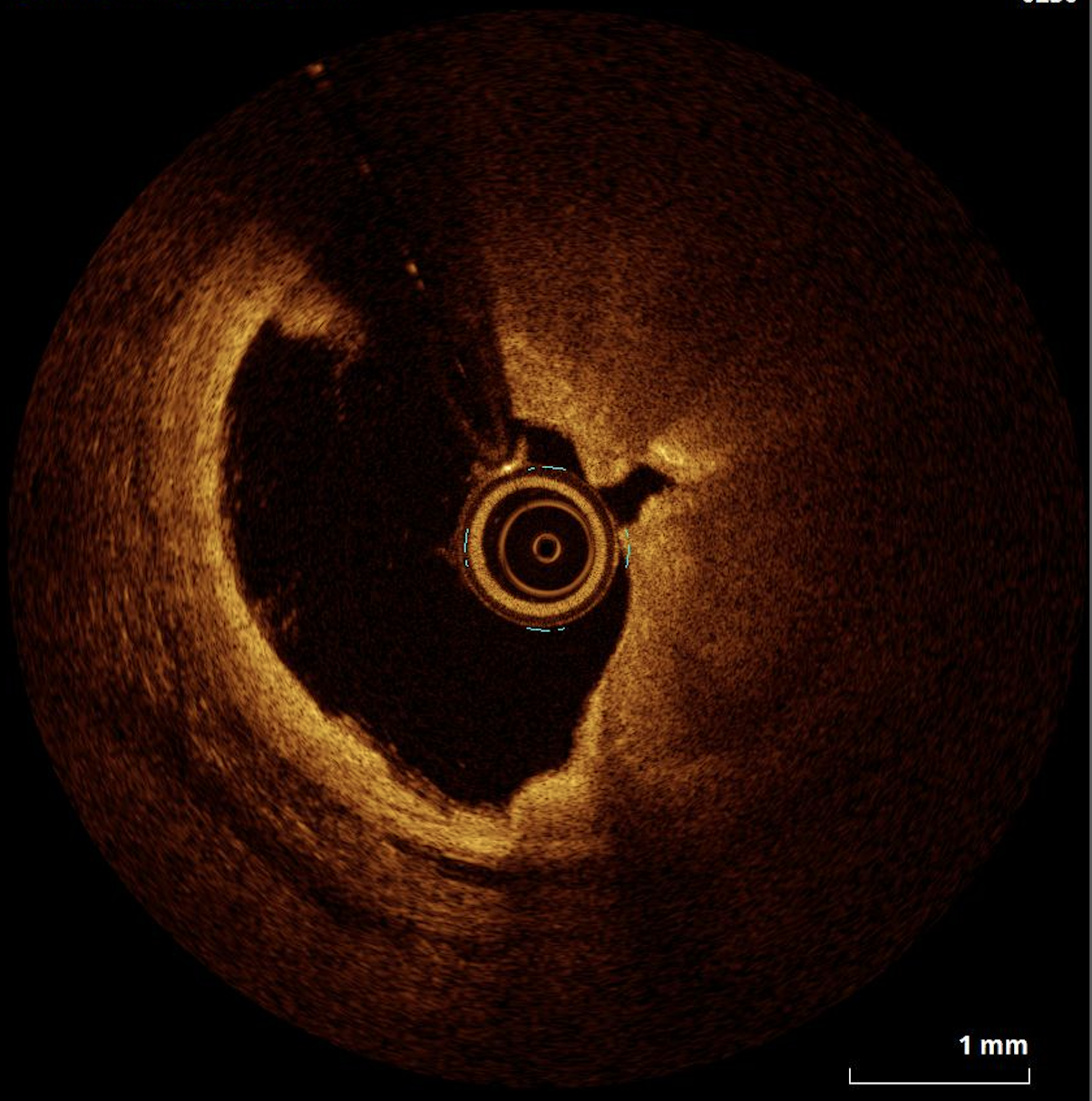
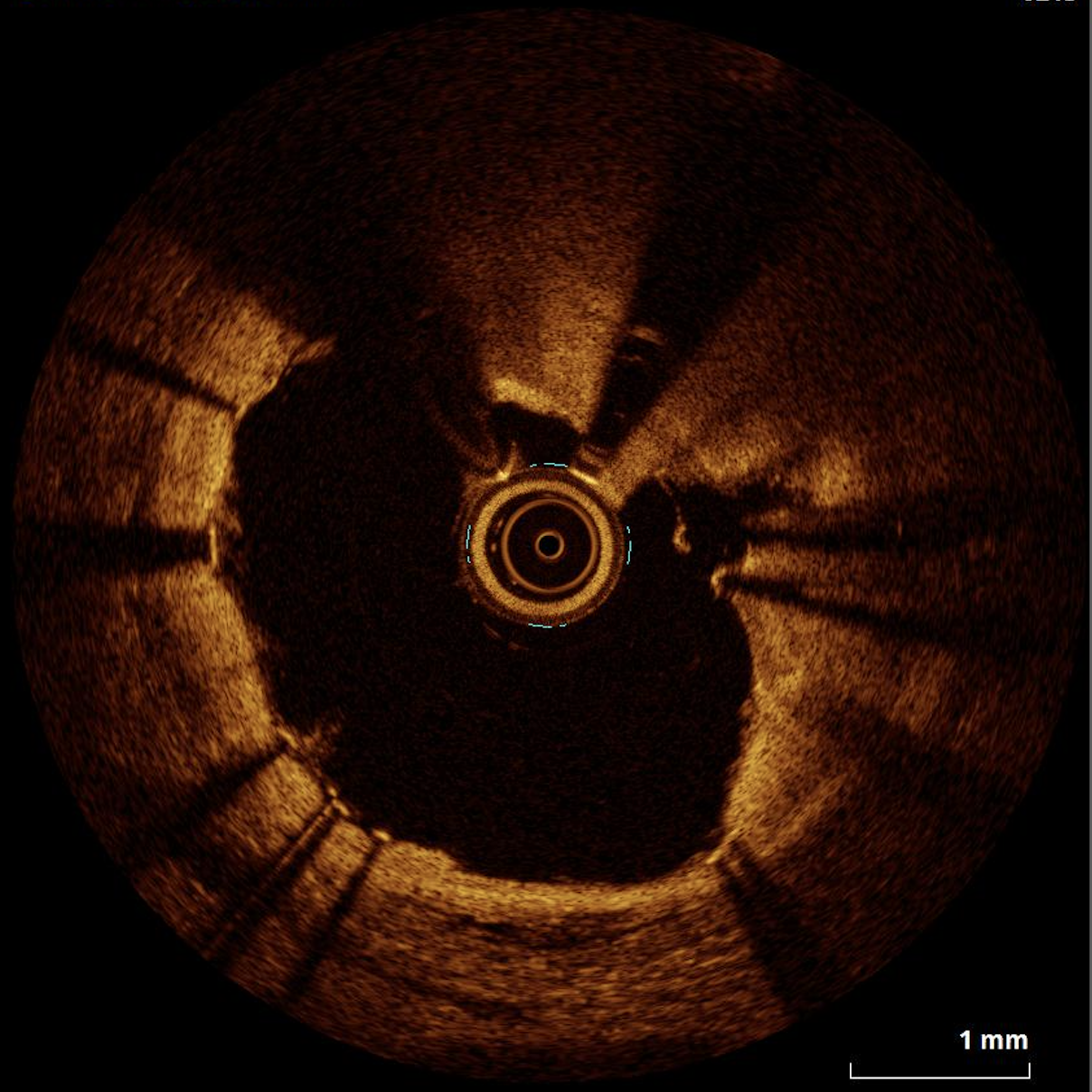
With a 6 Fr Launcher (Medtronic, US) AL. 75 guiding catheter. The critical mid RCA lesion was crossed with Runthrough Floppy (Terumo, Japan) guidewire and predilated with a 2.0 semi-compliant balloon. The diffuse RCA lesion was then interrogated with OCT (Abbott, US). It showed, from proximal to distal RCA, diffuse eccentric calcification up to 300 degrees arc and 1.5 mm thick. Upfront orbital atherectomy was decided for modification of the calcium plate. The Runthrough floppy (Terumo, Japan) guidewire was changed to a ViperWire (CSI, US). Orbital atherectomy was performed at 80,000 rpm for 3 runs and then 120,000 rpm for 5 runs. There was an episode of slow flow improved with administration of intracoronary adrenaline and sodium nitroprusside. Repeated OCT (Abbott, US) showed evidence of calcium ablation. For fear of the risk of further slow flow, a 3.0 intravascular lithrotripsy (Shockwave medical, US) balloon was applied to the calcified lesion for 8 runs to further modify it, resulting in cracking of the calcium plate. An Orsiro 2.5/30mm stent (Biotronik, Germany) was deployed at mid to distal RCA while an overlapping Orsiro 3.5/35mm stent (Biotronik, Germany) was deployed at proximal to mid RCA. The stent was post dilated with 3.0 non-compliant balloon distally and 3.5 non-complaint balloon proximally up to 22 atm. The final OCT (Abbott, US) and angiographic results are satisfactory. TIMI 3 flow was achieved with good stent expansion and apposition.
Case Summary
Calcified coronary lesion is one of the most difficult-to-treat lesion subsets in the field of percutaneous coronary intervention. And its presence in emergency setting of acute myocardial infarction further increases procedural complexity and even patient's morbidity. Our case demonstrated the combination of orbital atherectomy and intravascular lithrotripsy is a safe and viable tool in treating this kind of lesion, achieving satisfactory modification of calcium for optimal stent implantation. Intravascular imaging is pivotal in every steps in management of this type of lesions from tissue characterisation, to procedural planning and stent optimisation.