
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-142
A Challenging Case of Simultaneous Transarterial Coil Embolization in the Treatment of Post-EVAR Endoleak
By Se Hun Kim, Joon Hyuk Kong
Presenter
Se Hun Kim
Authors
Se Hun Kim1, Joon Hyuk Kong1
Affiliation
Incheon Sejong Hospital, Korea (Republic of)1,
View Study Report
TCTAP C-142
ENDOVASCULAR - Aorta Disease and Intervention
A Challenging Case of Simultaneous Transarterial Coil Embolization in the Treatment of Post-EVAR Endoleak
Se Hun Kim1, Joon Hyuk Kong1
Incheon Sejong Hospital, Korea (Republic of)1,
Clinical Information
Patient initials or Identifier Number
I I C
Relevant Clinical History and Physical Exam
The patients suffered from coronary triple vessel disease and a history of an emergency coronary artery bypass grafting due to hemopericardium during percutaneous coronary intervention in 2004. She went subtotal gastrectomy operation in 2021 beacause of gastric cancer and she had a dyslipidemia.
Relevant Test Results Prior to Catheterization
Laboratory testing demonstrated a hemoglobin level of 12.7 g/dl (normal 12.0 - 15.0 mg/dl), creatinine level of 0.69 mg/dl (normal 0.40 - 0.90 mg/dl), a HbA1c level of 6.4 % (normal 4.0 - 6.0 %) and a LDL cholesterol level of 84 mg/dl (normal 40 - 130 mg/dl).

Relevant Catheterization Findings
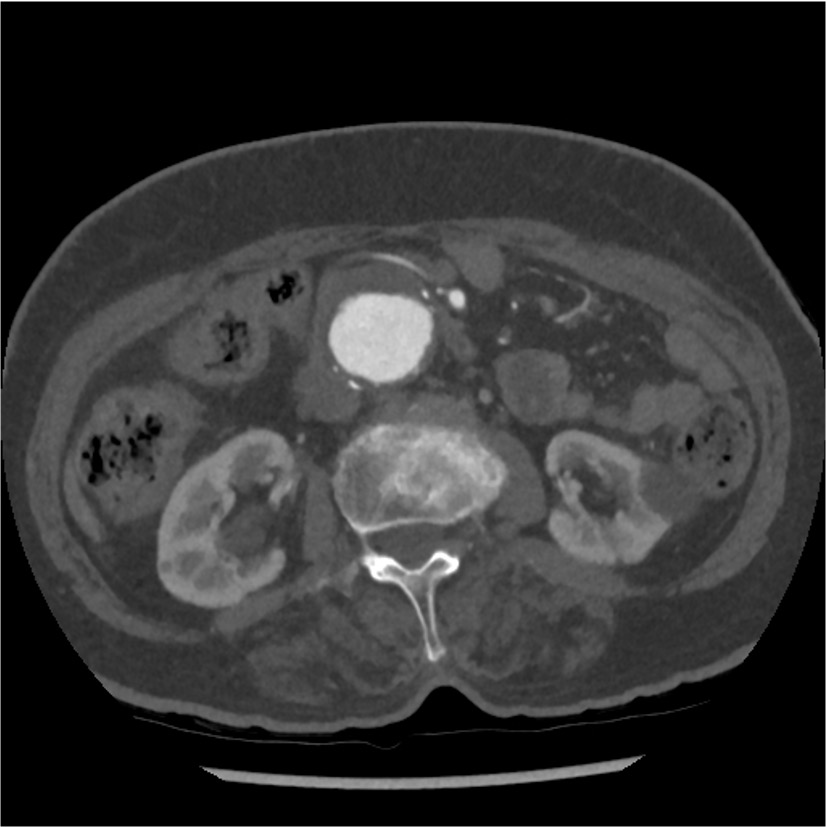
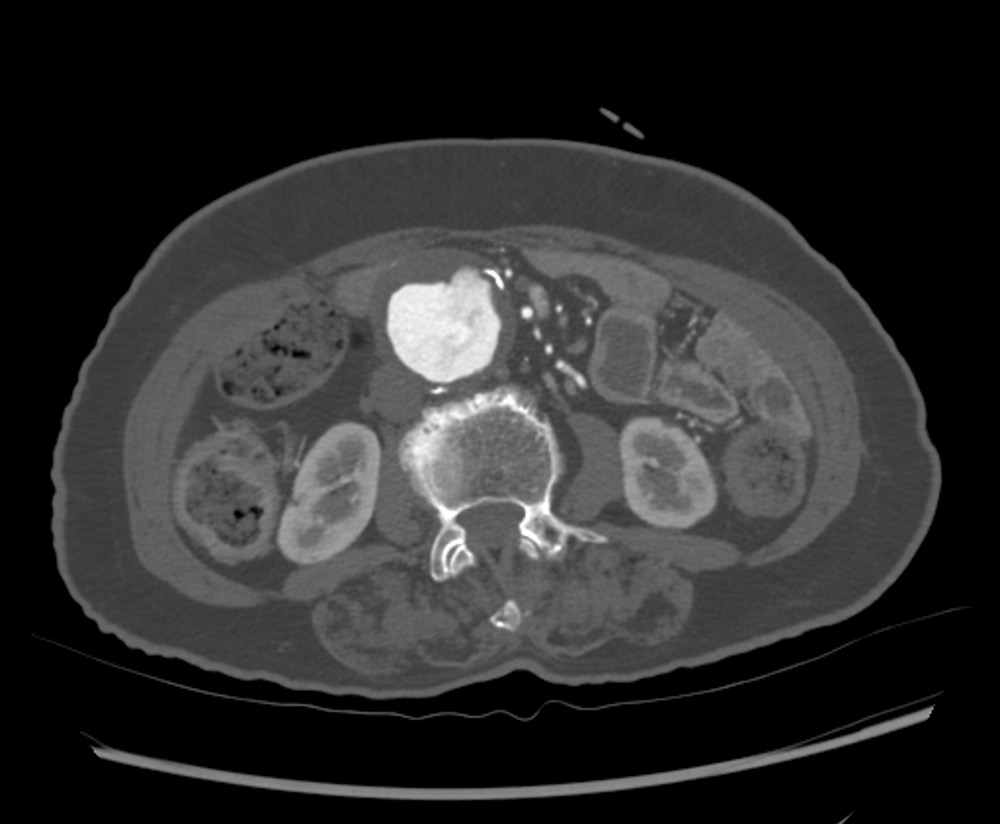
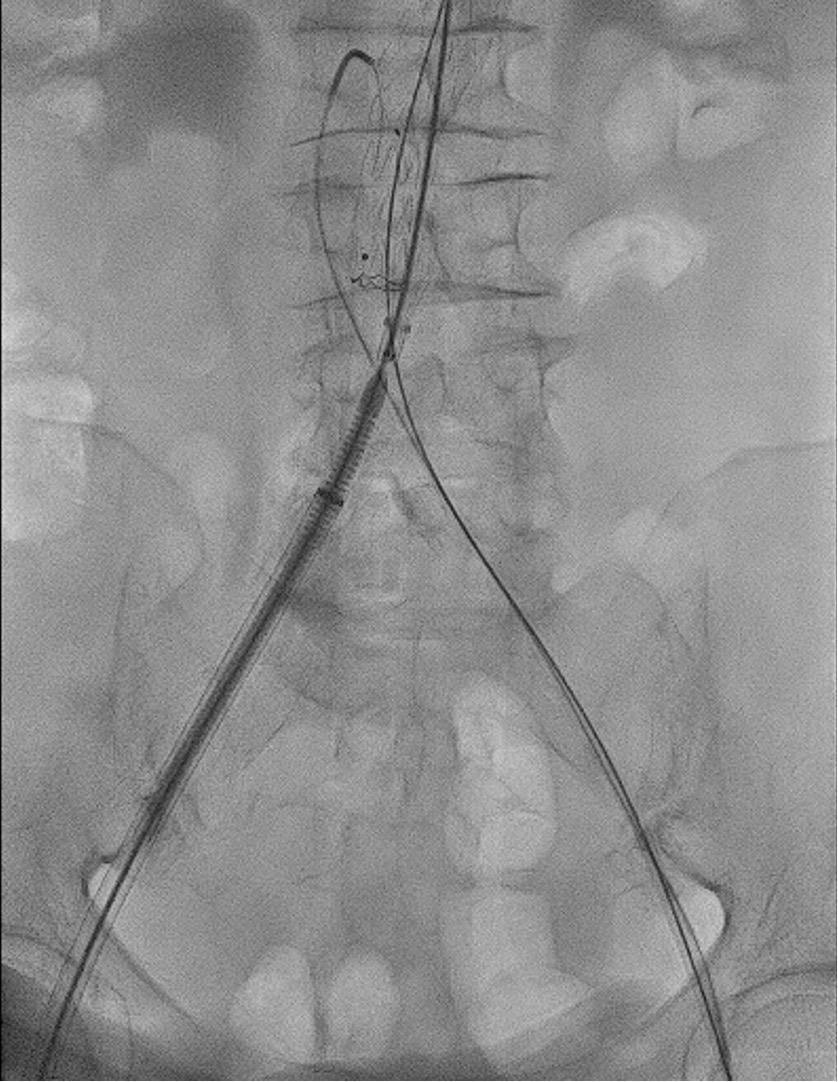
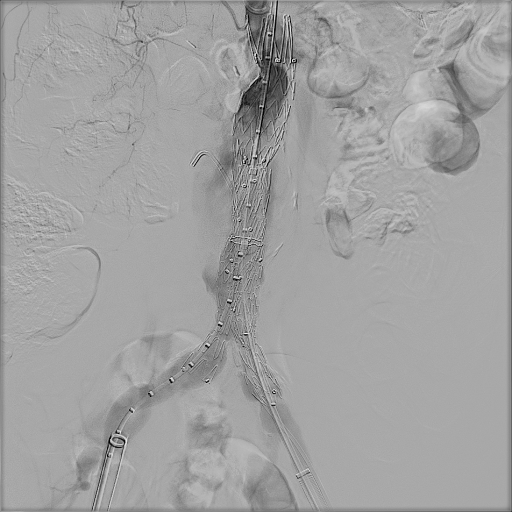
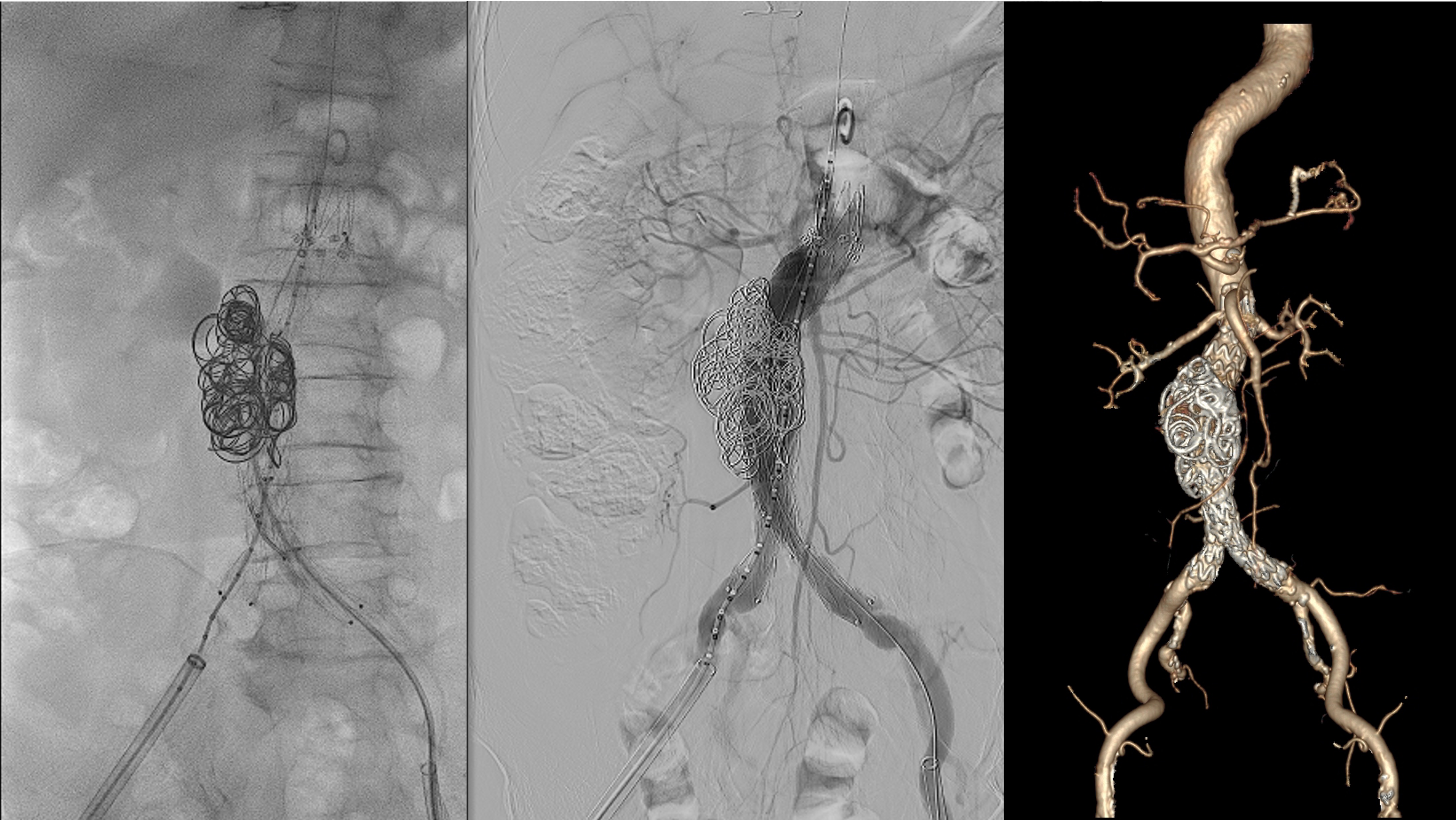
The bilateral femoral arteries were punctured and pre-closed with a perclose device. Baseline angiography revealed fusiform infrarenal aneurysm (Figure 4). We performed conventional EVAR main body implantation via the ipsilateral femoral artery. Before the contralateral limb implantation, a second vascular access was completed via the contralateral femoral artery and we positioned a 5Fr Cobra catheter tip in the middle portion of the aneurysmal sac in preparation of coil embolization (Figure 5).

Interventional Management
Procedural Step

Case Summary
The simultaneous coil embolization via percutaneous trans-femoral artery approach is a promising technique for treating persistent type I and II mixed type endoleak despite angioplasty with a compliant balloon and endoanchor proximal landing zone approximation therapy.