
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-165
Chronic Mesenteric Ischemia: Which One Is Culprit Vessel ?
By Ashwani Sharma
Presenter
Ashwani Sharma
Authors
Ashwani Sharma1
Affiliation
Fortis Escorts Hospital, India1,
View Study Report
TCTAP C-165
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular
Chronic Mesenteric Ischemia: Which One Is Culprit Vessel ?
Ashwani Sharma1
Fortis Escorts Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Mr. J
Relevant Clinical History and Physical Exam
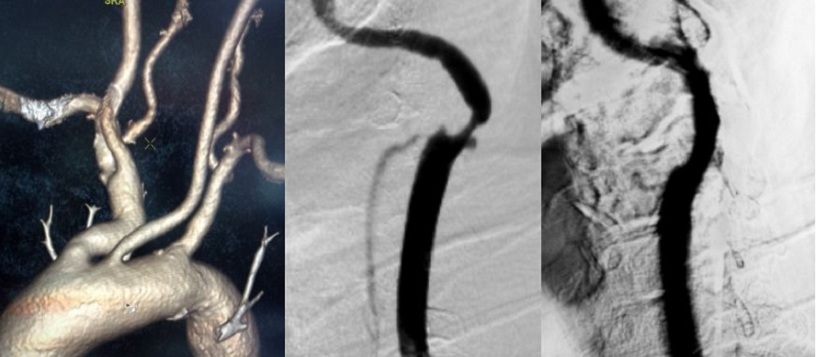
This elderly gentleman had right sided recurrent hemiparesis with slurring of speech. Brain imaging revealed multiple left frontal and parietal infarcts (all were TIAs). CT angiograpgy revealed left ICA 90% stenosis while 40-50% on right. Successful stenting was performed on left.
Relevant Test Results Prior to Catheterization
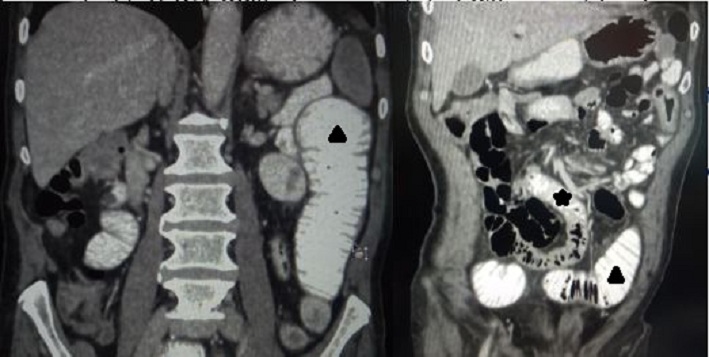
Also there was history of chronic mesenteric ischemia for 3- months. CECT abdomen revealed jejunal stricture with associated wall thickening (marked as solid black star) with dilated and laterally displaced proximal loops (solid black triangles).
Relevant Catheterization Findings
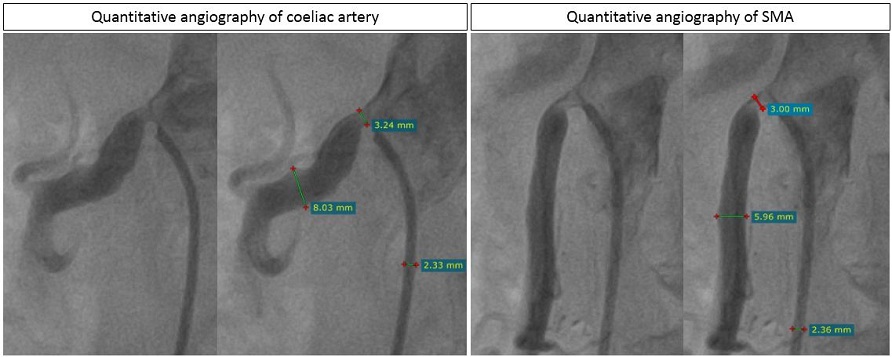
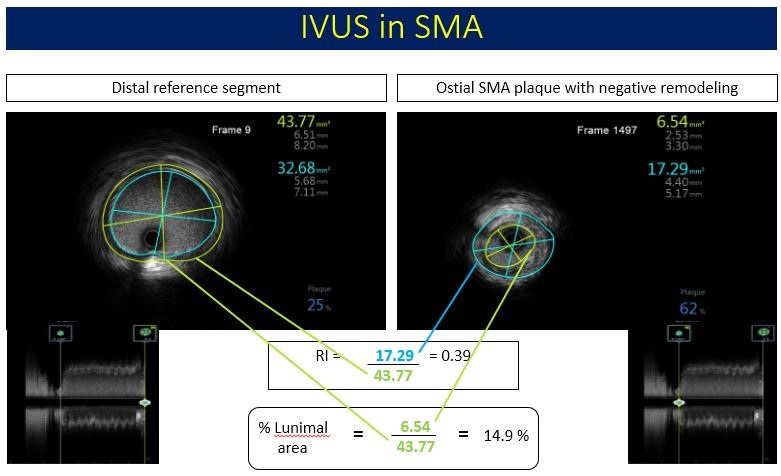
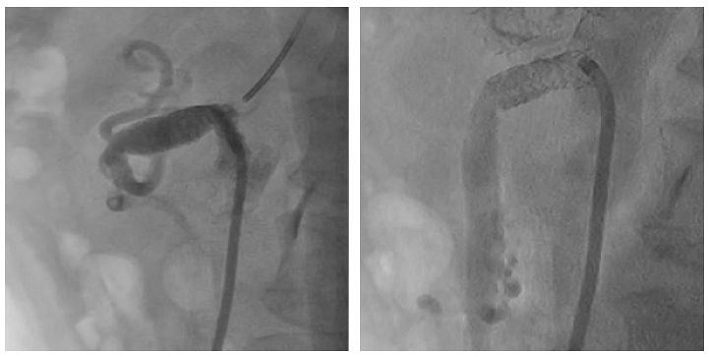
Angiography of the mesentric vessels revealed ostial 80% stenosis of coeliac trunk, ostial 40 - 50% stenosis of SMA while small sizes IMA had ostial 90% stenosis. The lesion in SMA was not explaining the presence of jejunal stricture. Hence, IVUS was performed in SMA which revealed significant ostioproximal calcified plaque with negative remedelling (Remodelling Index = RI = 0.39) and compare to normal reference segment the luminal area was 14.9% only.

Interventional Management
Procedural Step
Based upon IVUS, plan was drawn to stent the coeliac ans SMA while to manage the small IMA conservatively. Throught 8 F right transfemoral arterial access, after predilatation, 10 mm balloon expandable stent was deployed at ostioproximal Coeliac trunk. Postdilatation followed by flaring was performed. Then after predilatation, 7 mm balloon expandable stent was positioned in ostioproximal SMA and deployed. It was adequetely postdilated. There were good results in angiography as well as in IVUS. Second day patient had low hemoglobin without abdominal pain or local site hematoma. POCUS revealed left perinephric hematoma. CT angiography was performed which revealed no active bleed. Patient was managed conservatively with 2 unit PRBC transfusion. He was stabilized and discharged. He is absolutely symptom free and didn't required any further surgical management for stricture suggestive of functional stricture.
Case Summary
The given case exemplifies the value of clinical and image correlation. If jejunal stricture had not been considered during angiographic interpretation, most likely the stenting of coeliac and IMA would have been performed. Possibly the symptoms persisted and required surgical management. The IVUS helped a great in solving the puzzle and with due confidence stenting of IMA was omitted and stenting of SMA was performed.