
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-103
A Case of Coronary Artery Dissection and Perforation in a Severe Three Vessel Coronary Artery Disease With Chronic Total Occlusion
By Simeon Villangca, Patrick Nuique Vera Cruz, Myrtle Shekinah Lopez-Cayco, Glein Sayat, Ronald Santos, Alwyn Susanto, Francisco Dalangin
Presenter
Myrtle Shekinah Lopez-Cayco
Authors
Simeon Villangca1, Patrick Nuique Vera Cruz1, Myrtle Shekinah Lopez-Cayco1, Glein Sayat2, Ronald Santos1, Alwyn Susanto3, Francisco Dalangin1
Affiliation
St. Luke's Medical Center, Philippines1, St Luke's Medical Center, Philippines2, St Lukes Medical Center Quezon City, Philippines3,
View Study Report
TCTAP C-103
CORONARY - Complications (Coronary)
A Case of Coronary Artery Dissection and Perforation in a Severe Three Vessel Coronary Artery Disease With Chronic Total Occlusion
Simeon Villangca1, Patrick Nuique Vera Cruz1, Myrtle Shekinah Lopez-Cayco1, Glein Sayat2, Ronald Santos1, Alwyn Susanto3, Francisco Dalangin1
St. Luke's Medical Center, Philippines1, St Luke's Medical Center, Philippines2, St Lukes Medical Center Quezon City, Philippines3,
Clinical Information
Patient initials or Identifier Number
NM
Relevant Clinical History and Physical Exam
A 67-year old male, hypertensive, diabetic, came in for elective coronary angiogram. Patient is asymptomatic with normal resting echocardiogram but with abnormal stress test (>1.0 mm downsloping ST-segment depression in leads II, III, aVF, V3 to V6). He is a non-smoker, non-alcoholic beverage drinker and denies illicit drug use.Patient’s vital signs are within normal limits. He is overweight; body mass index of 27.8 kg/m2. Physical examination is unremarkable.
Relevant Test Results Prior to Catheterization
ECHOCARDIOGRAM
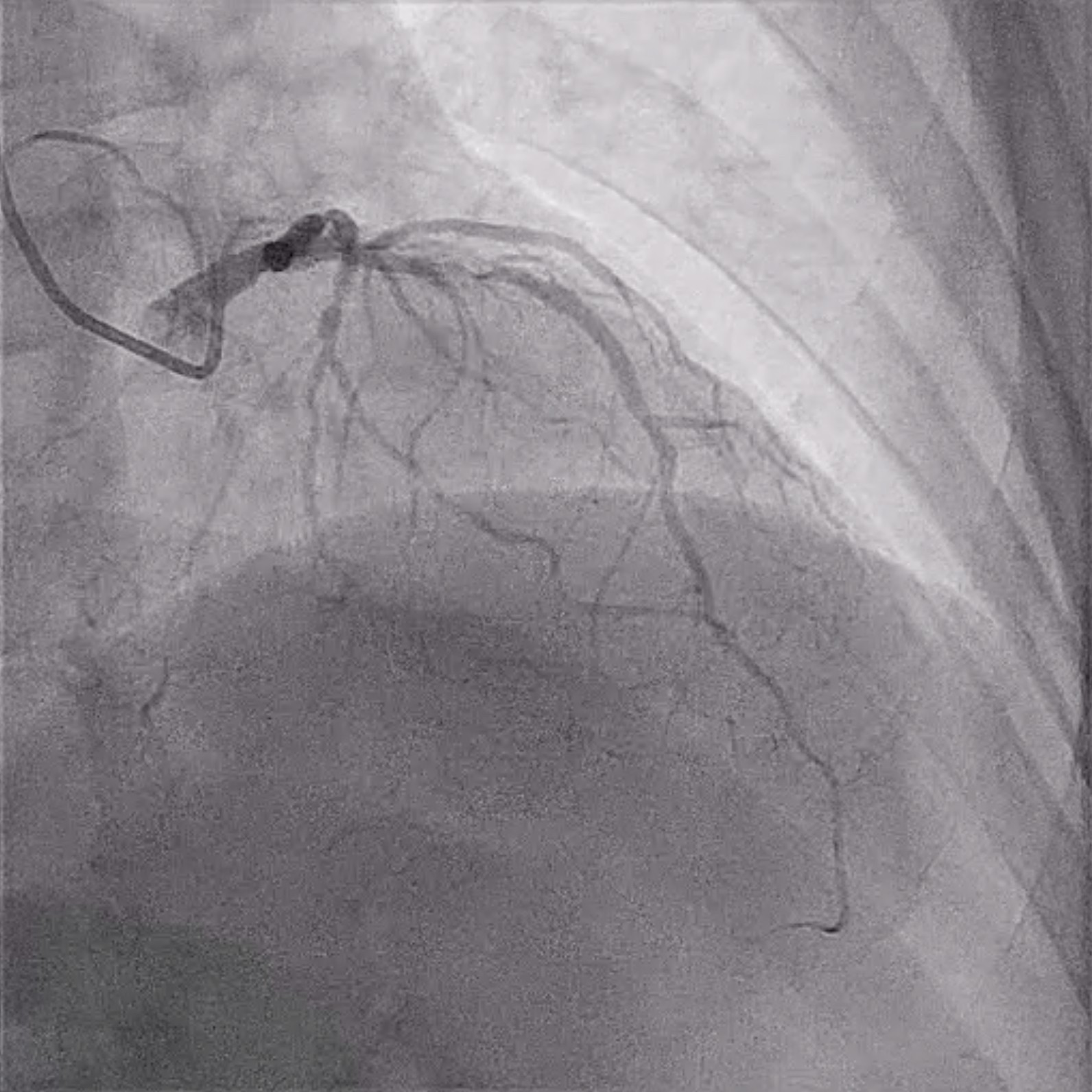
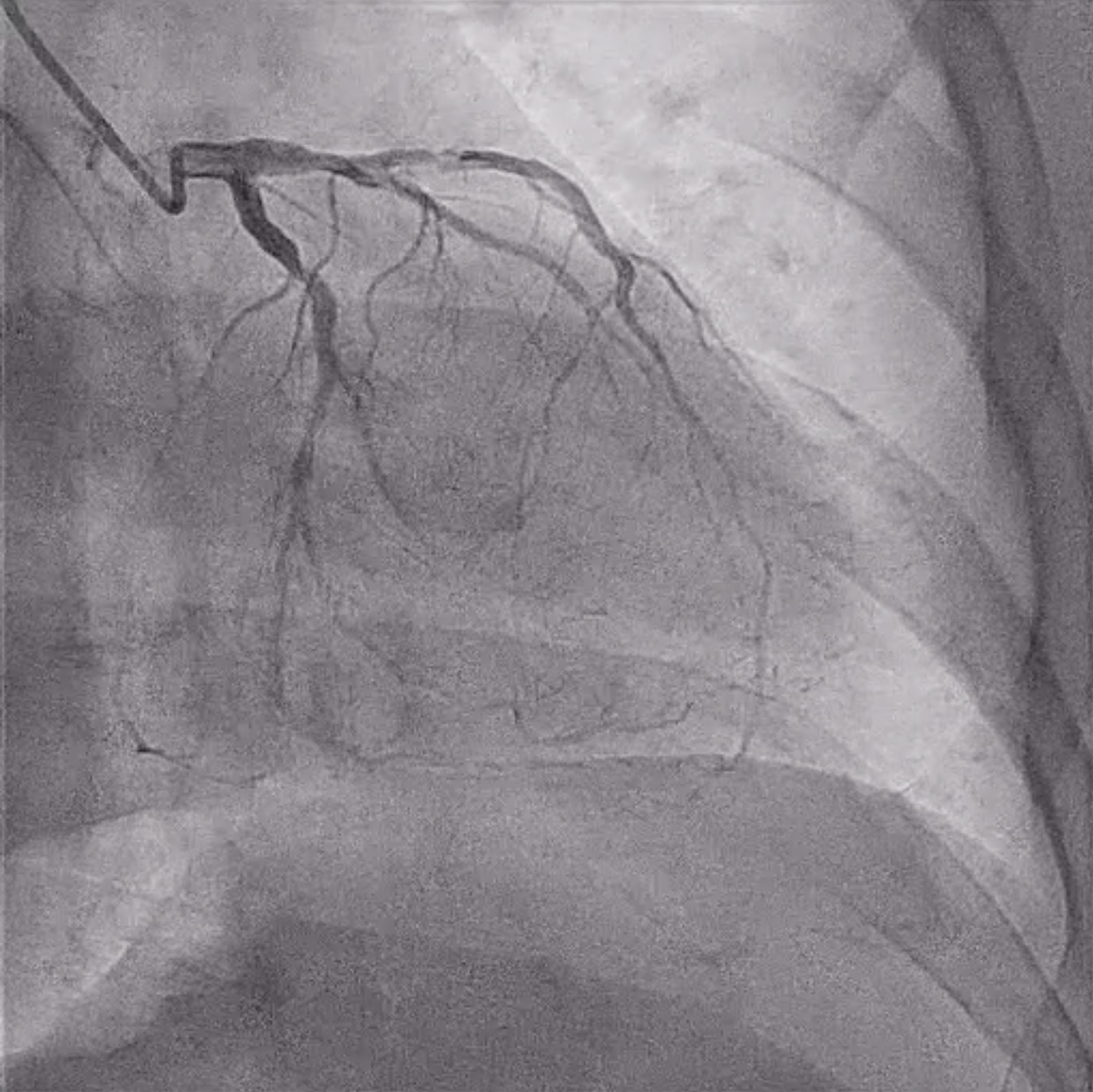
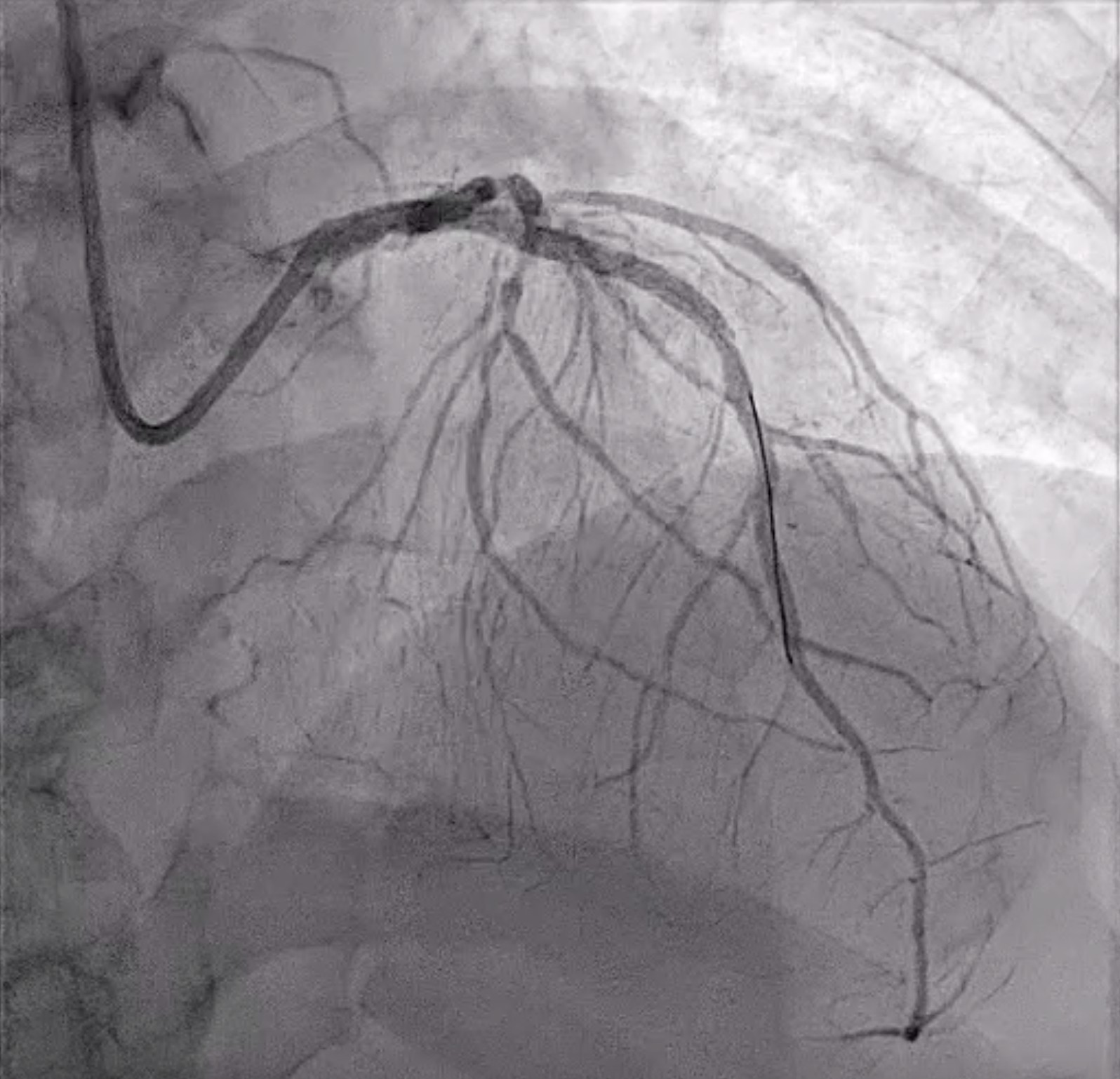
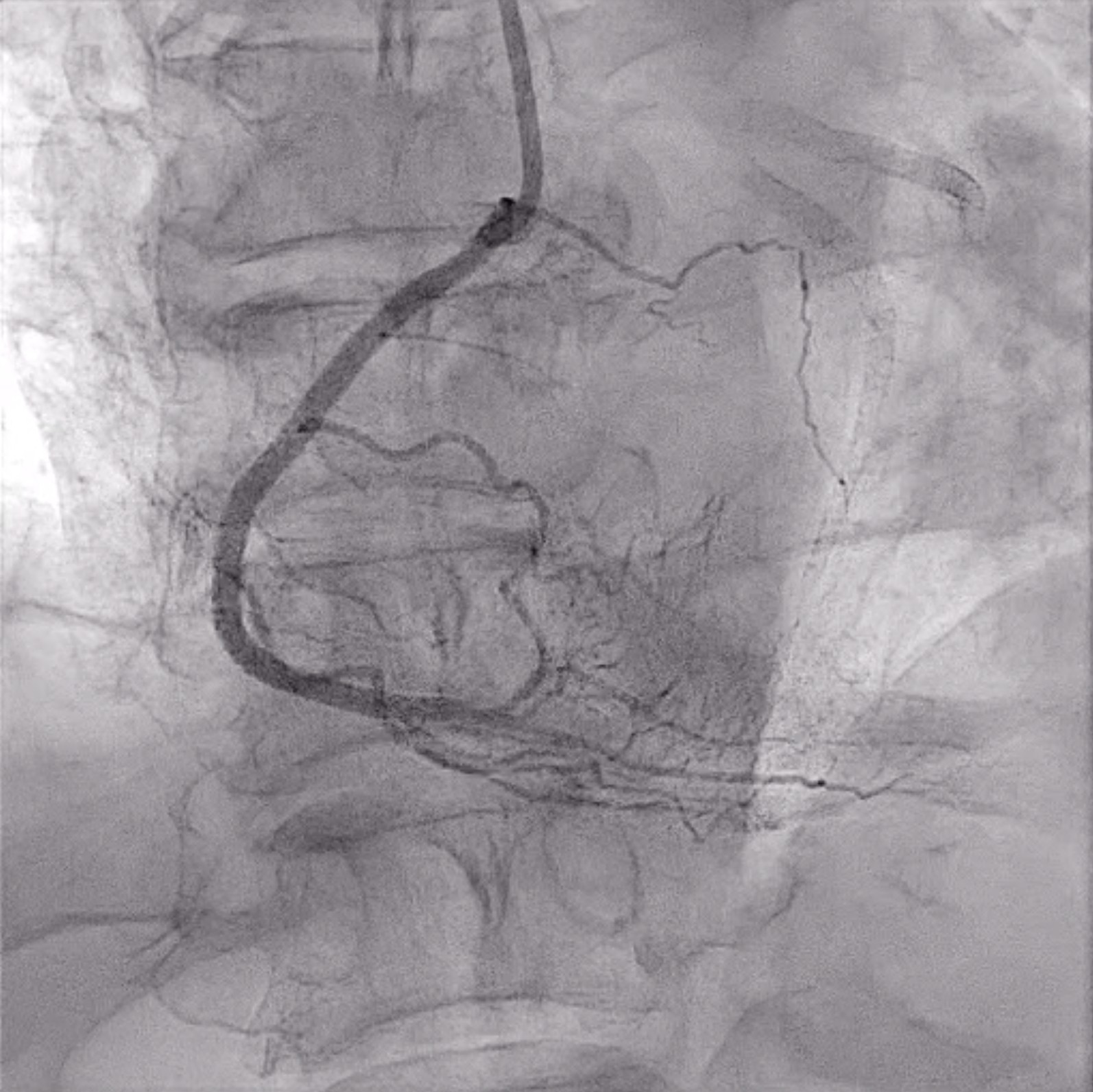
Relevant Catheterization Findings
The left main coronary artery has a non-significant stenosis at the distal segment.
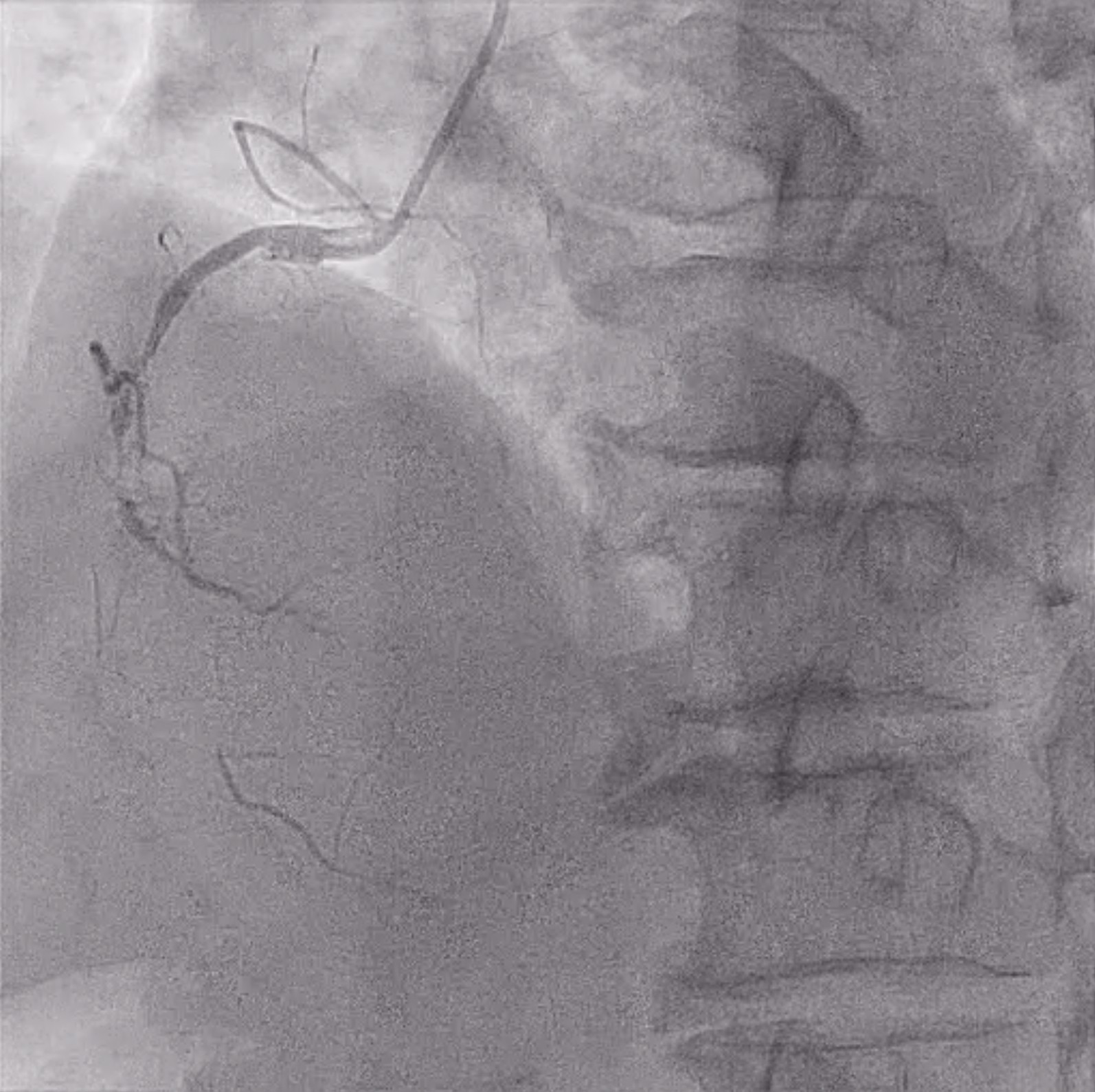
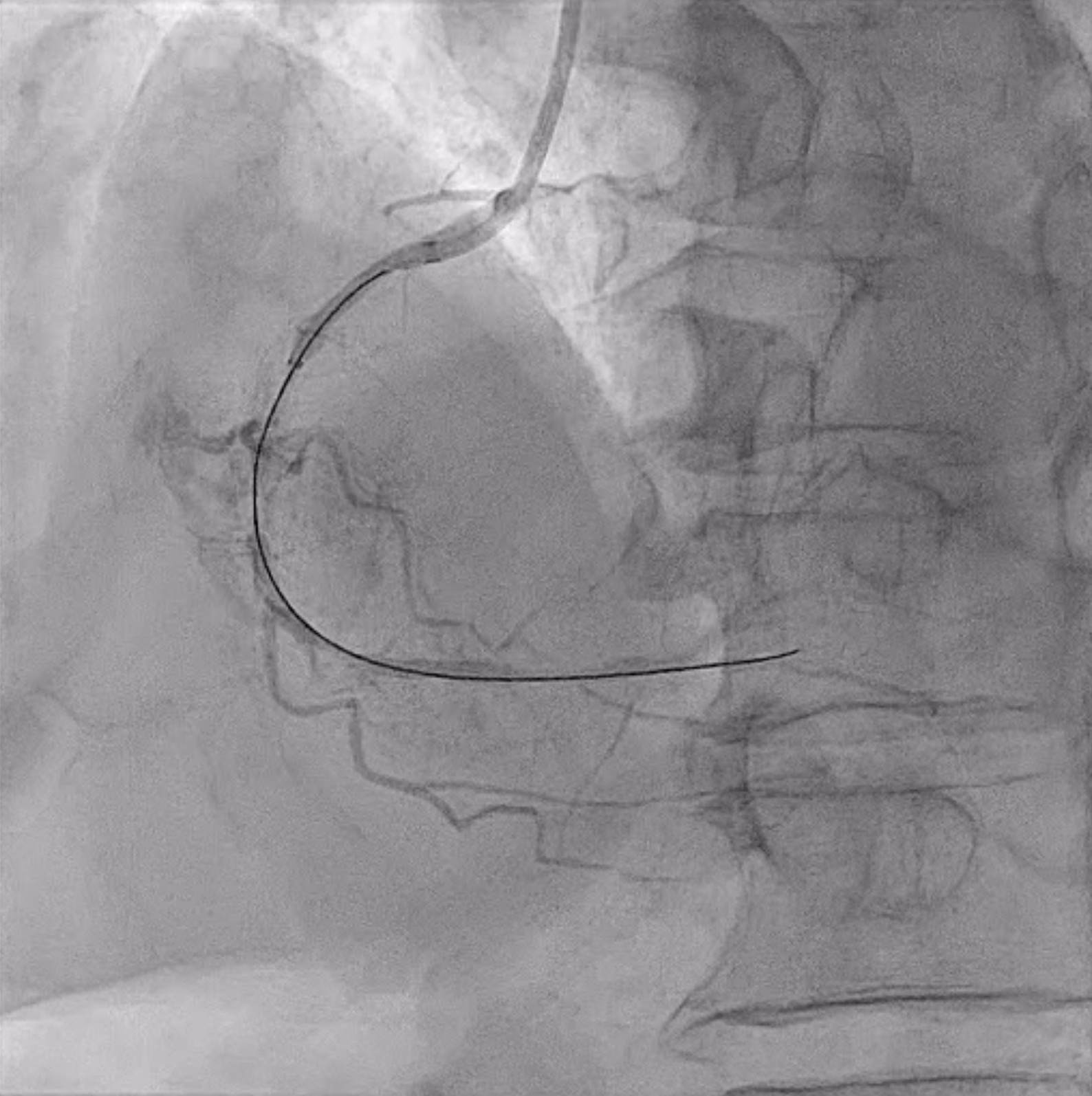
Interventional Management
Procedural Step
PCI OF LAD
Case Summary
Coronary artery perforations and dissections are rare but life-threatening complication of percutaneous coronary intervention. Several risk factors increase the risk of these complications such as chronic total occlusion, old age, diabetes and long lesions. All of these are present in our patient.