
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-062
Single Lumen Microcatheter Facilitated Reverse Guidewire Technique for Bifurcation Angioplasty
By Amjad Ali, Dileep Kumar Tiwari
Presenter
Amjad Ali
Authors
Amjad Ali1, Dileep Kumar Tiwari2
Affiliation
Sagar Multispeciality Hospital, India1, Baderiya Metroprime Hospital, India2,
View Study Report
TCTAP C-062
CORONARY - Bifurcation/Left Main Diseases and Intervention
Single Lumen Microcatheter Facilitated Reverse Guidewire Technique for Bifurcation Angioplasty
Amjad Ali1, Dileep Kumar Tiwari2
Sagar Multispeciality Hospital, India1, Baderiya Metroprime Hospital, India2,
Clinical Information
Patient initials or Identifier Number
AA
Relevant Clinical History and Physical Exam
A 64-year-old Asian man presented with acute onset severe retrosternal chest pain of three hours duration associated with profuse sweating. He was a known case of coronary artery disease and underwent CABG in 2014 (Two grafts LIMA to LAD, left radial to OM1). He is a known case of diabetes mellitus and hypertension and was on optimal medical treatment. His pulse was 60/minute and his blood pressure was 100/60 mmHg.
Relevant Test Results Prior to Catheterization
The patient’s electrocardiogram revealed sinus rhythmwith inferior ST-segment elevation. Bedside echocardiogram revealed basal andmid inferior and posterior wall hypokinesia with mild mitral regurgitation. His LV ejection fraction was 45%.
Relevant Catheterization Findings
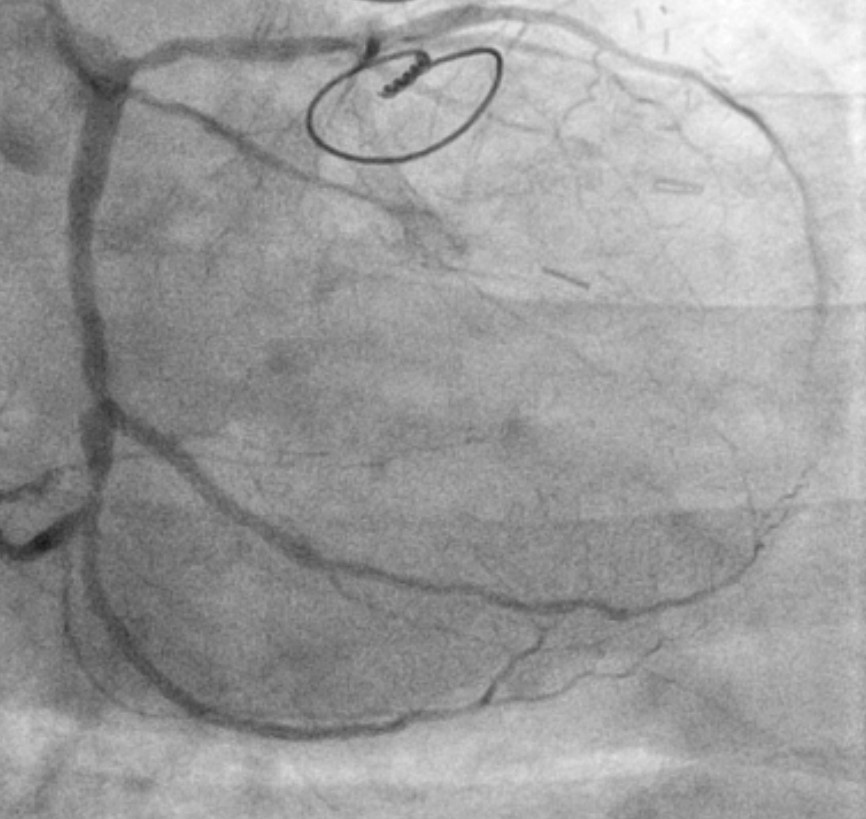
Coronary angiogram showed patent LIMA to LAD graft, Atretic left radial to OM2 graft which was the culprit vessel. RCA was non-dominant and small vessel.
Interventional Management
Procedural Step
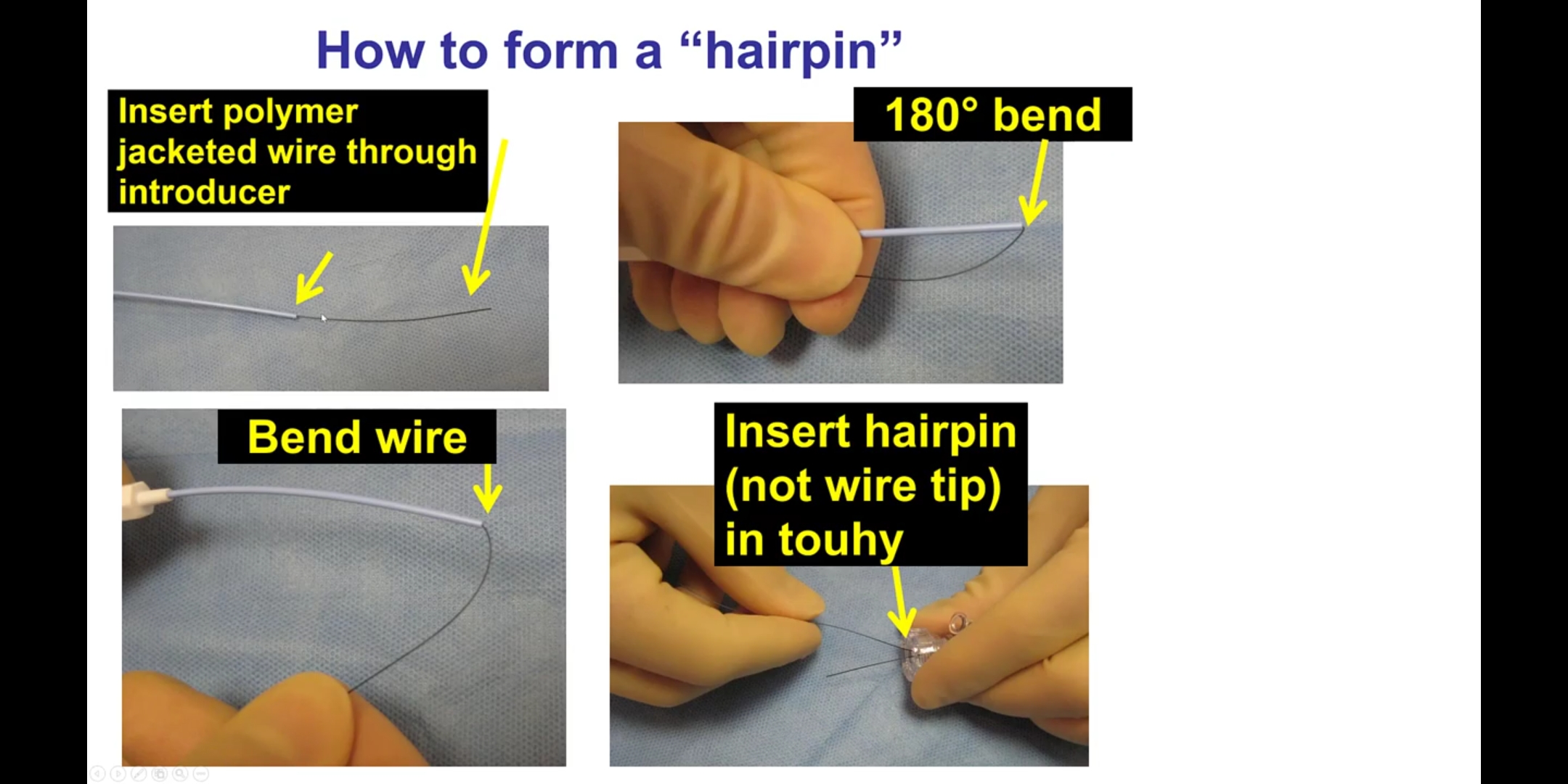
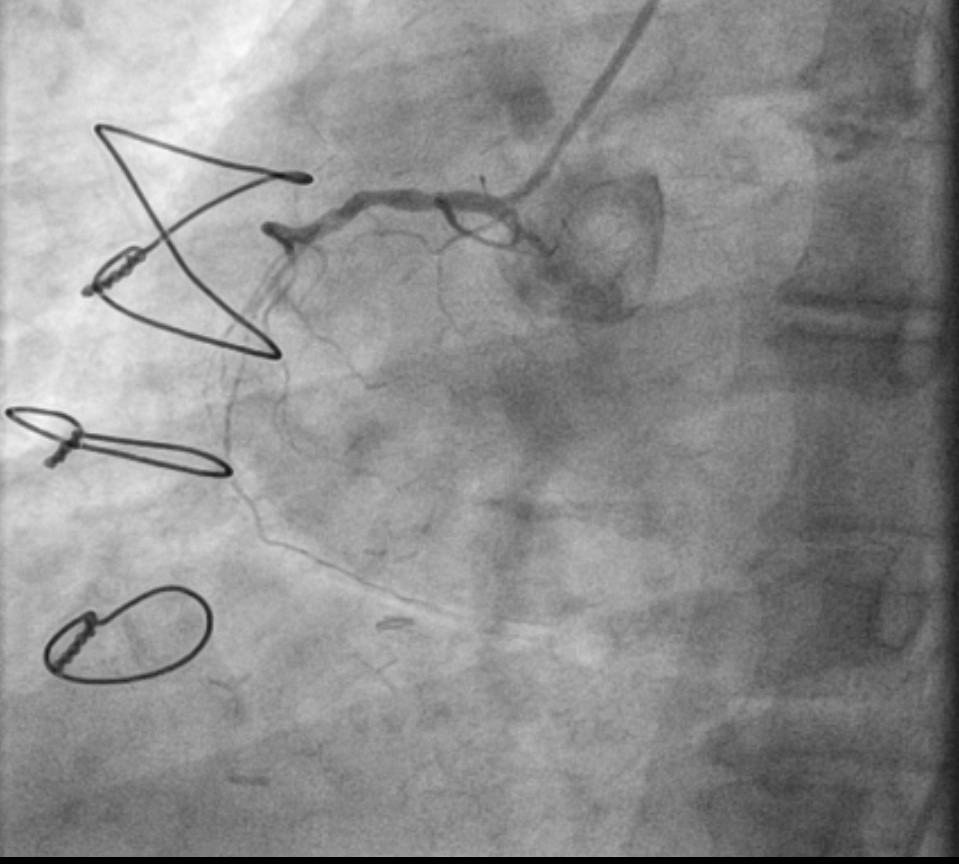
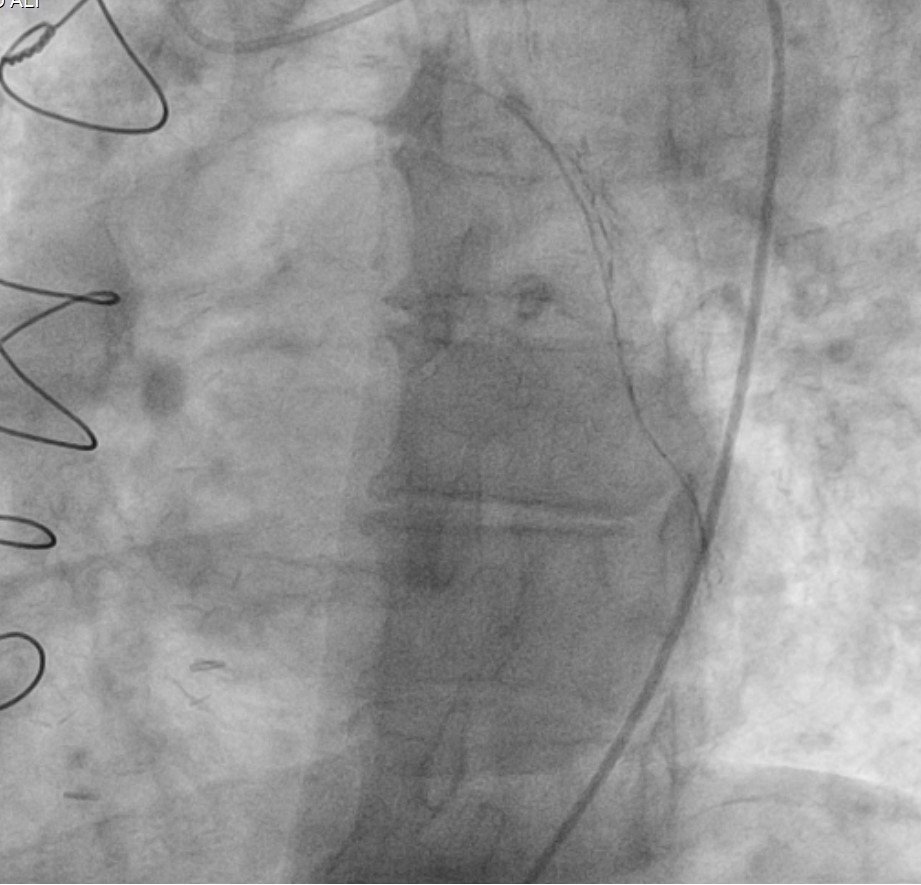
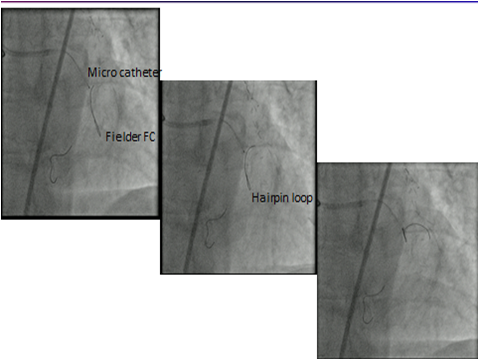
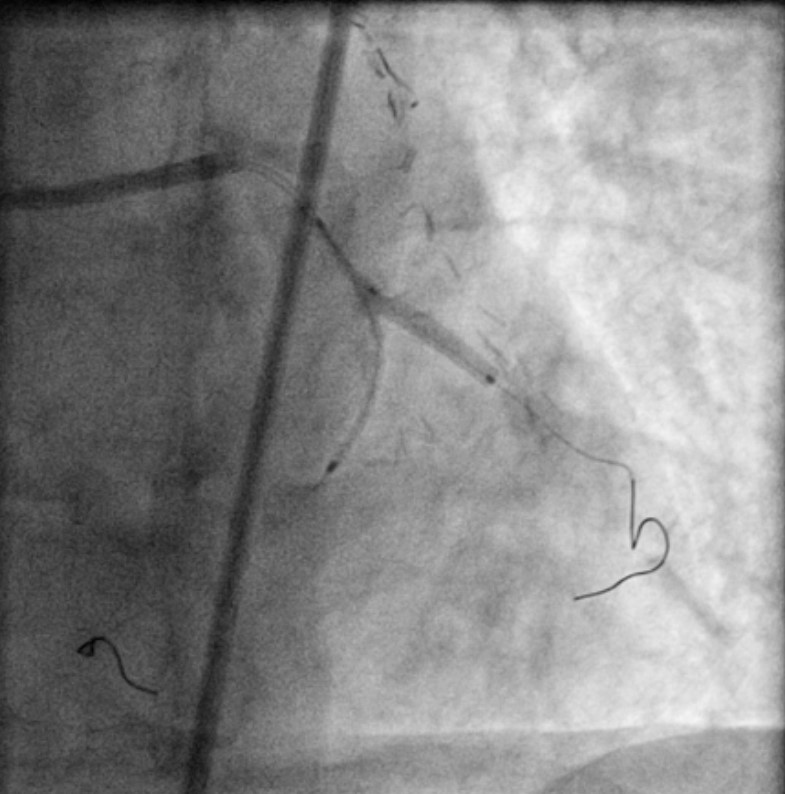
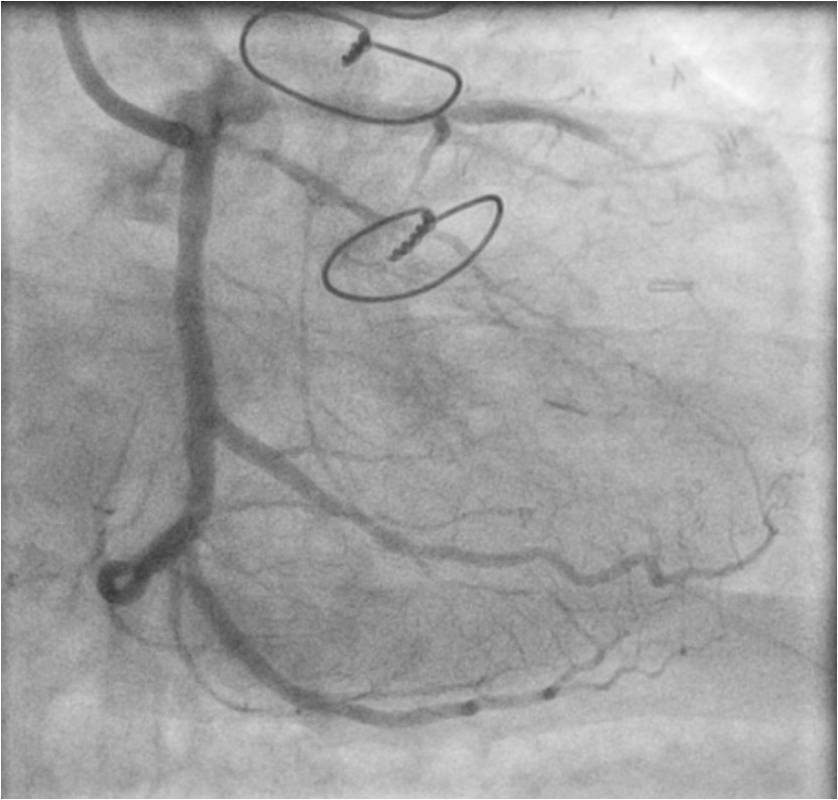
The patient was planned for LCX/OM2 bifurcation stenting with two drug-eluting stents (mini crush). The first wire was parked at distal LCX, wiring of OM2 was very difficult due to the very obtuse angle. After giving several attempts with different wires even by making a large C shape, we failed to cross the lesion. So we opted for the reverse guidewire/hairpin loop method. We used a fine cross microcatheter and fielder FC guidewire to make a hairpin loop and directed this loop to be parked in the distal branch. We kept the orifice of the microcatheter at the origin of the branch and gently pulled back the wire(hairpin loop). While pulling back the wire, It quickly crossed the markedly angulated side branch and made our further procedure very easy. The further procedure was done by the deployment of two DES by mini crush bifurcation stenting followed by final kissing balloon inflation and proximal optimization.
Case Summary
Discussion/Conclusion: Wiring of markedly angled side branches can be done by