
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-171
Hypoxic Ischemic Encepahalopathy After an Out-Of-Hospital-Cardiac Arrest Following a Case of Brugada Syndrome
By Huzairi Sani, Muhammad Hanis Muhmad Hamidi, Khairul Shafiq Ibrahim, Ahmad Bakhtiar Md Radzi, Rizmy Najme Khir, Hafisyatul Aiza Zainal Abidin, Sazzli Kasim
Presenter
Muhammad Hanis Muhmad Hamidi
Authors
Huzairi Sani1, Muhammad Hanis Muhmad Hamidi2, Khairul Shafiq Ibrahim2, Ahmad Bakhtiar Md Radzi2, Rizmy Najme Khir3, Hafisyatul Aiza Zainal Abidin2, Sazzli Kasim2
Affiliation
Hospital Pantai Klang, Malaysia1, Universiti Teknologi MARA (UiTM), Malaysia2, Ara Damansara Medical Centre, Malaysia3,
View Study Report
TCTAP C-171
OTHERS - Others (Unclassified)
Hypoxic Ischemic Encepahalopathy After an Out-Of-Hospital-Cardiac Arrest Following a Case of Brugada Syndrome
Huzairi Sani1, Muhammad Hanis Muhmad Hamidi2, Khairul Shafiq Ibrahim2, Ahmad Bakhtiar Md Radzi2, Rizmy Najme Khir3, Hafisyatul Aiza Zainal Abidin2, Sazzli Kasim2
Hospital Pantai Klang, Malaysia1, Universiti Teknologi MARA (UiTM), Malaysia2, Ara Damansara Medical Centre, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Mr S
Relevant Clinical History and Physical Exam
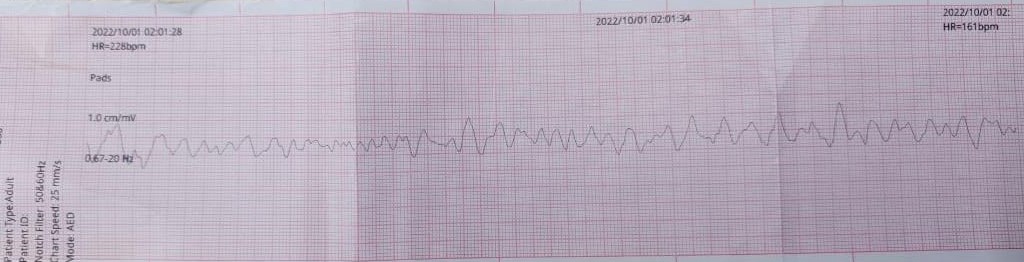
A fit and healthy 29-year-old businessman with no past medical history was found unresponsive at home at 130a.m. His father heard abnormal breathing in the living room and found him unconscious. He was in a generalized tonic state with closed eyes. Cardiopulmonary resuscitation (CPR) was immediately commenced and continued throughout the journey to the hospital. He was intubated and CPR downtime was 45 minutes. Total of 6 shocks were delivered.
Relevant Test Results Prior to Catheterization
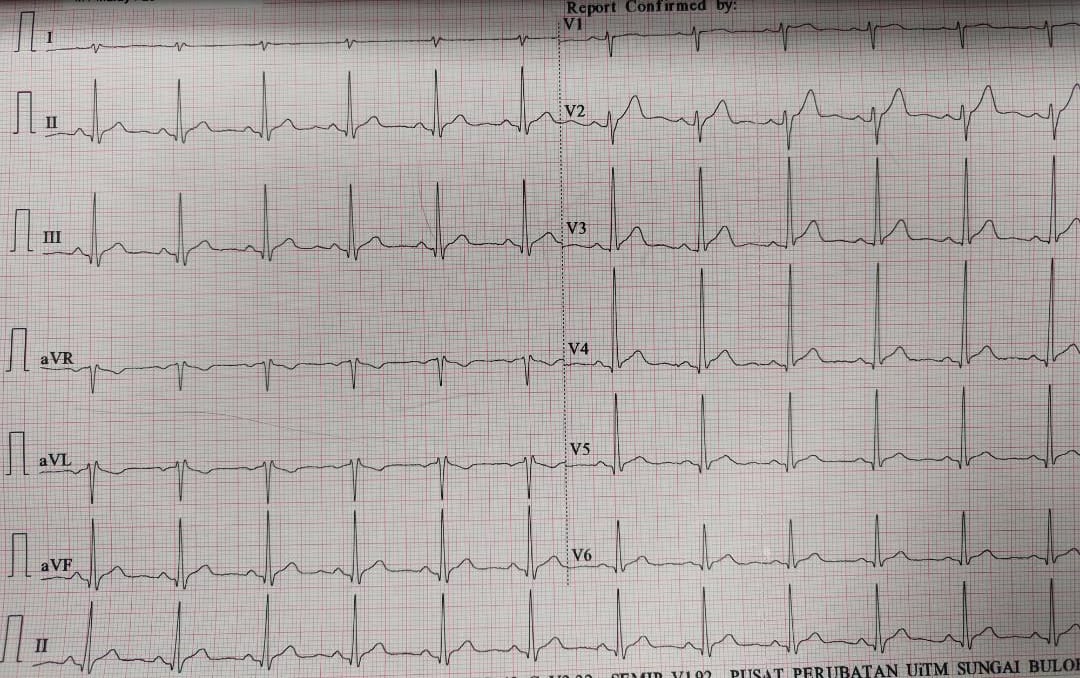
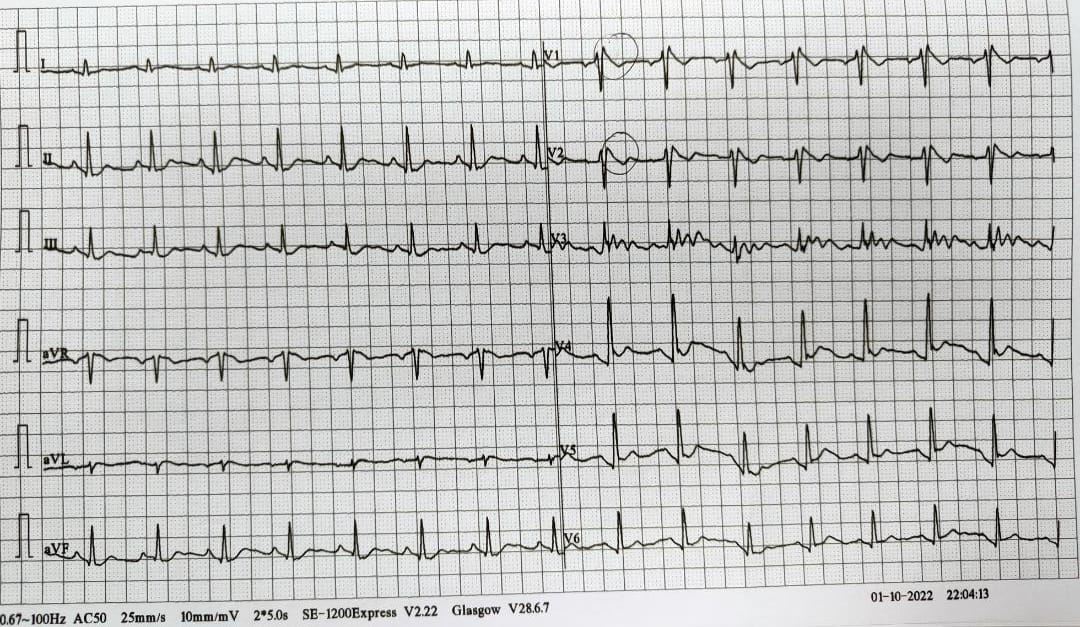
Haemoglobin 15.4, Creatinine 112 mmol/L. Cardiac MRI showed no significant abnormality. CT brain reported as diffuse enhancement of the cerebral sulci. Diffuse loss of grey-white matter differentiation. Decreased attenuation of the basal ganglia bilaterally. These features are suggestive of hypoxic ischemic injury. High leads ECG (lead V1 and V2 at 2nd intercostal space while lead V3 between V2 and V4) revealed coved ST-segment elevation >2mm in V1 and V2 followed by a negative T-wave.
Relevant Catheterization Findings
Interventional Management
Procedural Step
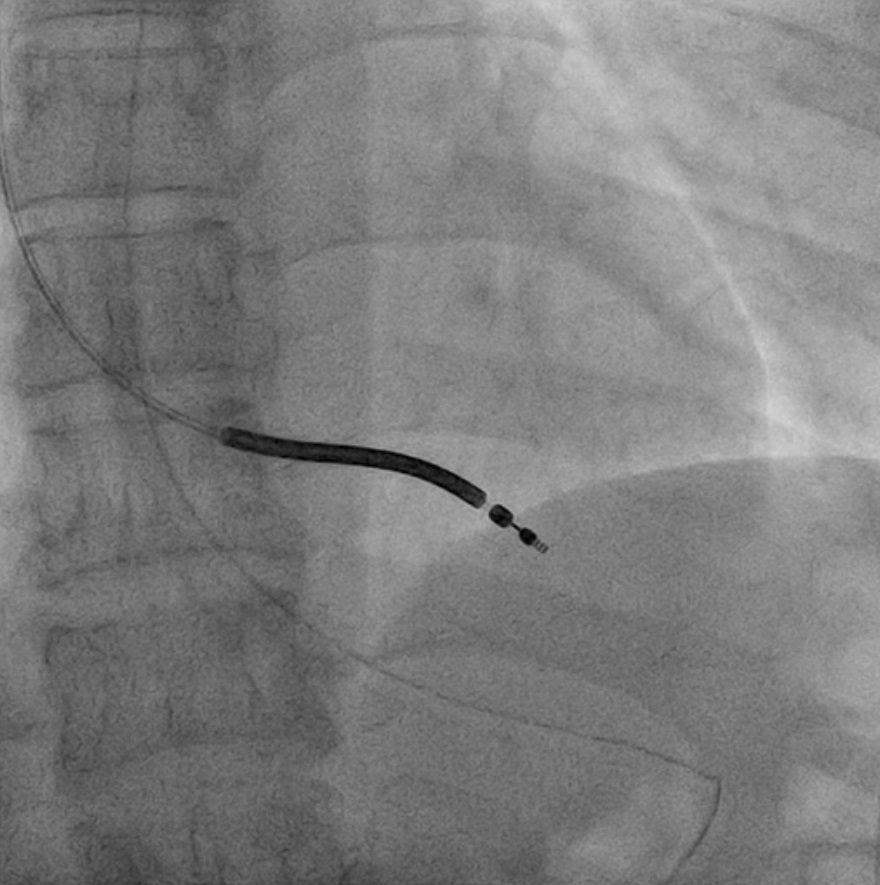
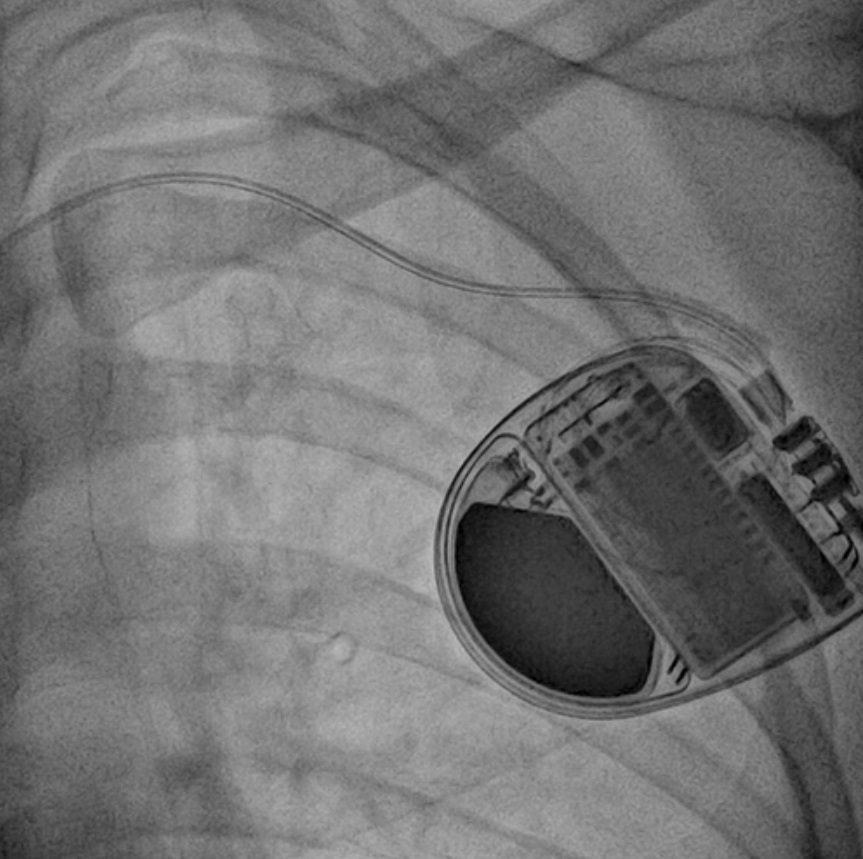
Left axillary venogram performed prior to the area being cleaned and draped. 40cc of lignocaine administered subcutaneously for local anaesthesia. Skin incision made along the deltopectoral groove. Dissection of subcutaneous layers to reach the fascia layer by using diathermy. Approached by left axillary vein access. RV lead was inserted and placed at the apex. The RV threshold was at 0.50 V and the RV pulse width was 0.4ms. Visia AF MRI XT ICD was implanted in a pocket. Fascia and subcutaneous later closed using interrupted suture technique. The skin later closed by continuous technique. The setting was VVI mode.

Case Summary
Brugada syndrome has been recognized as an important cause of sudden cardiac death in young men, especially in Southeast Asia. Symptomatic treatment with implantable cardioverter defibrillators (ICDs) is the mainstay in the prevention of sudden cardiac death. We presented a case of a fit young gentleman who survived out-of-hospital cardiac arrest and received cardiopulmonary resuscitation (CPR) but unfortunately developed hypoxic ischemic encephalopathy. Education and lifestyle measures for the prevention of arrhythmia events are crucial. We would like to highlight the importance of high-quality CPR by family members or outsiders is key to preventing neurological complications.