
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-145
Numerous Difficulties to Stent in Tortuous and Calcified ICA
By Hao Yun Lo, Jen-Kuang Lee
Presenter
Hao Yun Lo
Authors
Hao Yun Lo1, Jen-Kuang Lee2
Affiliation
National Taiwan University Hospital Hsin-Chu Branch, Taiwan1, National Taiwan University Hospital, Taiwan2,
View Study Report
TCTAP C-145
ENDOVASCULAR - Carotid & Neurovascular Intervention
Numerous Difficulties to Stent in Tortuous and Calcified ICA
Hao Yun Lo1, Jen-Kuang Lee2
National Taiwan University Hospital Hsin-Chu Branch, Taiwan1, National Taiwan University Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
LHY
Relevant Clinical History and Physical Exam
Thisis a 69-year-old woman had medical history of peripheral arterial diseasestatus post percutaneous transluminal angioplasty to right common iliac artery,left common femoral artery, left popliteal artery, and innominate artery during2019 to 2020. She also had right middle cerebral artery infarction in 2019.Other underlying diseases included hypertension, dyslipidemia, diabetesmellitus, hypothyroidism, coral reef aorta, and chronic kidney disease stageIIIb.


Relevant Test Results Prior to Catheterization
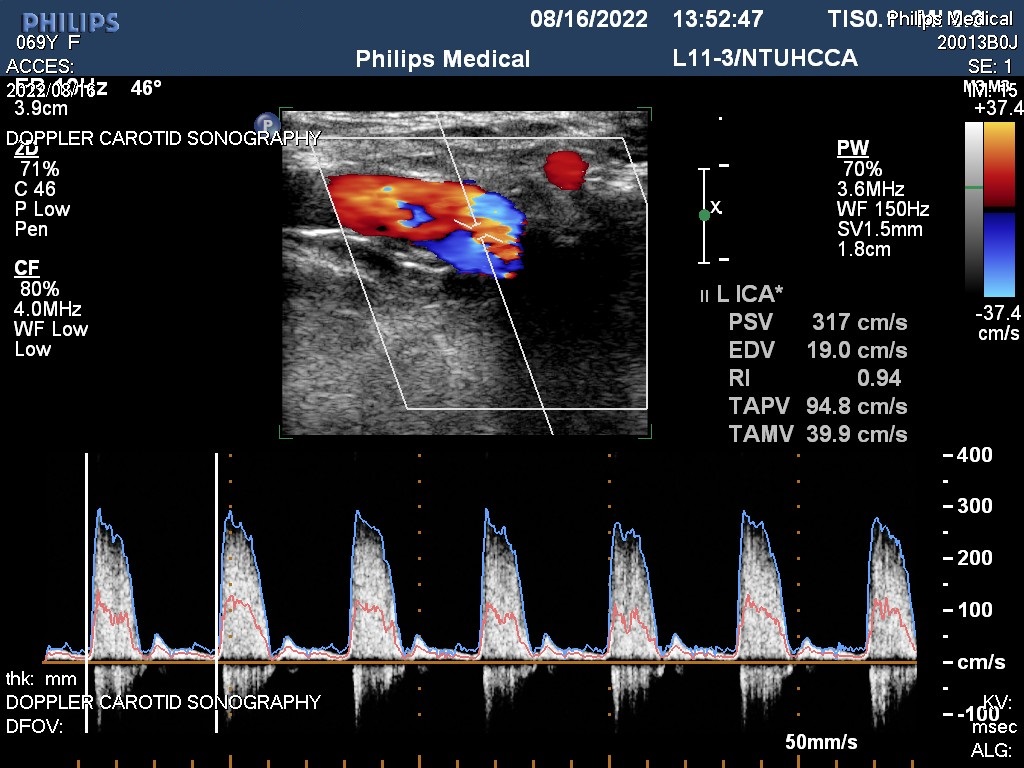
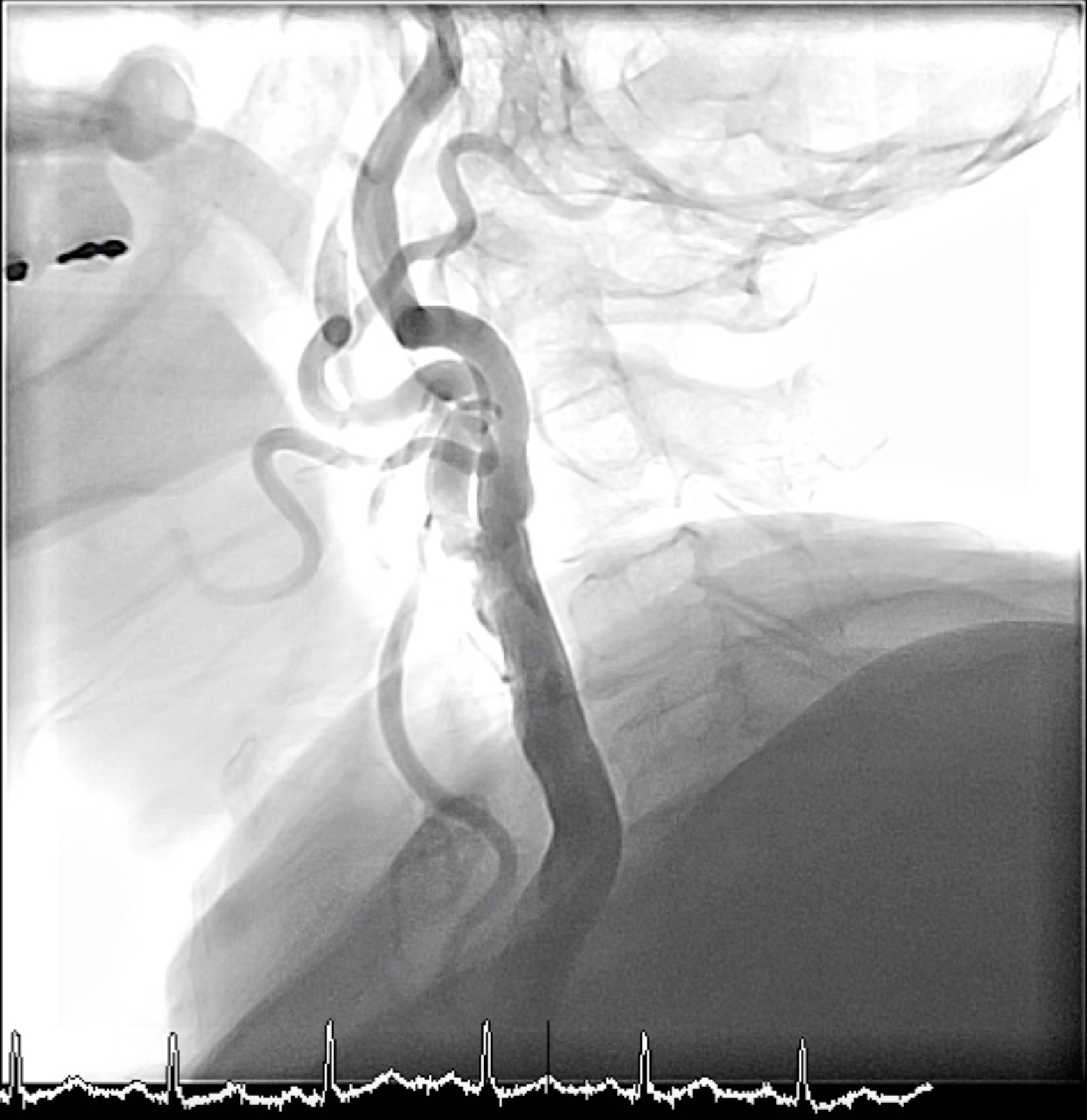
She suffered from dizziness since June2022. The carotid doppler showed left internal carotid artery > 70%stenosis, with high flow velocity (peak systolic velocity = 317 cm/s and enddiastolic velocity = 19 cm/s). She took clopidogrel and cilostazol for years.The LDL level was 40 mg/dL with statin treatment and HbA1c was 6.0%. In thiscondition, she was admitted for carotid angiography and percutaneoustransluminal angioplasty.
Relevant Catheterization Findings
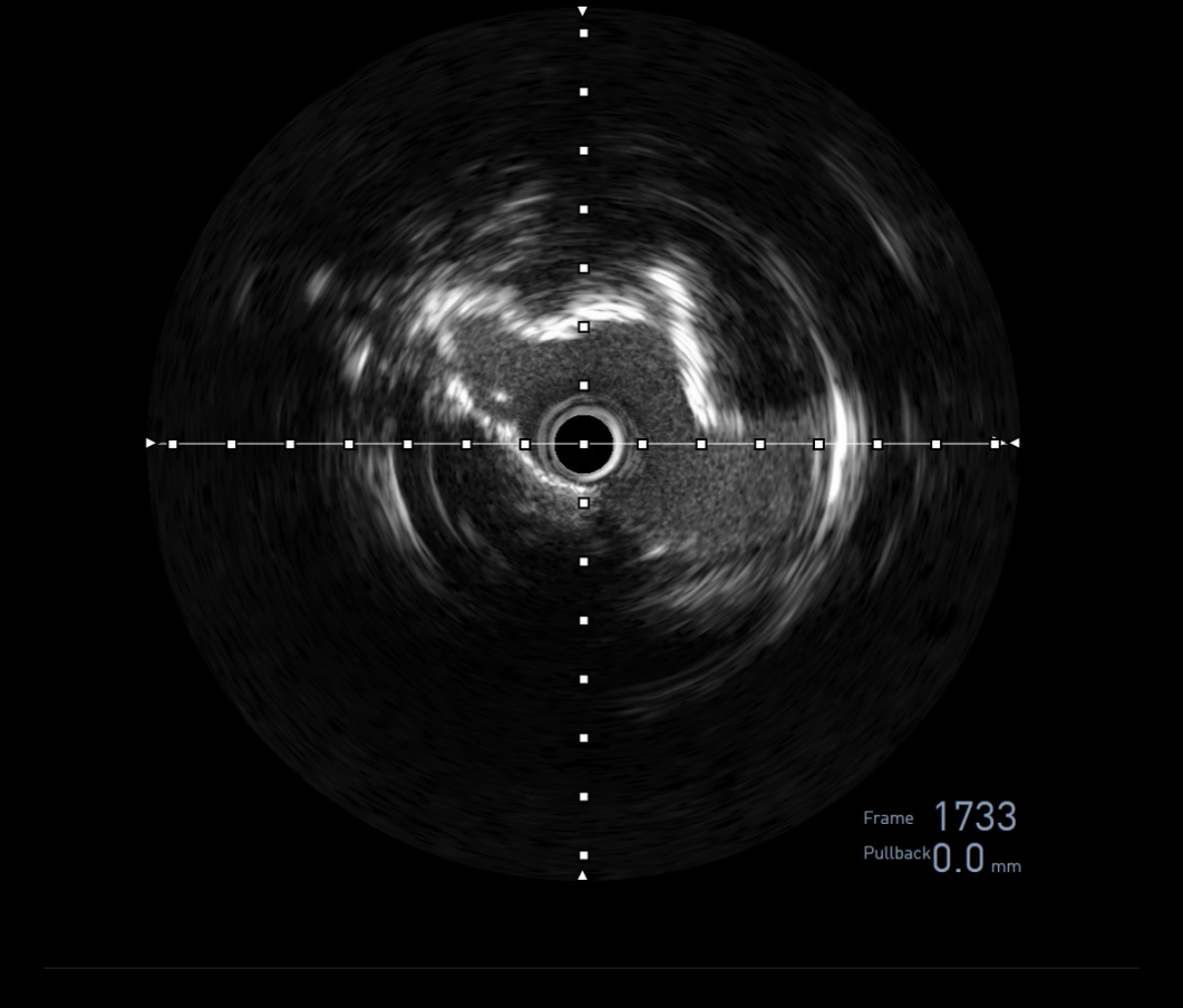
- Right innominate artery: in-stent restenosis 80%- Right common carotid artery: distal stenosis 40%- Right internal carotid artery: patent- Right external carotid artery: 80% stenosis- Left common carotid artery: ostial 50% stenosis- Left internal carotid artery: 80% stenosis * IVUS showed severe stenosis eccentric calcification- Left external carotid artery: patent- Left vertebral artery: proximal total occlusion


Interventional Management
Procedural Step
1. Approached through rightfemoral artery with 8 Fr sheath.
Case Summary
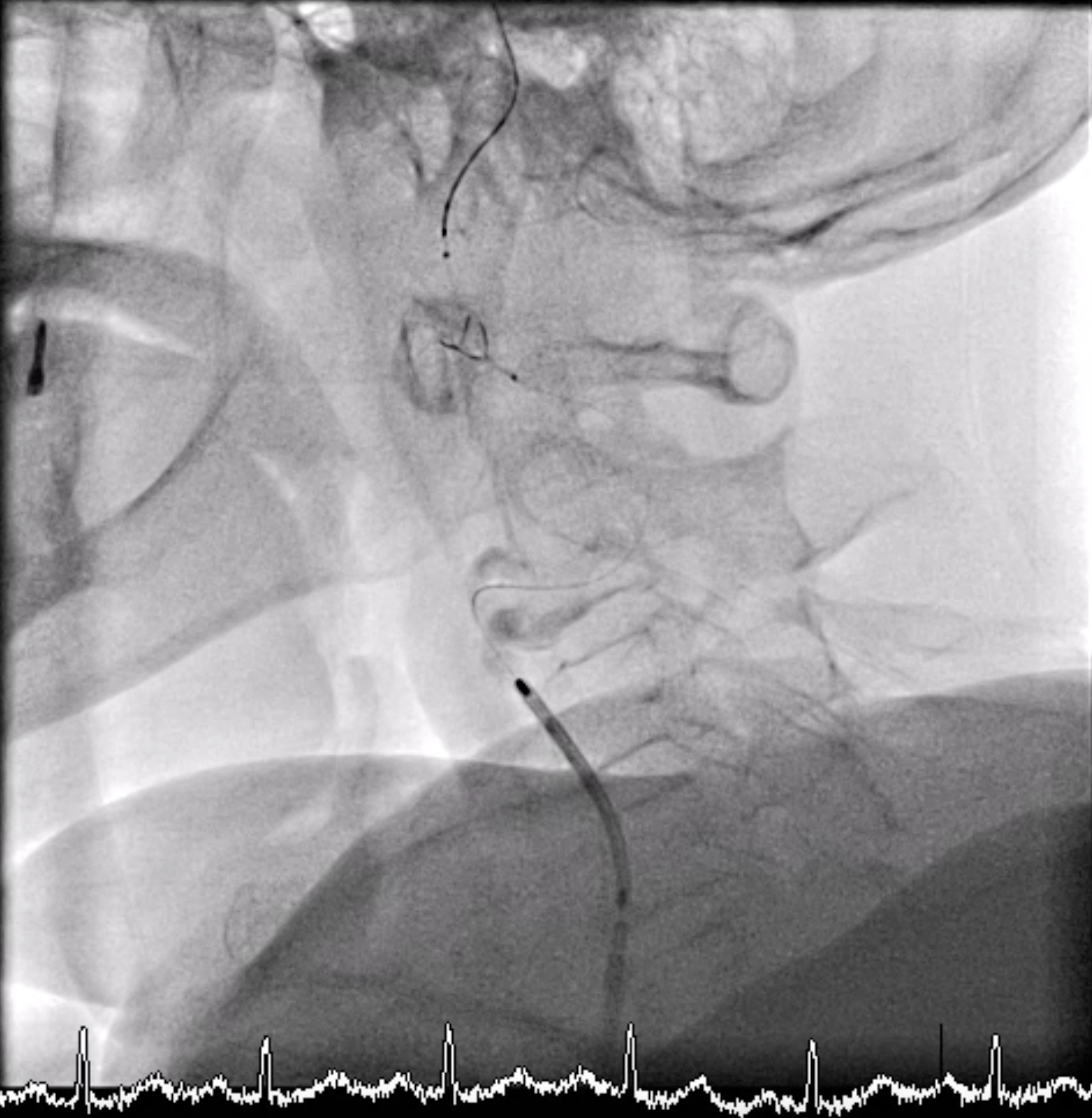
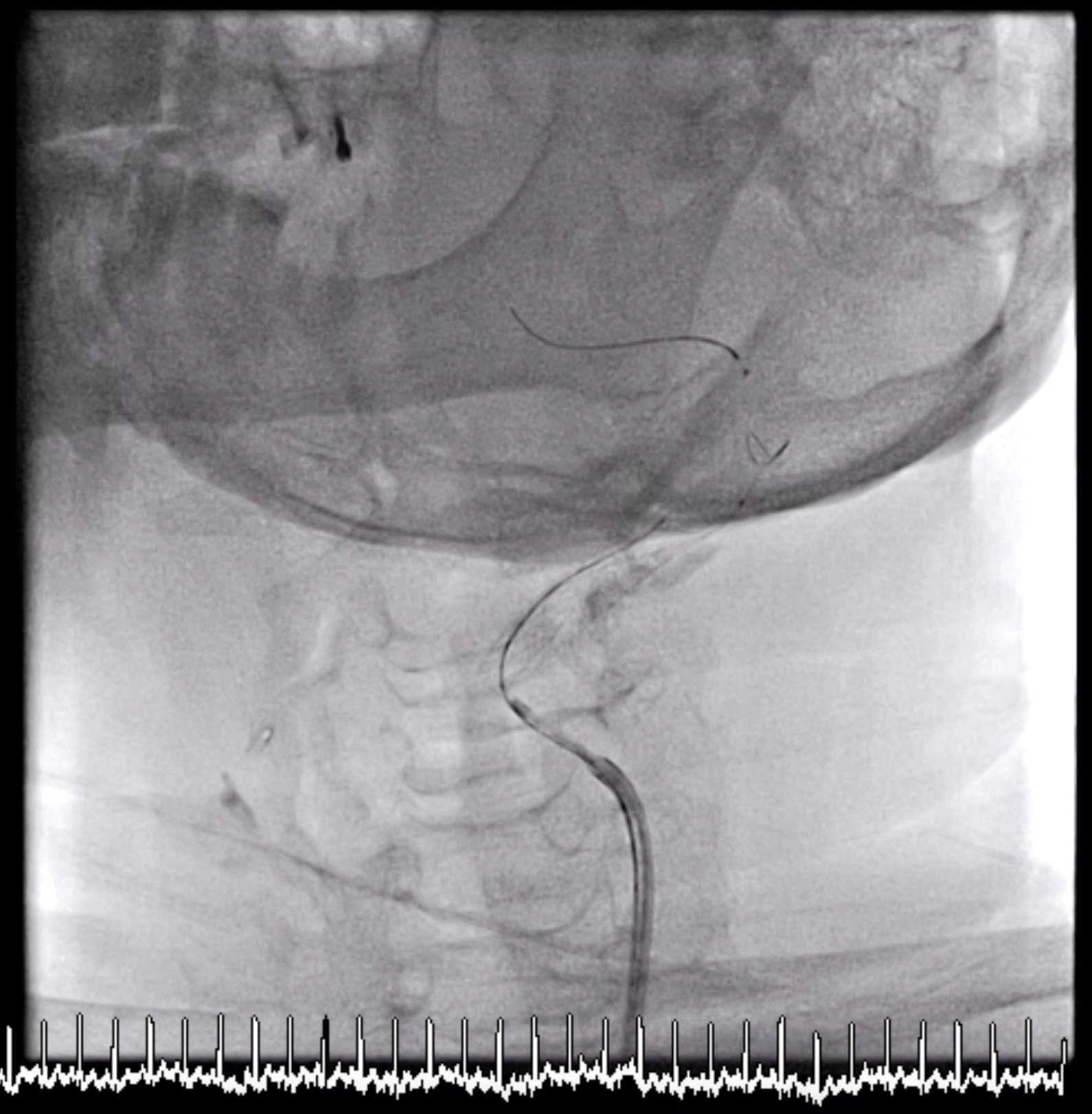
Incarotid intervention, there is high risk of stroke in difficult devicedelivery. In our case, the difficulty caused from coral reef aorta and tortuousleft ICA. Tortuous ICA is more difficult to overcome than tortuous coronary.First, there is less support for guiding catheters from the aorta. Second,there is no vessel could be anchored. We use long sheath (Terumo Guide sheathTM 8F45cm Straight) to decrease resistance resulting from coral reef aorta anduse another wire to make tortuous ICA straight. Finally, we use these methodsto make whole system stable, and complete the procedure smoothly.